Download presentation
Presentation is loading. Please wait.

2
Water Water constitutes about 65 -70 % total body weight Fluid balance between ECF & ICF Products of digestion are absorbed in a fluid medium and distributed in blood and lymph Controlled body temperature Excretion (lung, kidney,..) Involve chemical reaction
 Involve chemical reaction")
3
Water sources Water is a constituent of most food, even though they may be solid in consistency: Bread contains approximately 35% water Fish 65% Meat 50-70% Vegetables and fruits 80-90%

4
Water balance Water is lost from the body in urine, faeces, sweat and expired air. The regulatory mechanisms in the kidneys result in a variable volume of urine being secreted-consequently a balance is maintained between intake and output of water

5
Requirement An average adult living in a temperate climate requires approximately 2500 ml of water daily. The actual amount that is ingested depends both on climate and habit : Drinks provide 1000-2500 ml. Food provide 1000-1500 ml. Metabolism provide 200-400ml.

6
Dehydration Means loss of water, but is often used as implying a loss of certain mineral elements also, particularly sodium. Loss of up to 5% of body-weight by dehydration results in thirst and discomfort. Loss of 6-10% results in dizziness, absence of saliva and inability to walk. Loss of 11-12% results in delirium, swollen tongue, inability to swallow and shrivelled skin

7
Why Is Water So Important? Water is the most abundant substance in the body Average healthy adult is 50–60% water depending on Age Percent of water declines with age Composition of fat and muscle Muscle is ~65% water Fat is 10–40% water Male 60% and female 50%) )Gender
 )Gender.")
8
Most athletes and coaches are aware that will dehydration will result in a loss of performance. Water is often referred to as the “silent nutrient” To maintain health, and both deficiency symptoms and overdosage symptoms can be observed. Water is a largest single component for about 50- 60% 0f total body mass. Lean body tissue contain a constant fraction – about 75% of water by mass, whereas adipose tissue has a little watter contant. Why Is Water So Important?

9
Electrolyte content, and protein content, which will influence the volume of urine that must excreted. The water formed by the oxidation of food stuffs will make some small contribution to meeting to daily water losses, but water in drinks and in foods will meet most the demand. Losses in urine, faces, sweat, expired air and are the major avenues of water loss : smaller losses occur through blood loss, and in semen, tears, etc., but it was normally trivial Why Is Water So Important?

10
The regulation of body water and electrolyte concentration involves a number of neural and hormonal mechanisms which influence both intake loss. Social and other factors that act to increase or restrict fluid intake. Why Is Water So Important?

11
Metabolic 400 Water production Fluid 1600 Water content of food 1000 Total 3000 Urine 1400 Expired air 320 Skin loss 530 Sweat loss 650 Fecal loss 100 Total 3000 Fluid Balance

12
Water is essential for life, HOW??? Water is vital to health and normal cellular function as it is a medium for metabolic reactions within cells. Transporter for nutrients and waste products. Lubricant. Help in regulating and maintaining body temperature.

14
Water 60% percent of male body weight 50% percent of female body weight Mostly in the intracellular fluid Water exchange between ICF and ECF occurs across cell membranes by osmosis Why this difference between males and females? In old age, only about 45% of body weight is water

15
The Composition of the Body

16
Functions of Water in the Body Commonly known as a universal solvent Polarity allows it to attract charged particles into solutions and dissolve a variety of other polar substances Important to digestion Helps transport dissolved nutrients and other substances throughout the body Blood is composed of water and red blood cells Water allows blood to transport oxygen, nutrients, and hormones to cells Water helps transport waste products away from cells to be excreted

17
Functions of Water in the Body 2 Lubricates joints, sensitive eye tissues, mouth, and intestinal tract Provides a protective cushion, bathing certain organs with fluid During pregnancy the fetus is surrounded by watery amniotic fluid Provides a structural component to cells

18
Figure 11.5 Water Balance between Fluid Compartments Body fluid is located Intracellular – within the cells Extracellular – outside the cells

