Download presentation
Presentation is loading. Please wait.

1
Menopausal Hormone Replacement Professor Gordana Prelevic, MD, DSc, FRCP Consultant Endocrinologist Royal Free Hampstead NHS Trust Whittington Health

2
Vasomotor symptoms Hot flushes Sweats Occur in 74% of women Last 5 or more years in 25% 94 % menopausal symptoms 64 % severe symptoms 3rd European Menopause Survey 2005

3
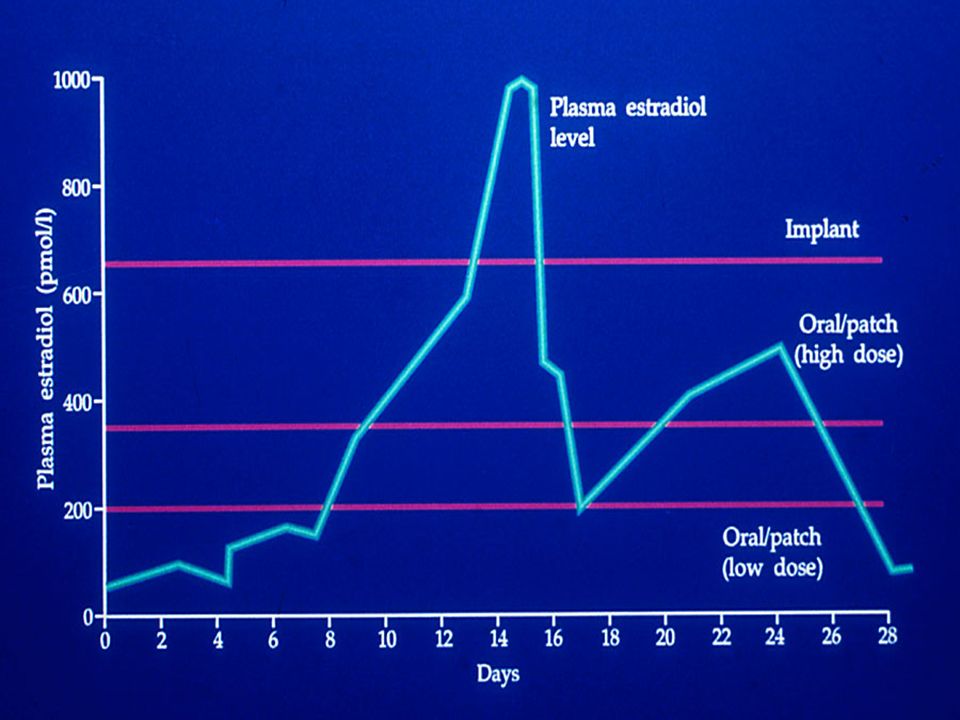
Types of menopausal therapy Conventional HRT Oestrogen oral, transdermal, implant Oestrogen/progestogen sequential or continuous combined Steroid with tissue specific activity Tibolone

4
HRT - doses Oestrogen –dose symptoms bone protection (+/- Ca ++ ) Progestogen –dose (sequential/continuous combined) –duration
 Progestogen –dose (sequential/continuous combined) –duration")
7
HRT - follow up Symptoms Bone mineral density Pelvic US mammography

8
Women’s Health Initiative - WHI Randomized controlled primary prevention trial of 16608 postmenopausal women aged 50-79 with uterus in situ CEO 0.625 mg + MPA 2.5 mg Results: RRCI CHD 1.290.85 - 1.97 Stroke1.410.86 - 2.31 Breast cancer 1.260.83 - 1.92 PE 2.131.26 - 3.55 Colorectal cancer 0.630.32 - 1.24 Hip fracture 0.660.33 - 1.33 JAMA 2002;288:321-333

9
WHI - estrogen alone Randomized controlled primary prevention trial of 10739 postmenopausal women aged 50-79years with prior hysterectomy CEO 0.625 mg Results: RRCI CHD 0.91(0.75 - 1.12) Stroke 1.39(1.10 - 1.77) Breast cancer 0.77(0.59 - 1.01) PE 1.34(0.87 - 2.06) Colorectal cancer 1.08(0.75 - 1.55) Hip fracture 0.61(0.41 - 0.91) JAMA 2004;291:1707-1712
 Stroke 1.39( ) Breast cancer 0.77( ) PE 1.34( ) Colorectal cancer 1.08( ) Hip fracture 0.61( ) JAMA 2004;291:")
11
Menopausal symptoms and quality of life Estrogen therapy is gold standard treatment for hot flushes (effectiveness 90%) 42% of women restarted HRT because of the return of symptoms (3rd European Menopause Survey 2005) Effective doses (0.3 mg CEE, 0.5 mg E 2 25mcg transdermal E2) Only women with flushes have improvement in emotional measures of quality of life (JAMA 2002;287:591-597)
 42% of women restarted HRT because of the return of symptoms (3rd European Menopause Survey 2005) Effective doses (0.3 mg CEE, 0.5 mg E 2 25mcg transdermal E2) Only women with flushes have improvement in emotional measures of quality of life (JAMA 2002;287: )")
12
Breast cancer risk & HRT Population based case control study 975 women with invasive Breast Ca 65-79 yrs & 1007 population controls ERT alone - no increased risk CHRT - 1.7-fold increased risk 2.7-fold increased risk of invasive lobular Ca Relation of HRT to risk of invasive Breast Ca by receptor status ER+/PR+ER+/PR-ER-/PR- E alone1.0 (0.8-1.4)0.7(0.4-1.3)1.0(0.5-1.9) CHRT2.3(1.6-3.2)1.4(0.8-2.4)1.1(0.5-2.2) Li et al JAMA 2003;289:3254-3263
0.7( )1.0( ) CHRT2.3( )1.4( )1.1( ) Li et al JAMA 2003;289:")
15
Clinical profile of tibolone Relief of climacteric symptoms restores vaginal atrophy beneficial effects on libido and mood No endometrial stimulation Prevention of osteoporosis & fractures Risk of stroke similar to HRT Non-estrogenic effect on breast tissue Less breast tenderness than with conventional HRT No increase in mammographic breast density

