Download presentation
Presentation is loading. Please wait.

1
Analgesia and Anesthesia in Obstetrics ASIS.PROF.MOHAMMED AL-KHATIM
SUPER VISED BY; ASIS.PROF.MOHAMMED AL-KHATIM Done by :Eman Abdullah AL- otibi

2
Objective: 1-Introduction about anesthesia in pregnancy
2-Uterine innervations and Pain pathway 3- list the different types ,uses ,complications ,contraindications and Factors determining the choice of anesthesia. 4-special considerations while using anesthesia in labor including cardiovascular diseases and uterine inversion

3
Introduction Labor and delivery is a time of intense pain, which is often influenced by the psychological ,emotional , social, cultural , and physiological state of the parturient . multiple methods of alleviating pain are currently available during the birthing process.

4
Definition: Anesthesia: is the absence of all sensation ,including pain,touch,temperature,and pressure. Analgesia: is the absence of nociceptive stimuli ,with the preservation of motor &touch sensation. Ideal :allow the patient to participant in her labor and delivery .

5
Pain pathway: 1-During first stage of labor(visceral pain):
Pain pathway: 1-During first stage of labor(visceral pain): *Visceral pain produced by distention of the uterous &cervix and ischemia of the uterine and cervical Tissue *Pain signal traverse T10 to L1 2-During second stage of labor(visceral+ somatic) *Distention of the vagina ,perineum and pelvic floor *Pain signals traverse the pudendal nerve ( S2 to S4) *more somatic pain
: *Visceral pain produced by distention of the uterous &cervix and ischemia of the uterine and cervical Tissue *Pain signal traverse T10 to L1 2-During second stage of labor(visceral+ somatic) *Distention of the vagina ,perineum and pelvic floor *Pain signals traverse the pudendal nerve ( S2 to S4) *more somatic pain")
6
Type of anesthesia &analgesia:
1-non pharmacological 2-pharmacological

7
-#Non pharmacological:
use In a highly motivated patients this may be all that they require 1-relaxation and concentration on breathing 2-Massage - including aromatherapy 3-Acupuncture and acupressure 4- audioanalgesia. 5-maternal movement and positioning. #Pharmacological: 1-local injection 2-periphral nerve block 3-regional (epidural, spinal) 4-systemic(IV, IM ,inhalation) 5-general anesthesia
 4-systemic(IV, IM ,inhalation) 5-general anesthesia.")
8
A)Local injection: (field bloke)
Local injection: (field bloke)")
9
*indication: Used before episiotomies &for repair of episiotomies or tears that occur during and after delivery *Advantage : no systemic complication if administered correctly *Complication: (rare) systemic complication -toxicity may cause hypotension, arrhythmia and seizures. ( The maximum dose of lidocaine should be 4.5mg\kg per dose) Commonly used agent include lidocaine (1% to 2%) or 2-chloroprocaine (1% to 3%) which provide anthesia mint.. .
 Commonly used agent include lidocaine (1% to 2%) or 2-chloroprocaine (1% to 3%) which provide anthesia mint..")
10
B)Peripheral nerve block (pudendal, paracervical)
Peripheral nerve block (pudendal, paracervical)")
11
*indication: -Paracervical block used in → -first stage of labor in patient in which the epidural or spinal contraindicated -rarely used today duo to fetal adverse effect. -pudendal block used as→ -supplemental during second stage of labor if epidural has not provide adequate analgesia to the sacral nerves. - Also use in lower forceps.