19
Control of water balance Water intake and excretion are driven by a complex interaction of neural and hormonal factors which respond to a number of different inputs. A rise or fall of about 5msmol /l in the plasma osmolality is sufficient to switch the kidney from maximum conservation of water to maximum urine output Sodium has greatest effect on fluid balance(50% osmolality)
.")
20
Body Fluid Compartments 2/3 (65%) of TBW is intracellular (ICF) 1/3 extracellular water 25 % interstitial fluid (ISF) 5- 8 % in plasma (intravascular fluid) 1- 2 % in transcellular fluids – CSF, intraocular fluids, serous membranes, and in GI, respiratory and urinary tracts (third space)
 of TBW is intracellular (ICF) 1/3 extracellular water 25 % interstitial fluid (ISF) 5- 8 % in plasma (intravascular fluid) 1- 2 % in transcellular fluids – CSF, intraocular fluids, serous membranes, and in GI, respiratory and urinary tracts (third space)")
21
What are the factors that influence body fluids? Age body fluids ↑ in younger than older Body fat content Thin people > obese as fat cells contain little water Sex Male>Female Environmental factors

22
Major Compartments for Fluids INTRACELLULAR FLUID (ICF) Inside cell Most of body fluid here - 63% weight Decreased in elderly EXTRACELLULAR FLUID (ECF) Outside cell Intravascular fluid - within blood vessels (5%) Interstitial fluid - between cells & blood vessels (15%) Transcellular fluid - cerebrospinal, pericardial, synovial
 Inside cell Most of body fluid here - 63% weight Decreased in elderly EXTRACELLULAR FLUID (ECF) Outside cell Intravascular fluid - within blood vessels (5%) Interstitial fluid - between cells & blood vessels (15%) Transcellular fluid - cerebrospinal, pericardial, synovial")
23
ELECTROLYTES IN BODY FLUID COMPARTMENTS INTRACELLULAREXTRACELLULAR POTASSIUMSODIUM MAGNESIUMCHLORIDE PHOSPHOROUSBICARBONATE

24
Movement of Body Fluids and Electrolytes It can be by: Osmosis? Diffusion? Filtration ? Active transport

25
METHODS OF FLUID & ELECTROLYTE MOVEMENT 1- Passive Transport Diffusion Osmosis Filtration 2- Active Transport using energy (ATP)
")
27
DIFFUSION Process by which a solute ( ions and molecules) in solution moves as gas or substance Molecules move from an area of higher concentration to an area of lower concentration to evenly distribute the solute in the solution It can be simple or facilitated diffusion
 in solution moves as gas or substance Molecules move from an area of higher concentration to an area of lower concentration to evenly distribute the solute in the solution It can be simple or facilitated diffusion")
30
FACILITATED DIFFUSION Involves carrier system that moves substance across a membrane with simple diffusion, (from area of higher concentration to one of lower concentration) Example is movement of glucose with assistance of insulin across cell membrane into cell
 Example is movement of glucose with assistance of insulin across cell membrane into cell")
31
Figure 11.6 Osmosis

32
Electrolytes Participate in Fluid Balance Osmosis Strongest factor influencing water balance between compartments Water moves from a diluted concentration to a more concentrated area Osmolarity of a solution indicates total concentration

33
FILTRATION Movement of fluid and solutes together through a selectively permeable membrane from an area of higher hydrostatic pressure to an area of lower hydrostatic pressure Arterial end of capillary has hydrostatic pressure > than osmotic pressure so fluid & diffusible solutes move out of capillary

34
ACTIVE TRANSPORT SYSTEM Moves molecules or ions uphill against concentration & osmotic pressure Requires specific “carrier” molecule as well as specific enzyme (ATP) Hydrolysis of adenosine triphosphate (ATP) provides energy needed Sodium-potassium pump is an active transport system. It moves substances from area of low solutes concentration to a higher one

36
Homeostasis definition? The tendency of an organism or a cell to regulate its internal conditions, usually by a system of feedback controls, so as to stabilize health and functioning, regardless of the outside changing conditionsorganismcellinternalconditionsfeedback controlshealthconditions

37
HOMEOSTASIS!!!

38
What is Homeostasis? HHomeostasis makes sure our body has the correct levels of; Temperature Carbon dioxide OxygenWater Homeostasis involves maintaining a constant internal environment in the body

39
InOut Breath Sweat Faeces Urine Food and drink Water made in respiration B2 : How does the body control water balance? Our bodies need a balanced water level to keep the internal concentration of our cells at the correct level for them to work properly.

