Download presentation
Presentation is loading. Please wait.

1
Complex OIs of the CNS David R Boulware MD, MPH, CTropMed Lois & Richard King Distinguished Assoc. Professor University of Minnesota boulw001@umn.edu

2
Warm Up: What is the diagnosis?

3
1.Cryptococcosis 2.Emmonsiosis 3.Histoplasmosis 4.Molluscum

4
Case 1 35yo M presents to hospital Fever, Headache, Photophobia of 1 day duration Cough for ~5 days Known HIV+, not in care

5
Statistically, what is the most probable etiology of meningitis? 1.Cryptococcal 2.Meningococcal 3.Pneumococcal 4.TB

6
Case 2 35yo F wife presents to hospital Headache of 10 days duration Cough for ~5 days Known HIV+, not in care

7
Statistically, what is the most probable etiology of meningitis? 1.Cryptococcal 2.Meningococcal 3.Pneumococcal 4.TB

8
What would be the first test you would order on CSF? 1.BACTEC MGIT culture 2.CSF Culture 3.Cryptococcal Antigen 4.Gram’s Stain 5.India ink 6.Xpert MTB/Rif 7.Z-N Stain for AFB

9
HospitalCountry Sample Size HIV infected Meningitis Prevalence Bacterial / Pyogenic TuberculosisCryptococcal Aseptic / Viral Meningitis Mulago and Mbarara 1 Uganda41698%4%8%59%29% GF Jooste 2 South Africa 1,73796%19%13%30%38% Queen Elizabeth Central 3 Malawi26377%20%17%43%20% Harare Central and Parirenyatwa 4 Zimbabwe20090%16%12%45%28% Univ. Teaching Hospital Zambia331100%3%14.5%27.5% †55% Pooled Average 261693% 9.3% (8.2-10.5%) 12.7% (11-14%) 37% (35-39%) 41% (40-43%) Etiologies of Meningitis in Africa Durski K et al. J AIDS 2013 72% in 2014
 12.7% (11-14%) 37% (35-39%) 41% (40-43%) Etiologies of Meningitis in Africa Durski K et al. J AIDS % in")
10
Cape Town, South AfricaKampala, Uganda Jarvis J et al. BMC Inf Dis 2010 Etiologies of Meningitis in Africa Durski K et al. JAIDS 2013

11
Only Modest reduction of Cryptococcosis with ART Roll Out Jarvis J, et al. AIDS 2009 Govender N et al, GERMS 2010 Shift from HIV-status unknown to known HIV+ In Uganda, 95% known HIV+ status at meningitis presentation.

12
Cryptococcal Meningitis Incidence per 100,000 HIV-infected persons, 2014

13
What is the most sensitive test for cryptococcal meningitis? 1.India ink 2.CSF Culture 3.CrAg – latex (CLAT) 4.CrAg – lateral flow assay 5.BACTEC MGIT culture
 4.CrAg – lateral flow assay 5.BACTEC MGIT culture.")
14
Diagnostics Cryptococcal Antigen Lateral Flow Assay US$100 = ZAR 700 = 50 tests

15
What is the least sensitive test for cryptococcal meningitis? 1.India ink 2.CSF Culture 3.CrAg – latex (CLAT)
.")
16
Performance of CrAg LFA Kampala, Mbarara, Cape Town Boulware et al Emerg Infect Dis 2014 Diagnostic TestnSensitivitySpecificity Positive Predictive Value Negative Predictive Value CRAG LFA61999.0%(406/410)99.0%(207/209) * 99.5%(406/408)98.1%(207/211) CSF Culture † 76190.7%(438/483)100%(278/278)100%(438/438)86.1%(278/323) 100 L CSF volume 47995.7%(288/301)100%(178/178)100%(288/288)93.2%(178/191) 10 L CSF volume 28282.4%(150/182)100%(100/100)100%(150/150)75.8%(100/132) India Ink75886.0%(413/480)97.1%(270/278)98.1%(413/421)80.1%(270/337) CRAG-latex (Meridian)27997.8%(176/180)85.9%(85/99)92.6%(176/190)95.5%(85/89) CRAG-latex (Immy)66896.5%(413/428)99.6%(239/240)99.8%(413/414)94.1%(239/254)
99.0%(207/209) * 99.5%(406/408)98.1%(207/211) CSF Culture † %(438/483)100%(278/278)100%(438/438)86.1%(278/323) 100 L CSF volume %(288/301)100%(178/178)100%(288/288)93.2%(178/191) 10 L CSF volume %(150/182)100%(100/100)100%(150/150)75.8%(100/132) India Ink %(413/480)97.1%(270/278)98.1%(413/421)80.1%(270/337) CRAG-latex (Meridian) %(176/180)85.9%(85/99)92.6%(176/190)95.5%(85/89) CRAG-latex (Immy) %(413/428)99.6%(239/240)99.8%(413/414)94.1%(239/254)")
17
Cryptococcal Meningitis: in the first week of therapy, which has largest impact on improving survival among all patients receiving amphotericin. 1.Adjunctive flucytosine (5FC) 2.Adjunctive fluconazole 3.Intracranial pressure management 4.Liposomal Amphotericin
 2.Adjunctive fluconazole 3.Intracranial pressure management 4.Liposomal Amphotericin.")
18
Intracranial Pressure Control >200 mm H 2 O is High –50% prevalence in US –80% prevalence in Uganda >250 mm, Repeat LP daily Yeast obstruct CSF outflow cause ↑ICP –Minimal inflammation in HIV- associated cryptococcosis – Not cerebral edema

