Download presentation
Presentation is loading. Please wait.

1
Interesting case of GI bleed Dr Charles Panackel MD DM, Dr Sunil K Mathai MD, DM Department of Gastroenterology, Medical Trust Hospital, Kochi Presenting Author – Dr Sunil K Mathai, HOD Gastroenterology

2
History 56 year old female Admitted with ▫Hematemesis - 2 episodes ▫Malena - 3 episodes ▫Generalized weakness ▫Giddiness

3
Admitted to ICU Hemodynamically stable PR – 80 / min., BP – 140/70 mm Hg RT inserted – no fresh blood, coffee ground aspirate General examination – mild pallor + Systemic examination – no s/o liver disease ▫No contributory findings

4
Urgent Endoscopy

5
Ulceration with Adherent Clot in Mid Esophagus ? Aortoesophageal fistula

6
Flash Back

7
Fish bone in mid esophagus in 2005. Active oozing ++ -Referred to MTH

8
Flash Back CT Chest- Fish bone in mid esophagus piercing aorta Emergency Thoracotomy with aortic repair on 21/03/2005 Uneventful till date…. When she presented with GI bleed on 15/o6/2012

9
Back to case

10
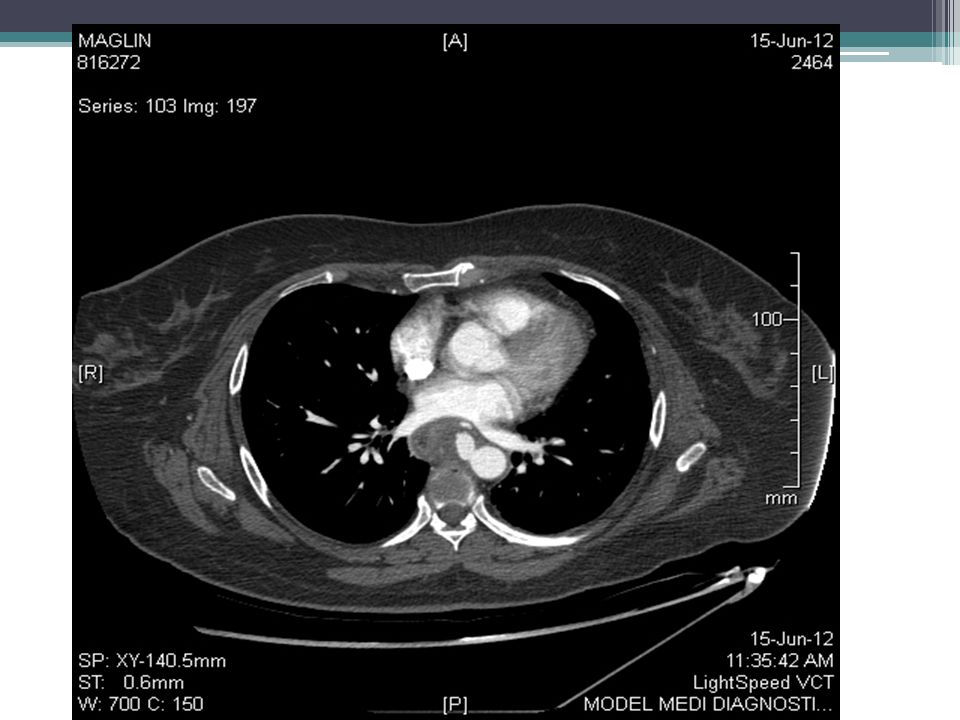
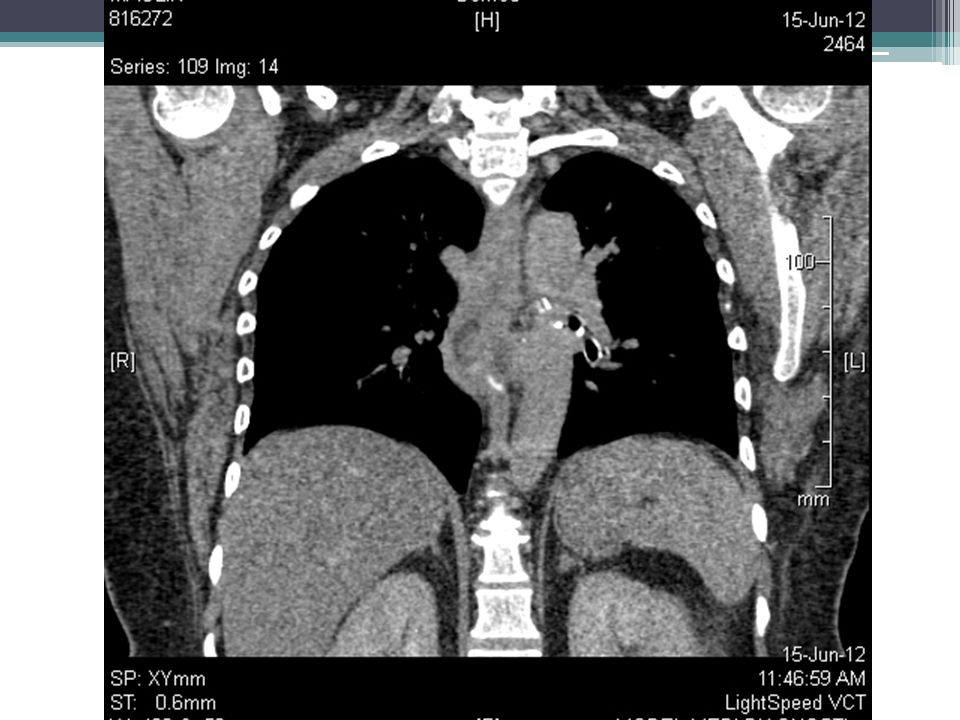
CT chest with aortogram