40
The kidneys Kidneys do two main jobs: 1.Remove waste urea from the blood. 2. Keep a balance of other chemicals in the blood – including water.

41
The kidneys can cover water and electrolytes by reducing the rate of loss, but can do nothing to store a deficit, which can only be corrected by fluid intake. The subjective sensation of thirst initiates the desire to drink and hence plays a key role in the control of fluid balance. Thirst relatively insensitive to acute changes in hydration status in humans, and the desire to drink is a powerful regulatory factor

42
A number of the sensations associated with thirst: Drinking behavior Dryness of the mouth or throat Distention of stomach

43
The thirst control centers in the brain play a key role in the regulation of both thirst and diuresis. Changes in plasma osmolality and blood pressure and volume, while others are stimulated by the fluid balance hormones which also regulate renal excretion. A rise of between 2 and 3 % in plasma osmolality from the normal level of about 280- 295 msmol/l Is sufficient to evoke a profound sensation of thirst coupled with an increase in the circulating concentration of ADH

44
Homeostatic Mechanisms Kidneys: The kidneys are functioning under the mastering of aldosterone and antidiuretic hormone (ADH). Regulate electrolytes levels in the ECF by selective retention of needed substances and excretion of unneeded substances. Regulate pH of ECF by excretion or retention of hydrogen ions.

45
Antidiuretic Hormone (ADH) Stimulates water conservation at kidneys: reducing urinary water loss concentrating urine Stimulates thirst center: promoting fluid intake
 Stimulates water conservation at kidneys: reducing urinary water loss concentrating urine Stimulates thirst center: promoting fluid intake")
46
ADH Production Osmoreceptors in hypothalamus monitor osmotic concentration of ECF (plasma, CSF) Change in osmotic concentration in plasma and CSF alters osmoreceptor activity Osmoreceptor neurons secrete ADH in proportion to osmotic concentraiton via the posterior pituitary
 Change in osmotic concentration in plasma and CSF alters osmoreceptor activity Osmoreceptor neurons secrete ADH in proportion to osmotic concentraiton via the posterior pituitary")
47
Aldosterone Is secreted by adrenal cortex in response to: rising K + (sensed at the adrenal cortex) or falling Na + levels in blood activation of renin–angiotensin system (usually due to changes in blood volume) Determines rate of Na + absorption and K + loss along DCT and collecting system “Water Follows Salt” High plasma aldosterone concentration causes kidneys to conserve salt Conservation of Na + by aldosterone also stimulates water retention
 or falling Na + levels in blood activation of renin–angiotensin system (usually due to changes in blood volume) Determines rate of Na + absorption and K + loss along DCT and collecting system Water Follows Salt High plasma aldosterone concentration causes kidneys to conserve salt Conservation of Na + by aldosterone also stimulates water retention")
48
Figure 26.8 Aldosterone

49
Figure 11.8 Blood Volume Regulates Blood Pressure

50
Water content of the blood normal Water content of the blood HIGH Water content of the blood LOW Too much water drunk Too much salt or sweating Brain produces More ADH Urine output LOW Brain produces Less ADH Urine output HIGH High volume of water reabsorbed by kidney Low volume of water reabsorbed by kidney (small volume of Concentrated urine) (large volume of dilute urine)
 (large volume of dilute urine)")
51
Normal blood concentration Blood too concentrated – detected in brain ADH secreted by pituitary gland ADH causes kidneys to reabsorb more water to blood Normal blood concentration Blood too dilute – detected in brain ADH not secreted by pituitary gland kidneys reabsorb less water to blood Water Balance