12
Advantages: highly effective and provide an alternative method of pain control .
*Complication: IV injection→ hematoma ,infection. Para cervical block→ fetal bradycardia is a common side effect (15%). Pudendal block→ ♠fetal compromise (rarely occur) ♠maternal toxicity from rapid absorption of the drug
. Pudendal block→ ♠fetal compromise (rarely occur) ♠maternal toxicity from rapid absorption of the drug.")
13
C)regional(epidural, spinal)
regional(epidural, spinal)")
14
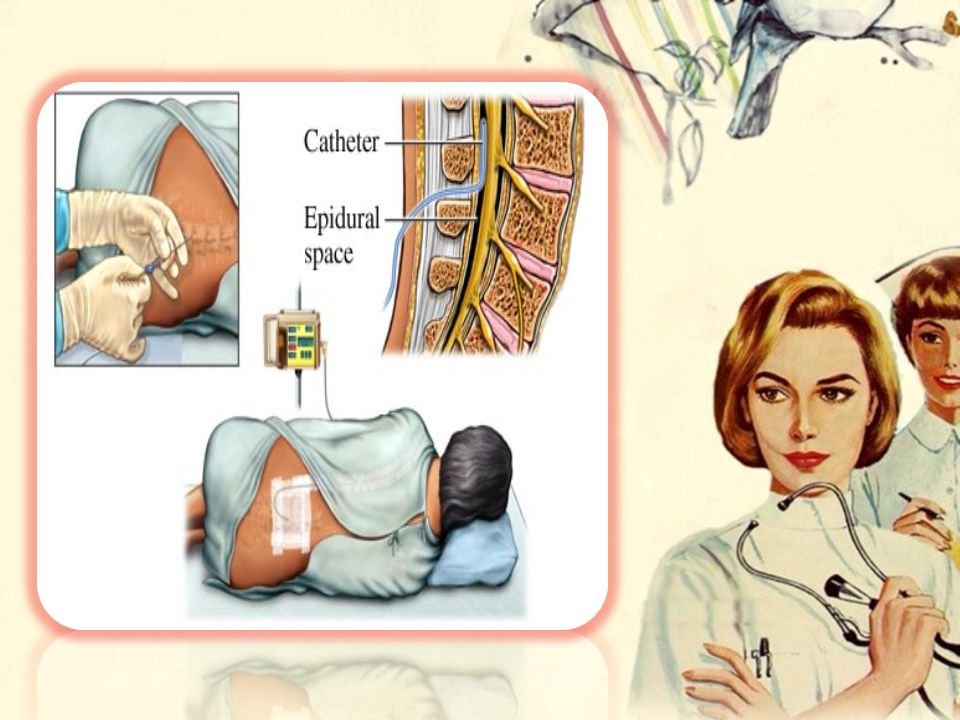
Application Epidural: 1- introduce a catheter into epidural space through a needle usually into the mid-lumber region . 2- The catheter is then secured to the patient's back with adhesive tape. 3- Medication is administered via the epidural route using continuous infusion pumps. 4- A test dose may be given to ensure the correct position of catheter.

18
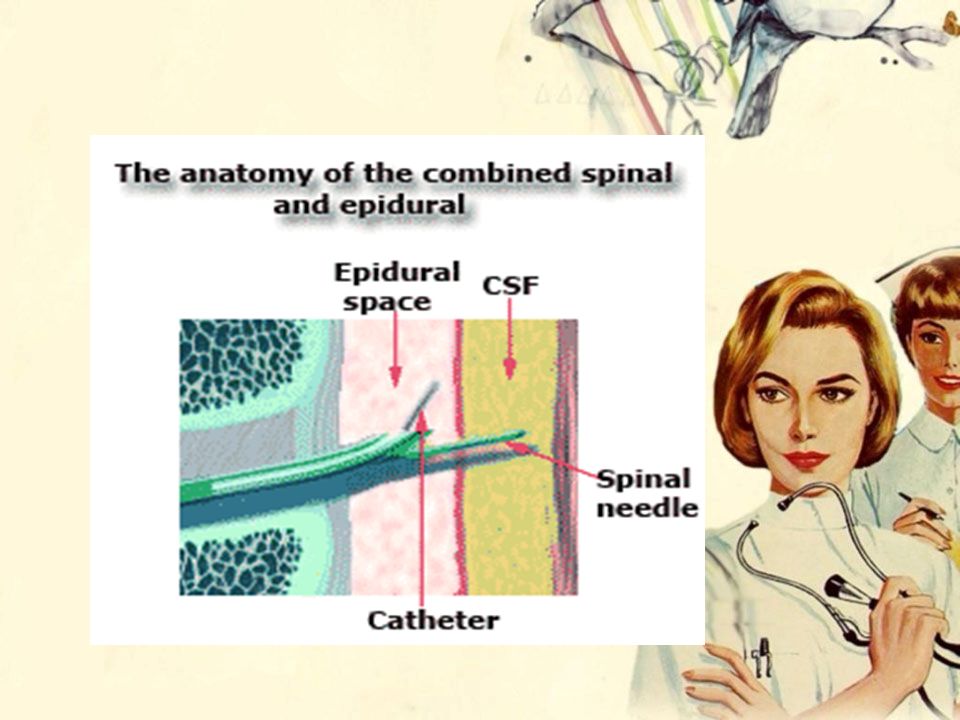
(CSE) Combined spinal epidural The needle-through-needle approach. A single bolus of opiod,perhaps with local anesthetic into subarachanoid space, in addition to an epidural catheter placement in the lumbar epidural space. This method combine a rapid onset of action of spinal with epidural to provide long-lasting throughout the labor and delivery process.

