Download presentation
Presentation is loading. Please wait.

1
Pediatric surgery Clinical practice DR. Bassam Al-Abbasi

2
الصور من الدكتور الشرح من كتابة الطلاب

3
Head and Neck

4
Cleft lip and palate Problems: Aspiration during feeding Nasal speech Cosmetic problems Affect the hearing (glue ear) Lead to recurrent chest infection Surgery: In 6 months to 1 year for cleft palate In 3 months for cleft lip Feeding: Use special bottle tit In setting position
 Lead to recurrent chest infection Surgery: In 6 months to 1 year for cleft palate In 3 months for cleft lip Feeding: Use special bottle tit In setting position")
5
Cleft lip repair (cheiloplasty)
")
7
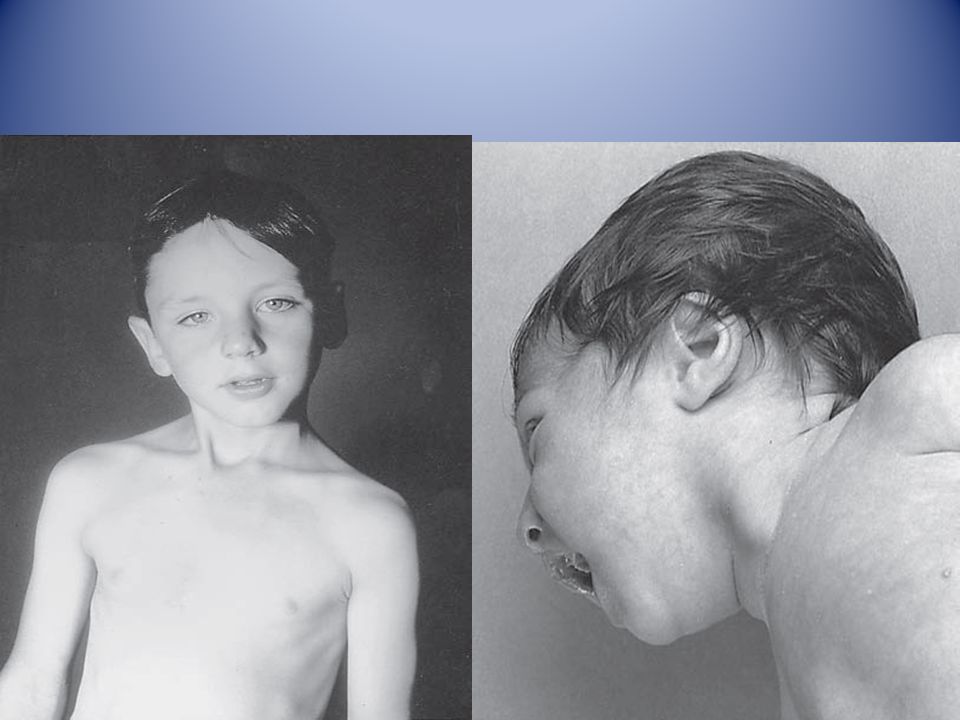
First photo: Diagnosis: thyroglossal cyst Problems: Lead to infection Lead to fistula Could convert to malignancy Need surgery remove the fistula tract + remove the hyoid bone to prevent recurrance Second photo: Diagnosis: cystic hygroma Notes: It is due to lymphatic obstruction Common at the sites of communication between the trunk and the extremities like cervical region, axilla, groin. Treatment: By surgery: it depends on presence of complications like compression, infection bleeding (rapid increase in size and become pale and shock) During surgery be careful to some nerves like hypoglossal never, spinal accessory nerve, mandibular branch of facial nerve
 During surgery be careful to some nerves like hypoglossal never, spinal accessory nerve, mandibular branch of facial nerve.")
10
Diagnosis: sternocleidomastoid torticollis (first photo) sternocleidomastoid mass (second photo) Notes: Ask about breech presentation and obstructed labor If not treat the mass it could be converted to torticollis Treatment of mass is by physiotherapy by twisting the chin and movement of ear and massage 90% will disappear if not treated do surgery by cutting the mass and muscle. Treatment of torticollis is by surgery.

