Download presentation
Presentation is loading. Please wait.

1
Spinal Anaesthesia

2
August Bier 1885

3
SPINAL ANESTHESIA

4
ANAESTHETICS USED HYPERBARIC (HEAVY) LIGNOCAINE 5% IN 7.5%DEXTROSE
BUPIVACAINE 0.5% IN 5% DEXTROSE

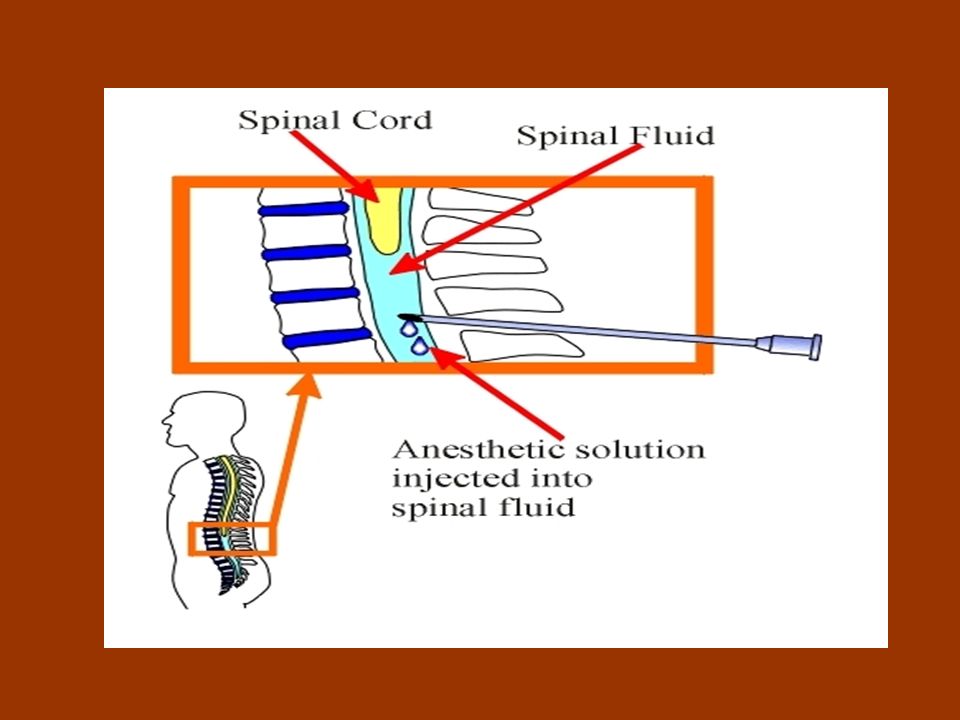
5
HOW A HEAVY ANAESTHETIC SOLUTION FLOWS IN CSF

6
INDICATIONS Economical Pulmonary Diseases Full Stomach
Lower Abdominal Surgery Ischemic Heart Diseases for Lower Abdominal Surgery Fit patient requiring lower abdominal, anal of lower extremity surgery A patient having relative contraindication to general anaesthesia eg respiratory infection, asthma, or a deformed airway Operations where the patient needs to be placed prone eg excision pilonidal sinus Operations of one lower extremity ( hemispinal)
")
7
CONTRAINDICATIONS Hypotensive Patients Cardiac failure Raised ICT
Spinal Deformity Refusing Patients Bleeding Diathesis Skin Infection

8
CONTRAINDICATIONS Unco-operative patient
Operations lasting more than 2 hours Hypovolemic shock Children Sepsis anywhere on the back Operations on the thorax and above

9
TECHNIQUE Preload with 500- 1000ml crystalloid
Premedicate – pentazocine,prometazine, atropine Moniter BP,pulse and O2 sat, heart rhythm

10
COMPLICATIONS IMMEDIATE
Hypotension- increase IV fluids, use small doses of vasoconstrictors eg mephenteramine ( 3mg iv as needed) Bradycardia- iv atropine Respiratory distress- supplement with O2, bag and mask or intubate Inadequate block – supplement with IV ketamine Total spinal IV Isotonic Fluids Vasopressors Oxygen by mask
 Bradycardia- iv atropine. Respiratory distress- supplement with O2, bag and mask or intubate. Inadequate block – supplement with IV ketamine. Total spinal. IV Isotonic Fluids. Vasopressors. Oxygen by mask.")
11
Pregnancy & Spinal Aortocaval Occlusion Pre loading with IV Fluids
Left lateral Position Vasopressors Oxygen therapy

12
COMPLICATIONS LATE Headache Meningitis Back pain

13
Local Anaesthetic Drugs
Lignocaine 2% Lignocaine 5% Bupivacaine 0 .5%

14
Lignocaine Dose 3mg /kg 7mg/kg with adrenaline
Prolong action/reduces the toxicity

15
Lignocane Toxicity Tingling sensation around mouth Drowsiness
Hypotension Fits Treatment Dizepam/Thiopentone Muscle relaxant

16
Bupivacaine Longacting 4-6 hours Deferential blockers
-Sensory more than Motor -Dose mg/kg -Cardiac Toxic -No Tachyphylaxis- Repeat drug

17
SPINAL CORD

18
Where Spinal Cord Ends

20
100% Sterile

21
Spinal Anaesthesia

22
Holding for Spinal

23
Sitting Position

24
Structures Pierced

25
Spinal Needle

26
Factors Influence The Level Of Anaesthesia
The level of Injection The volume of drug Tilt of Table Speed of Injection

27
Advantages of spinal anaesthesia
• Full and complete anaesthesia • Prolonged block: Pain free postoperatively • Alternative to GA for certain poor risk patients esp.: - Difficult airway - Respiratory disease • Contracted bowel • Good muscle relaxation • Suitable for certain surgical procedures: -

28
Caesarian section (awake patient, bonding)
Lower limb surgery Lower abdominal surgery - Urological & gyneacological procedures.

29
SITTING / LYING

30
Reason For the Patho physiological Changes
Blockade of the Sympathetic Systems

31
Cardivascular Changes
Hypotension Tachycardia Bradycardia Sympathetic Blockade Marys law/Mayos Reflex Bainbridge Reflex

32
Drug for Spinal Anaesthesia
Lignocaine Bupivacaine Hyperbaric Stay in the lowest area as per gravity 5% with Glucose 0.5% with Glucose Does not mix up with CSF

33
How to prevent Delayed Complication
Use Thin Spinal needles Sterile Precaution

Similar presentations



 may be used to terminate status epilepticus?>")



 Benzocaine (Hurricaine) Dextrose Glucagon Diphenhydramine (Benadryl) Glucagon.>")