20
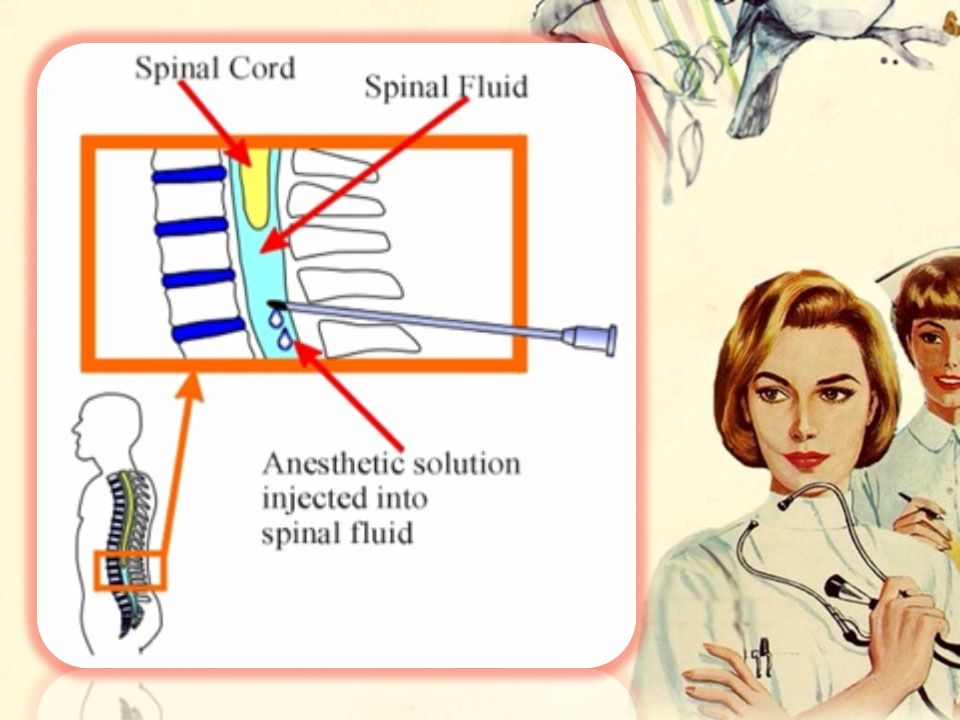
loss of pain sensation occurs below the T8 to T10 levels, with varying degrees of motor blockage. Indications: 1-1st stage of labor.(preferred method of birth control) 2- difficulty with intubation. 3- a history of malignant hyperthermia. 4- CVS or respiratory disorders. 5- preeclampsia.
 2- difficulty with intubation. 3- a history of malignant hyperthermia. 4- CVS or respiratory disorders. 5- preeclampsia.")
21
1-Infection:meningitis ,epidural abscess 2-Neurological complication:
Advantage : provide effective anesthesia &yet allows patient to participates in her labor &delivery. *Complication: 1-Infection:meningitis ,epidural abscess 2-Neurological complication: ♦Spinal headache: -may result in up to 70% of patient. -ttt include analgesics, supine positioning, hydration ♦Obstetric nerve palsies: the commonly injured nerves include lumbosacral trunk ,lateral Coetaneous nerve ,femoral nerve, and common peroneal. ♦back pain .