19
< 250 mm > 250 mm CSF Opening Pressure Days after Diagnosis Cumulative Survival Survival by Baseline Intracranial Pressure in Uganda Unpublished from the cohort of: Kambugu et al. Clin Inf Dis 2008; 46: 1694-1701.

20
Benefit of therapeutic LPs COAT Trial Sub-Study 248 Persons with Cryptococcus screened for the COAT trial COAT Protocol: scheduled LPs at Day 1,~8,14 and therapeutic LPs recommended when ICP >250 56% with ICP >250mm H 2 O 30% received therapeutic LPs 69% relative reduction in ~10 day mortality, regardless of baseline pressure (95% CI: 18%-88%). 1.3 vs. 2.4 deaths per 100 person days Rolfes MA et al CID 2014; 59:1607-14.

21
Benefit of therapeutic LPs COAT Trial Sub-Study 248 Persons with Cryptococcus screened for the COAT trial 69% relative reduction in ~10 day mortality, regardless of baseline pressure (95% CI: 18%-88%). Baseline CSF ICP <250 mm H 2 O 0% (0/21) vs. 16% (11/77) mortality Baseline CSF ICP >250 mm H 2 O 8% (4/48) vs. 17% (12/69) mortality Rolfes MA et al CID 2014; 59:1607-14. 1.3 vs. 2.4 deaths per 100 person days Timing of 1 st Therapeutic LP
 vs. 16% (11/77) mortality Baseline CSF ICP >250 mm H 2 O 8% (4/48) vs. 17% (12/69) mortality Rolfes MA et al CID 2014; 59: vs. 2.4 deaths per 100 person days Timing of 1 st Therapeutic LP.")
22
Level of Care Kate Birkenkamp Radha Rajasingham

23
At time of initial cryptococcal diagnosis, the median amount of CSF volume needed to be removed to normalize intracranial pressure (<20 cm H 2 O) is? 1.5 mL 2.10 mL 3.15 mL 4.20 mL

24
Case 3 35yo M brother presents to hospital Headache of 10 days duration Cough for ~5 days Known HIV+, not in care CSF Cryptococcal Antigen LFA negative CSF: 65 white cells, 100% lymphocytes 2mL of CSF collected

25
What would be the next test you would order? 1.MGIT culture 2.CSF Culture 3.Cryptococcal Antigen, blood 4.Gram’s Stain 5.India ink 6.Xpert MTB/Rif 7.Z-N Stain for AFB

26
Suspected Meningitis n=207 Blood Fingerstick CRAG Positive n=149 Serum/Plasma CRAG Positive n=149 CSF CRAG Positive n=138 CSF Culture Positive n=126 Williams D Clin Infect Dis 2015 Fingerstick Testing of Cryptococcal Antigen 72%

27
CrAg LFA is negative in blood, what would be the next test you would order? 1.MGIT culture 2.CSF Culture 3.India ink 4.Xpert MTB/Rif 5.Z-N Stain for AFB 6.Repeat large volume LP

28
What would be the next test you would order? 1.MGIT culture4-6 weeks to result 2.CSF Culture5-14 days to result 3.Cryptococcal Antigen, bloodZAR ~45 4.Gram’s StainCase = 10 days of symptoms 5.India inkLess sensitive than CrAg 6.Xpert MTB/RifZAR ~370 7.Z-N Stain for AFBPoor sensitivity

29
WHO, Oct 2014 Strong recommendation: Xpert MTB/RIF should be used as the initial diagnostic test in testing cerebrospinal fluid specimens from patients presumed to have TB meningitis

