Download presentation
Presentation is loading. Please wait.

1
Boerhaave ’ s Syndrome Is Esophagostomy needed? Dr Derek TL Tam United Christian Hospital

2
Boerhaave ’ s Syndrome 1st descriped by Hermann Boerhaave in 1724 Mortality rate 8-60% Spontaneous transmural perforation of the esophagus Commonly at lower 1/3 of esophagus, involving left thoracic cavity Hill 2003 ANZ J Surg

3
Diagnosis High index of suspicion Vomiting Sudden onset chest / epigastric pain +/- Respiratory symptoms (dyspnea / cough)
")
4
Investigations CXR –Hydrothorax, Hydropneumothroax –Mediastinal emphysema Contrast study –Water soluble contrast –Barium study if inconclusive CT –Difficulty to Dx or locate perforation –Contrast study not a/v

5
Investigations Flexible endoscopy (OGD) –Rarely –Direct visualization of perforation site Thoracentesis –Presence of undigested food –Low pH –↑Salivary amylase
 –Rarely –Direct visualization of perforation site Thoracentesis –Presence of undigested food –Low pH –↑Salivary amylase")
6
Management Prompt recognition Immediate action

7
Initial phase –Resuscitation and close monitoring –NPO –Broad-spectrum antibiotic therapy –NG decompression Whyte 2005 Surg Clin N Am

8
Subsequent phase depends on –Time course –Location, cause, extent of injury –Presence of intrinsic disease (eg. carcinoma / distal obstruction) –Age and general health of patient Whyte 2005 Surg Clin N Am
 –Age and general health of patient Whyte 2005 Surg Clin N Am.")
9
Surgical Objectives Repair of perforation and restore gastrointestinal integrity Eliminate infection and contamination Nutritional support Brinster 2004 Ann Thorac Surg

10
Surgical Plan Infection and contamination: –Thoracotomy –Mediastinal and pleural drainage –Broad-spectrum antibiotics

11
Surgical Plan Perforation: –Primary repair +/- reinforced primary repair +/- T-tube OR –T-tube alone OR –Esophagectomy with immediate or interval reconstruction OR –Endoscopic means Whyte Surg Clin N Am 2005, Davies Ann Thorac Surg 1999

12
Repair of Perforation Primary repair –2 layer repair –Meticulous exposure and repair of mucosa –Repair of muscular tear –Debridement of necrotic tissue Perforations with underlying distal obstruction requires additional evaluation Whyte 2005 Surg Clin N Am, Brinster 2004 Ann Thorac Surg, Zwischenberger 2001 Am J Respir Crit Care Med

13
Repair of Perforation Reinforced primary repair –Pleural flap –Diaphragmatic flap –Pericaridal flap –Intercostal muscle flap –Ometum –Fundus of stomach Whyte 2005 Surg Clin N Am, Brinster 2004 Ann Thorac Surg, Zwischenberger 2001 Am J Respir Crit Care Med

14
Injuries beyond repair Esophageal T-tube –Controlled fistula –Problem of chronic fistula Esophagectomy +/- immediate or interval reconstruction Brinster 2004 Ann Thorac Surg

15
Determinants of Success Interval between perforation and treatment Age and general health of patient Severity of contamination

16
Controversy ? Esophagostomy

17
Our experience Recent 3 consecutive patients Esophagostomy – 2 patients Without esophagostomy – 1 patient

18
Patient 1Patient 2Patient 3 Esophagostomy Yes No ICU stay (days) 111049 Thoracic contamination Well after first thoractomy Requires second thoracotomy Hospital stay (days) 455578 Vocal cord palsyNilLeft VC palsyNil
 Thoracic contamination Well after first thoractomy Requires second thoracotomy Hospital stay (days) Vocal cord palsyNilLeft VC palsyNil")
19
Literature review MEDLINE database –Esophageal perforation –Boerhaave ’ s syndrome –Diversion –Esophagostomy

20
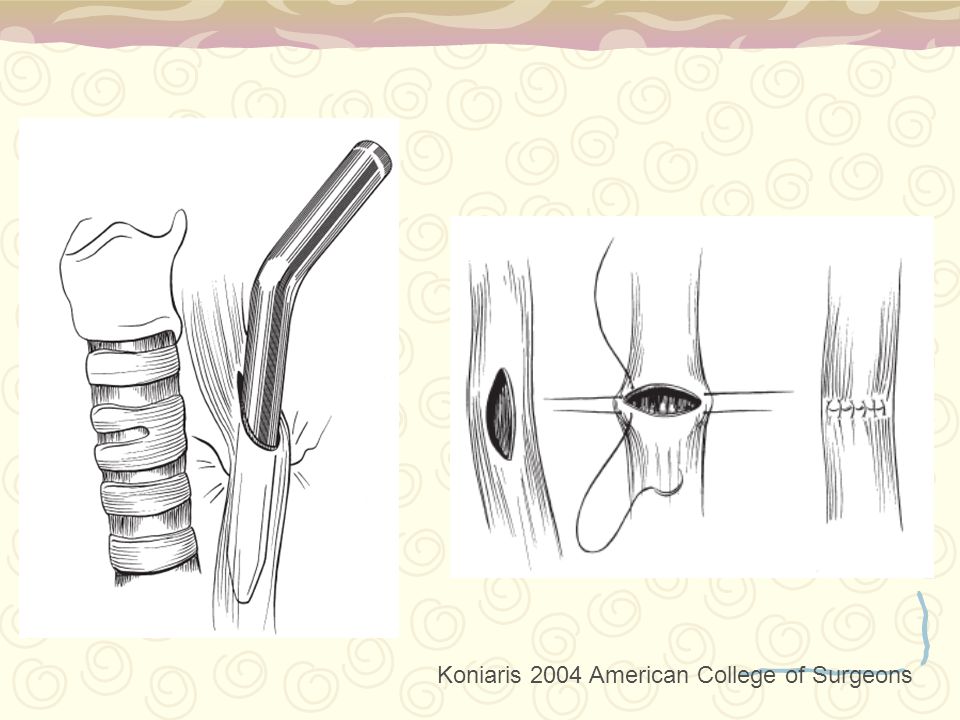
“ Can be extremely helpful in controlling ongoing thoracic contamination and sepsis ” “ Employed when the patient is too unstable to tolerate definitive repair or resection ” Koniaris 2004 American College of Surgeons Whyte 2005 Surg Clin N Am

21
Esophagostomy Described many decades ago Possible role of contamination by oral secretions Form of esophageal diversion Whyte 2005 Surg Clin N Am, Koniaris 2004 American College of Surgeons

22
Originally an end-cervical esophagostomy plus division and closure of esophagus proximal and distal to site of injury Later a side cervical esophagostomy plus placement of either a staple line or removable ligature distally

23
Advantages: –Role of controlling oral secretions is critical –Risk or ability to tolerate ongoing sepsis is impaired Disadvantages: –Needs second operation –Increase risk of morbidity –May result in subsequent leak or late stricture Koniaris 2004 American College of Surgeons

24
Surgical Management No golden standard or guidelines because few surgeons have managed enough patients

25
Conclusion Boerhaave ’ s syndrome requires prompt recognition and aggressive management Individualized approach to every patient Use of cervical esophagostomy carries its own risk of morbidity

26
Thank You

28
Koniaris 2004 American College of Surgeons

Similar presentations