12
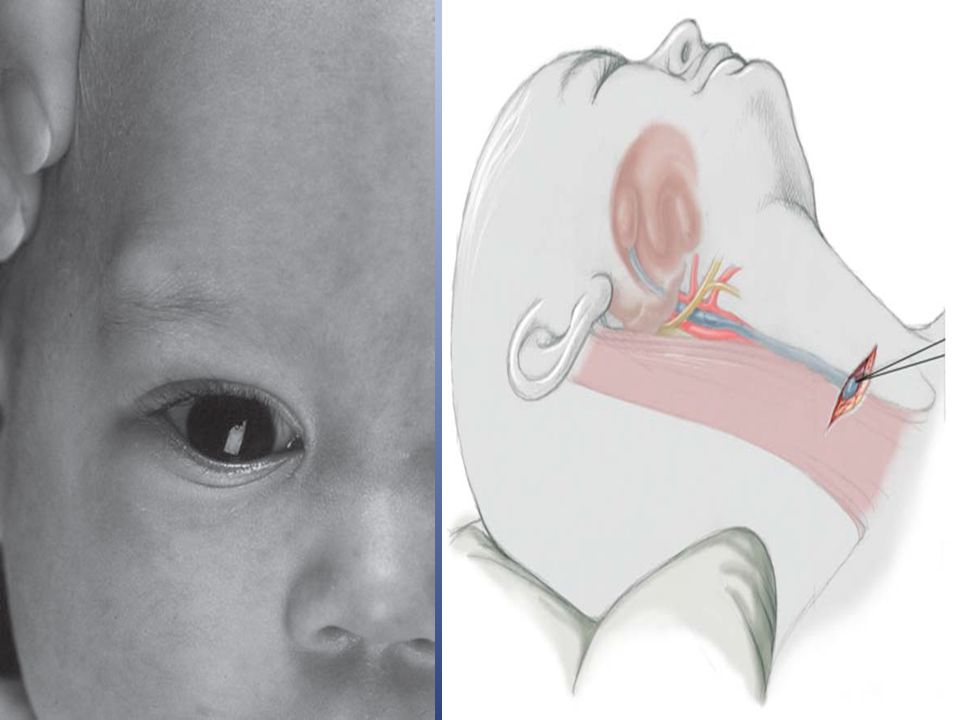
First photo: Diagnosis: External angular dermoid Notes: Treated by surgery excision and complete remove Problems infection, trauma, cosmetic Second photo: Diagnosis: remnant of second branchial arch branchial cyst or fistula Site: anterior border of sternocleidomastoid muscle between tonsil and lower two third of sternocleidomastoid muscle Problems: infection – malignancy Treatment: surgery (excision)
")
13
The Umbilicus

14
First photo: Diagnosis: umbilical hernia Treatment: could resolve spontaneously or by surgery Second photo: Omphalo-mesenteric duct connection between umbilicus and bowel

16
Diagnosis: Michaels diverticulum Role of 2: 2% of population. 2 type of mucosa(ectopic gastric mucosa). 2 feet from iliocecal valve. 2 inches in lengthe. Presentation: Bleeding per rectum (painless – bright red – profuse) Infection (lead to abdominal pain) Complication intestinal obstruction, volvulus, intussusception Incidental finding Diagnosis: Use isotope (bind to gastric tissue (parietal cell) within the mechaels) Laparoscope (diagnostic and therapeutic)
. 2 feet from iliocecal valve. 2 inches in lengthe. Presentation: Bleeding per rectum (painless – bright red – profuse) Infection (lead to abdominal pain) Complication intestinal obstruction, volvulus, intussusception Incidental finding Diagnosis: Use isotope (bind to gastric tissue (parietal cell) within the mechaels) Laparoscope (diagnostic and therapeutic).")
17
Vomiting in the First Months of Life

18
Diagnosis: pyloric stenosis Presentation: Projectile vomiting (not present in first two weeks) Olive mass in the abdomen Positive prestalsis FTT Diagnosis: Clinically Ultrasound Ba-meal dilated stomach – failure to pass to intestine – string sign Treatment: surgery pyloromyotomy (rami stick surgery)
 Olive mass in the abdomen Positive prestalsis FTT Diagnosis: Clinically Ultrasound Ba-meal dilated stomach – failure to pass to intestine – string sign Treatment: surgery pyloromyotomy (rami stick surgery)")
20
Diagnosis: achalasia cardia Presentation: Hailtosis Vomiting (not projectile) Wheezing Chest infection Ba-swallow dilatation of esophagus with narrowing of lower part. Treatment cardiomyotomy

21
The Child with an Abdominal Mass

22
5 years child, presented with mass in the flank. DDx of mass in the flank: 1- Wilms tumor 2- Neuroblastoma 3- Neglected PUJ obstruction Presentation: 1- Mass 2- hematuria 3- hypertension Treatment by surgery remove the kidney + chemotherapy