30
Uganda TBM Results CSF TestNSensitivitySpecificity Positive Predictive Value Negative Predictive Value Xpert 2mL un- centrifuged CSF 107 28% (5/18) 100% (89/89) 100% (5/5) 87% (89/102) Xpert centrifuged CSF 95 72% (13/18) 100% (77/77) 100% (13/13) 94% (77/82) Culture80 71% (12/17) 100% (63/63) 100% (12/12) 93% (63/68) AFB Smear by Microscopy 107 22% (4/18) 100% (89/89) 100% (4/4) 86% (89/103) Bahr NC. Intl J TB Lung Dis; 2015; 19:1209-15 Xpert Protocols: P=0.008 by McNemar’s test

31
MGIT Culture Xpert MTB/Rif 2mL raw CSF AFB Smear Xpert MTB/Rif Centrifuged CSF Median 6 mL 0 3 1 1 1 3 5 4 Bahr NC. Intl J TB Lung Dis; 2015; 19:1209-15

32
TBM Clinical Case Definition Diagnostic Score 1. Clinical criteria (maximum category score =6) Symptoms duration of more than 5 days 4 TB Systemic symptoms: cough for > 2 weeks, weigh loss, night sweats 2 Focal neurological deficit 1 Cranial nerve palsy 1 Altered consciousness 1 2. CSF criteria (maximum category score = 4) Clear appearance 1 Cells 10-500/ul 1 Lymphocyte predominance (>50%) 1 Protein concentration >1g/L 1 CSF to plasma glucose ratio <50% or absolute glucose concentration of <2.2 mmol/l 1 3. Evidence of TB elsewhere (maximum category score= 4) CXR suggestive of TB=2, millary =4 2/4 AFBs from sputum, lymph node, 4 Abdominal Ultrasound evidence for TB 2 4.Exclusion of alternative diagnoses Final diagnosis Probable TBM ≥ 10 Possible TBM 6-9 Not TBM ≤ 5
 Symptoms duration of more than 5 days 4 TB Systemic symptoms: cough for > 2 weeks, weigh loss, night sweats 2 Focal neurological deficit 1 Cranial nerve palsy 1 Altered consciousness 1 2. CSF criteria (maximum category score = 4) Clear appearance 1 Cells /ul 1 Lymphocyte predominance (>50%) 1 Protein concentration >1g/L 1 CSF to plasma glucose ratio <50% or absolute glucose concentration of <2.2 mmol/l 1 3. Evidence of TB elsewhere (maximum category score= 4) CXR suggestive of TB=2, millary =4 2/4 AFBs from sputum, lymph node, 4 Abdominal Ultrasound evidence for TB 2 4.Exclusion of alternative diagnoses Final diagnosis Probable TBM ≥ 10 Possible TBM 6-9 Not TBM ≤ 5.")
33
Cryptococcus vs. TBM Case Definition Diagnostic Score 1. Clinical criteria (maximum category score =6) Symptoms duration of more than 5 days 4 TB Systemic symptoms: cough for > 2 weeks, weigh loss, night sweats 2 Focal neurological deficit 1 Cranial nerve palsy 1 Altered consciousness 1 2. CSF criteria (maximum category score = 4) Clear appearance 1 Cells 10-500/ul 1 Lymphocyte predominance (>50%) 1 Protein concentration >1g/L 1 CSF to plasma glucose ratio <50% or absolute glucose concentration of <2.2 mmol/l 1 3. Evidence of TB elsewhere (maximum category score= 4) CXR suggestive of TB=2, miliary =4 2/4 AFBs from sputum, lymph node, 4 Abdominal Ultrasound evidence for TB 2 4. Exclusion of alternative diagnoses Final diagnosis Probable TBM ≥ 10 Possible TBM 6-9 Not TBM ≤ 5 8-9 Crypto 8-9 Crypto
 Symptoms duration of more than 5 days 4 TB Systemic symptoms: cough for > 2 weeks, weigh loss, night sweats 2 Focal neurological deficit 1 Cranial nerve palsy 1 Altered consciousness 1 2. CSF criteria (maximum category score = 4) Clear appearance 1 Cells /ul 1 Lymphocyte predominance (>50%) 1 Protein concentration >1g/L 1 CSF to plasma glucose ratio <50% or absolute glucose concentration of <2.2 mmol/l 1 3. Evidence of TB elsewhere (maximum category score= 4) CXR suggestive of TB=2, miliary =4 2/4 AFBs from sputum, lymph node, 4 Abdominal Ultrasound evidence for TB 2 4. Exclusion of alternative diagnoses Final diagnosis Probable TBM ≥ 10 Possible TBM 6-9 Not TBM ≤ Crypto 8-9 Crypto.")
34
Case 4 32yo M cousin presents to hospital Headache of 2 days duration, Seizure Known HIV+, CD4=50 cells/ L Started ART ~4 weeks ago Receiving TMP/SMZ (Septrin) ~1 year
 ~1 year")
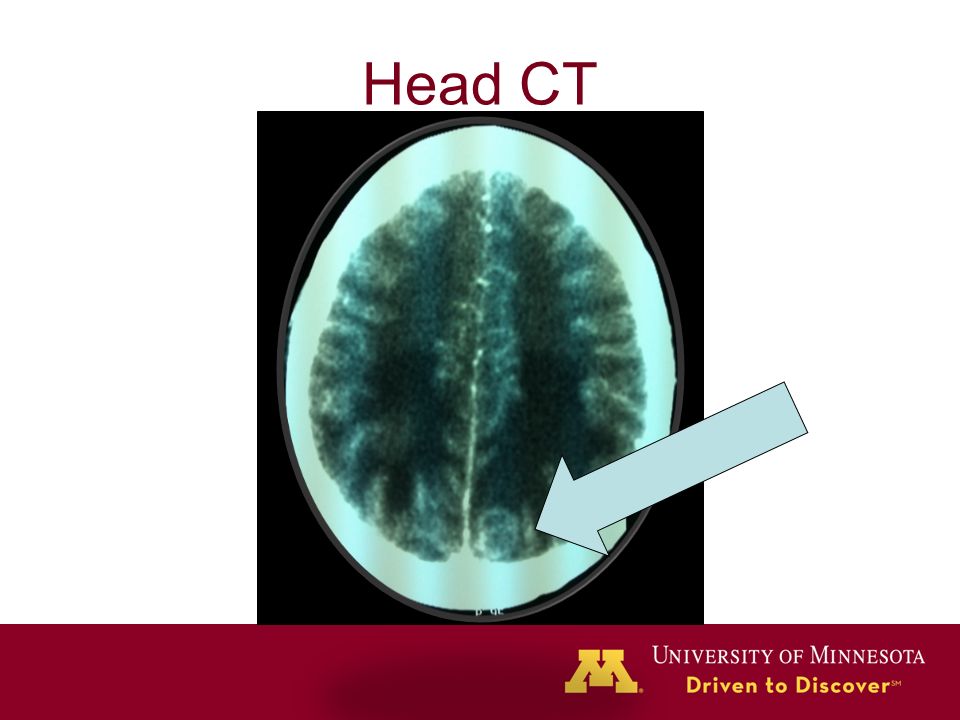
35
Head CT