16
Mammograms before and after treatment with tibolone Woman receiving transdermal E 2 /NETA Same woman 1 year after changing therapy to Livial Valdivia and Ortega 1997

20
Risk of VTE with HRT Risk in current users is 3-4 x higher than in non-users –one case in 5000 users per year The baseline risk of VTE between the ages of 50 and 70 is higher Increased risk appears to be concentrated in new users VTE risk is not increased with transdermal E (oral 3.5 vs TRD 0.9) ESTHER study - Lancet 2003;362:428-432
 ESTHER study - Lancet 2003;362:")
21
HRT & stroke Risk increased for 39% (CEE alone) - 41% (CEE/MPA) 29% increased risk in a meta-analysis (BMJ 2005;330:342- 345) ischaemic stroke risk is cumulative important factor increasing age Low dose TRDE2 no significant risk of stroke
 - 41% (CEE/MPA) 29% increased risk in a meta-analysis (BMJ 2005;330: ) ischaemic stroke risk is cumulative important factor increasing age Low dose TRDE2 no significant risk of stroke")
22
HRT - Cognitive function & Alzheimer’s Disease prevention E may improve cognitive performance in recently menopausal women with menopausal symptoms (JAMA 2001;285:1489-1499) WHIMS - women taking either CEE alone or CEE/MPA had higher risk of dementia (JAMA 2003;289:2651) Negative impact on cognitive abilities when starting HRT after 65years and with existing cognitive problems (JAMA; 2004;291:2959-2968) E in the treatment of AD - no benefit (Neurology 2000;54:295)
 WHIMS - women taking either CEE alone or CEE/MPA had higher risk of dementia (JAMA 2003;289:2651) Negative impact on cognitive abilities when starting HRT after 65years and with existing cognitive problems (JAMA; 2004;291: ) E in the treatment of AD - no benefit (Neurology 2000;54:295)")
23
HRT in women - who should get what? Who ? Women with menopausal symptoms When ? At the time of menopause / perimenopause What ? Minimal dose which controls symptoms (0.5mg oral, 25mcg TRD) Transdermal estradiol (obesity, DM, Hypertension, Liver disease) Estrogen alone (Mirena IUS) Vaginal estriol Tibolone Type of progestogen ? How long ? 3 - 5 years post-menopausal
 Transdermal estradiol (obesity, DM, Hypertension, Liver disease) Estrogen alone (Mirena IUS) Vaginal estriol Tibolone Type of progestogen . How long years post-menopausal.")
24
Key points (1) Primary use of any form of HRT is to control menopausal symptoms HRT should only be prescribed for the short-term relief of menopausal symptoms and prevention of osteoporosis HRT should not be prescribed in the hope or expectation of any protection against arterial CVD or Alzheimer’s disease Oral and non-oral oestrogen have different metabolic profiles that may impact on side-effects and therapeutic risks (VTE risk)
 Primary use of any form of HRT is to control menopausal symptoms HRT should only be prescribed for the short-term relief of menopausal symptoms and prevention of osteoporosis HRT should not be prescribed in the hope or expectation of any protection against arterial CVD or Alzheimer’s disease Oral and non-oral oestrogen have different metabolic profiles that may impact on side-effects and therapeutic risks (VTE risk)")
25
Key points (2) Combined E/PRG preparations have different profiles compared to E alone (lipids, CHD) An increase in breast cancer risk is related to the duration of use and also concurrent use of progestogens. The role of E and/or PRG dose is unclear Tibolone has significantly smaller risk of Breast Cancer compared to E/PRG preparations Data on HRT associated risks should not be extrapolated to women with premature menopause

26
Appropriate & effective doses and regimens need to be individualized HRT should be part of overall strategy –life style –increase exercise –decrease alcohol intake –decrease smoking –fight obesity

Similar presentations










. 2 Recent MHRA/CHM advice Drug Safety Update 2007; 1(2):2-4 The decision to prescribe HRT should be based on a thorough.>")
)>")










![M ENOPAUSE Phil Thirkell. D EFINE THE MENOPAUSE [2 MARKS ] No menstrual periods for 12 months.](/18/5711445/big_thumb.jpg "M ENOPAUSE Phil Thirkell. D EFINE THE MENOPAUSE [2 MARKS ] No menstrual periods for 12 months.>")


>")