23
Neuroblastoma in the adrenal gland

25
Diagnosis: non-Hodgkin lymphoma Presentation: 1- Mass 2- Intussusception Investigation: FNA Treatment: surgery + chemotherapy (for one year)
")
27
Diagnosis: Sacro-coccygeal teratoma Problems: 1-obstructed labor 2- Malignancy (if neglected for 2-3 months) Treatment: surgery + remove the coccyx to prevent recurrence
 Treatment: surgery + remove the coccyx to prevent recurrence")
28
Spleen, Pancreas and Biliary Tract غير مطلوب

31
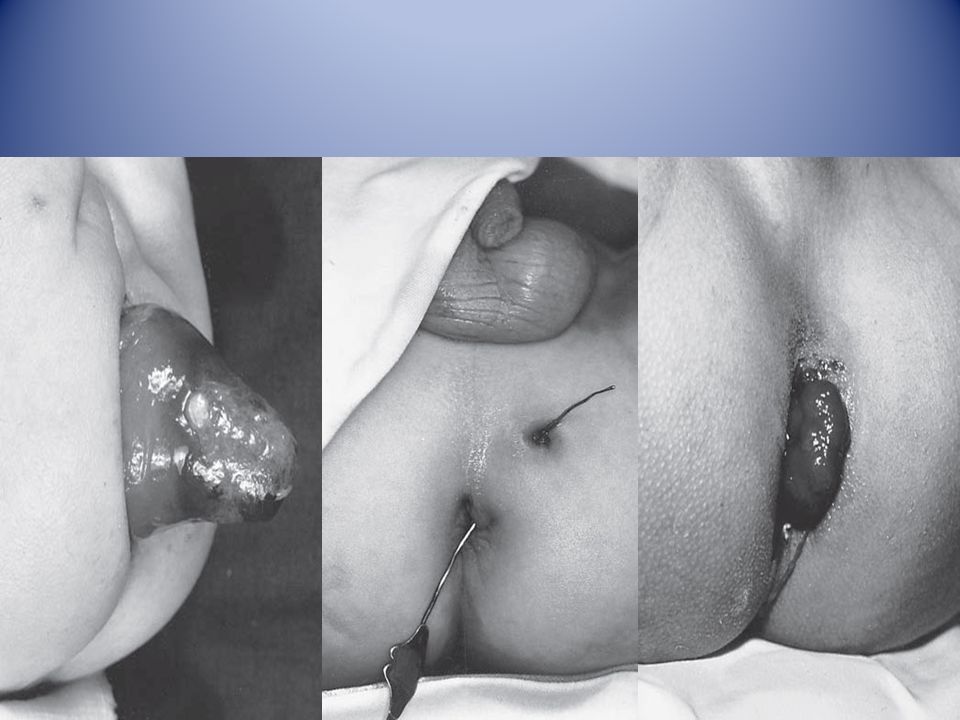
First photo: Diagnosis: rectal prolapse Causes: Constipation or diarrhea Weak pelvic muscles Worm (trichuris trichiura) Grades: Grade1 يطلع ويرجع conservative treatment by taping Grade2 يطلع ويحتاج الى دفع للدخول surgery (Therach operation) Grade3 يطلع وما يرجع ابد surgery (Therach operation) Second photo: Diagnosis: Perianal fistula Treatment: surgery (fistulectomy or fistulotomy) Third photo: Diagnosis: rectal polyp Cause in infection Red-bleed mass + bleeding per rectum Treatment: excision (use sigmoidoscope)
 Grades: Grade1 يطلع ويرجع conservative treatment by taping Grade2 يطلع ويحتاج الى دفع للدخول surgery (Therach operation) Grade3 يطلع وما يرجع ابد surgery (Therach operation) Second photo: Diagnosis: Perianal fistula Treatment: surgery (fistulectomy or fistulotomy) Third photo: Diagnosis: rectal polyp Cause in infection Red-bleed mass + bleeding per rectum Treatment: excision (use sigmoidoscope)")
32
Hernia Varicocele

34
Diagnosis: undescended testes Problems: Tumor Sterility Infection Orchitis (like appendicitis) Treatment: If palpable do fixation If not palpable do laparoscopy If not present do nothing
 Treatment: If palpable do fixation If not palpable do laparoscopy If not present do nothing")
35
غير مطلوب

37
ANY QUESTIONS

Similar presentations


























. Dysphagia Defn Difficulty in swallowing Classification 1- Oropharyngeal dysphagia Causes– Local pain -trauma, oral candida,>")