37
What is your testing/therapy? 1.Biopsy by Neurosurgery 2.CrAg on blood 3.Empiric TB therapy 4.Diagnostic LP 5.Pyrimethamine, sulfadiazine 6.Toxoplasma IgG

38
Pyrimethamine, sulfadiazine prescribed

39
Unmasking Cryptococcosis on ART Accelerated presentation on ART Can present with cryptococcomas –Rare in ART-naïve persons –Looks like Toxoplasmosis Unmasking of Toxo on ART, very rare when receiving TMP/SMZ prophylaxis.

40
Unmasking Cryptococcosis on ART, How can this be prevented? 1.Fluconazole prophylaxis for CD4<100 2.Pre-ART CrAg screening if CD4<100 3.Lumbar Puncture, if CrAg-positive

41
CRAG+ Prevalence ~7.2% average CRAG+ prevalence in CD4<100

42
NHLS CrAg+ Prevalence in CD4<100 Prince Mshiyeni Memorial Hospital (PMMH) in Umlazi, KZN started CrAg Screening in June 2015 4.4% CrAg+ (n=3501)
 in Umlazi, KZN started CrAg Screening in June % CrAg+ (n=3501)")
43
Meya DB, et al. Clin Infect Dis 2010; 51:448-453 N=33 All CD4 CRAG+ 200-400mg 2-4 weeks

44
CRAG Screening + Adherence Support Tanzania & Zambia, CD4<200 Mfinanga et al. Lancet 2015, 385:2173-82.

45
For asymptomatic CrAg+ person, what is the initial therapy? 1.Immediate ART if asymptomatic 2.Fluconazole 800mg/d x 2 wk 3.Fluconazole 400mg/d x 8 wk 4.Fluconazole 200mg/d x 26 wk 5.Amphotericin x1 week

Similar presentations




















 Geneva, Switzerland July 2011 What is the reality in the field? Survey.>")