22
3-drug-related complication:
♦Systemic toxicity: tinnitus, disorientation, and seizures. CV symptoms include hypotension, Cardiac arrest. ♦High spinal: result in a more cranial progression of anesthesia. ♦Motor bloc 4-Hypotension: (because dilatation of vascular beds decrease in venous (return ☻become significant if clinical sign are shown in the mother (light-headedness) Or fetus(bradycardia). ☻ttt with IV fluids or small dose of ephedrine (5mg) 5-Fetal complication: ♦Malpresentation (not clearly known increase risk of shoulder dystocia ) 6-complication in labor; ♦Instrumentation ♦prolongation of second stage of labor.
 Or fetus(bradycardia). ☻ttt with IV fluids or small dose of ephedrine (5mg) 5-Fetal complication: ♦Malpresentation. (not clearly known increase risk of shoulder dystocia ) 6-complication in labor; ♦Instrumentation. ♦prolongation of second stage of labor.")
23
*contraindication: 1-patient's refusal 2-Uncorrected/untreated coagulopathy→ hematoma 3-Skin infection of the lower back→ meningitis. 4-Bacteremia →meningitis. 5-Hypotension/hypovolemia 6-↑intracranial pressure →herniation of cerebral content through foramen magnum

24
D)Systemic (IV, IM, inhalation)
Systemic (IV, IM, inhalation)")
25
-Use opiods (morphine, mepridine),or mixed opiod agonist –antagonist(butorphanole).
-Have very limited efficacy for the relief of labor pain. -They work best in the first stage of labor. *Indication based on maternal request *Complication: -Mother &fetus respiratory depression(cross placenta barrier) -If there is continuous sign of respiratory depression→ repeated dose of naloxone are indicated. -Fentanyl &nalbuphine have the shortest neonatal half-lives of the commonly used .
 -If there is continuous sign of respiratory depression→ repeated dose of naloxone are indicated. -Fentanyl &nalbuphine have the shortest neonatal half-lives of the commonly used .")
26
E)-General anesthesia
-General anesthesia")
27
Indication: ☻In urgent situation (shoulder dystocia, head entrapment) ☻If there is contraindication to regional anesthesia. Advantage: ♦Rapid onset of uterine relaxation occurs, which is desirable with management of uterine inversion, internal/external cephalic version, or fetal entrapment..

28
**Complication: 1-Fetal side effect (respiratory depression)→oxygenation, naloxone, intubation after delivery. 2-Uterine bleeding →managed by pitocin. 3-Risk with intubation increase risk of aspiration and hypoxia . 4- Drug related complications: Potential side effects of the intrathecal opioids include maternal respiratory depression and hypoxemia.

29
During the first stage of labor : visceral pain is mollified by the preferred use of regional anesthesia ♠During vaginal delivery the goal is block nociceptive pathway while preserve motor function By☺ local anesthesia or peripheral nerve blocks . After delivery (post partum ) by oral analgesics. ♠During C.S: 1- better use regional anesthesia (safe, effective, and allows the mother to interact with the baby soon after the delivery ) 2- general anesthesia renders the patient unconscious and unable to experience the moment of birth and is used in urgent situation.. 3- local anesthesia can be used by the obstetrician who is familiar with maximal doses . Postoperative pain management Systemic administration or continuation of the epidural Eventually tranitioned to oral pain medication..
 by oral analgesics. ♠During C.S: 1- better use regional anesthesia (safe, effective, and allows the mother to interact with the baby soon after the delivery ) 2- general anesthesia renders the patient unconscious and unable to experience the moment of birth and is used in urgent situation.. 3- local anesthesia can be used by the obstetrician who is familiar with maximal doses . Postoperative pain management Systemic administration or continuation of the epidural Eventually tranitioned to oral pain medication..")
30
#Special consideration: Cardiovascular diseases:
Regurgitant lesions : Regional anesthesia is better compared to general anesthesia, because It will Improve the blood supply. Stenotic lesions: The general anesthesia will be better compared to the regional one, because the regional anesthesia will further augments the hypotension. - Hypertension: We have to balance Regional anesthesia will lead to more hypotension Uterine inversion : Usually halothane is used to do relaxation, then we will evert the uterus.

31
Factors determining the choice of anesthesia 1-fittness and condition of the mother 2-type and duration of the condition. 3-condition of the fetus. 4- presence of contraindications. 5- opinion of the anesthesiologist

32
Summary : Definition: Analgesia ,Anesthesia Type of anesthesia &analgesia 1-non pharmacological 2-pharmacological

33
Reference

Similar presentations