16
Diagnosis Upper GI Bleed Aortoesophageal Fistula

17
How to Manage ?

18
How to Manage ( what literature says?) High mortality Common cause of death – ▫Exsanguinating Bleed ▫ Infection
 High mortality Common cause of death – ▫Exsanguinating Bleed ▫ Infection")
19
How to Manage ( what literature says?) 2 main options for Aortic Pseudo aneurysm ▫Open surgery Aortic repair using – Synthetic material Pedicle graft Thoracic esophagectomy + cervical esophagostomy + gastrostomy ▫Endovascular repair
 2 main options for Aortic Pseudo aneurysm ▫Open surgery Aortic repair using – Synthetic material Pedicle graft Thoracic esophagectomy + cervical esophagostomy + gastrostomy ▫Endovascular repair")
20
How to Manage ( what literature says?) Esophageal defect ?? Leave it alone ?? Esophagostomy/Esophagectomy ?? Stenting ??

21
Plan Endovascular repair Esophageal Stenting PEG for Feeding Antibiotics

22
Esophageal stenting done

24
PEG tube for feeding

25
Follow up aortogram Both stents well in situ No obvious leak seen. Antibiotics PEG feed

26
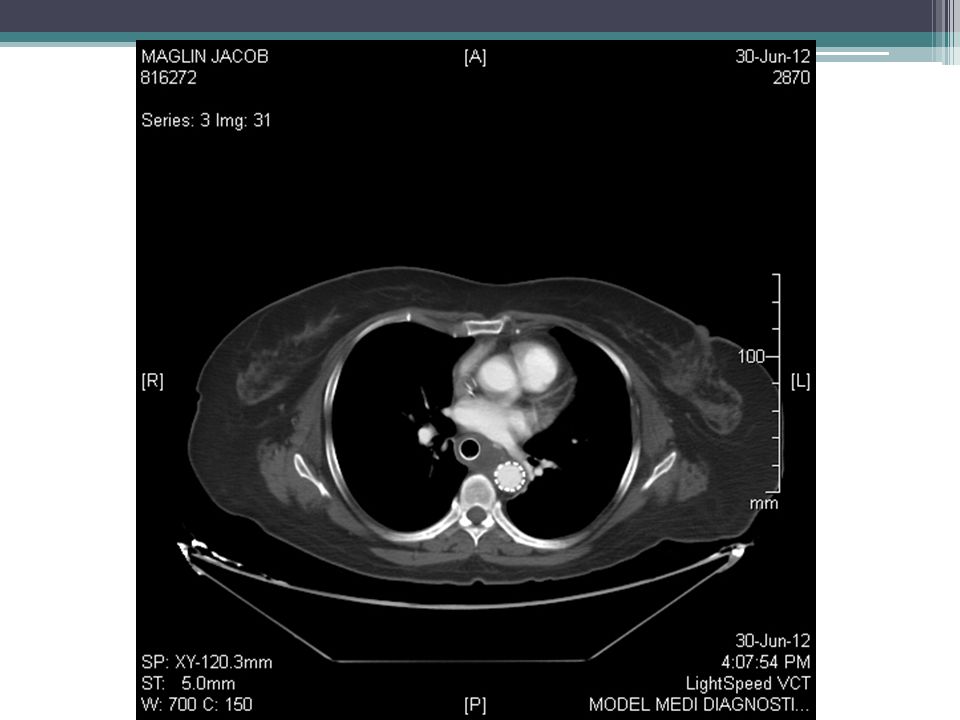
CT Chest after 2 weeks

29
Follow up Six weeks Patient eating well No infection or leak Planned for removal of esophageal stent

30
At Six weeks At six weeks Granulation tissue in growth at both ends of esophageal stent. Unable to remove APC done to ablate the granulation Still stent could not be dislodged.

31
Six Months Both Stents in situ In growth of Granulation tissue at both ends. Planned for APC

32
Thank you.

Similar presentations





 Practice Group Logo here.>")


