52
Natriuretic Peptides ANP and BNP are released by cardiac muscle cells in response to abnormal stretching of heart walls due to elevated blood pressure or volume Reduce thirst Block release of ADH and aldosterone Cause diuresis Lower blood pressure and plasma volume

53
FLUID VOLUME DEFICIT (FVD) Hypovolemia or FVD is result of water & electrolyte loss Compensatory mechanisms include: Increased sympathetic nervous system stimulation with an increase in heart rate & cardiac contraction; thirst; plus release of ADH & aldosterone Severe case may result in hypovolemic shock or prolonged case may cause renal failure
 Hypovolemia or FVD is result of water & electrolyte loss Compensatory mechanisms include: Increased sympathetic nervous system stimulation with an increase in heart rate & cardiac contraction; thirst; plus release of ADH & aldosterone Severe case may result in hypovolemic shock or prolonged case may cause renal failure")
54
Disorders of Water Balance: Figure 26.7a

56
Several factors will influence the body water losses and thus determine the requirement for water intake Ambient climatic condition Level of physical activity Body size Body composition & volume Metabolically activity Body surface area

57
FLUID VOLUME DEFICIT (FVD) Hypovolemia or FVD is result of water & electrolyte loss Compensatory mechanisms include: Increased sympathetic nervous system stimulation with an increase in heart rate & cardiac contraction; thirst; plus release of ADH & aldosterone Severe case may result in hypovolemic shock or prolonged case may cause renal failure
 Hypovolemia or FVD is result of water & electrolyte loss Compensatory mechanisms include: Increased sympathetic nervous system stimulation with an increase in heart rate & cardiac contraction; thirst; plus release of ADH & aldosterone Severe case may result in hypovolemic shock or prolonged case may cause renal failure")
58
SIGNS & SYMPTOMS OF FVD Dry mucous membranes Weight loss Orthostatic hypotension & tachycardia Subnormal Body temperature Flat neck veins & decrease in CVP Decreased urinary output & altered sensorium

59
Dehydration !!!! Water isn’t replaced in body Fluid shifts from cells to EC space Cells lose water Happens in confused, comatose, bedridden persons along with infants & elderly May be treated with hypotonic sol (like dextrose 5% in water)
.")
60
Signs of Dehydration

62
Dehydration Causes Risk Factors Insufficient intake due to anorexia, nausea, impaired swallowing, confusion, depression. Loss of water and electrolytes from: vomiting, diarrhea, nasogastric suction, excessive sweating, fever, polyuria, abdominal drainage, or wound losses.

63
FLUID VOLUME EXCESS (FVE) FVE is a result of expansion of fluid compartment due to increase in total sodium content. Fluid excess in the intravascular space is called hypervolemia. Fluid excess in interstitial space is called edema Excess of extra cellular fluid in other body compartment Third space is called. Fluids may be trapped in abdomen, peritoneum (ascites) or plural space (plural effusion).
 or plural space (plural effusion)..")
64
SIGNS & SYMPTOMS OF FVE Orthopnea Edema & weight gain Distended neck veins & tachycardia Increased blood pressure Crackles & wheezes May be ascites & pleural effusion Increase in CVP

65
EDAEMA It is excessive accumulation of fluid in the interstitial space it may be localized edema if it due to trauma or inflammation. Generalized edema involves the whole body. It is severe.

66
Pitting edema on the leg Pitting edema on the foot

67
Pitting odema

68
Water Intoxication !!!! Excess fluid moves from EC space to IC space Happens with SIADH, rapid infusion of hypotonic IV sol or tap water as NG irrigant or enemas; can happen with psychogenic polydipsia ( may drink 12-18 L/day ) Findings Serum NA < 125 mEq/L Serum Osmolality < 280 mOsm/kg
 Findings Serum NA < 125 mEq/L Serum Osmolality < 280 mOsm/kg.")
69
Electrolyte Balance An electrolyte balance exists when the quantities of electrolytes gained equals the amount lost. Electrolyte Intake - The electrolytes of greatest importance to cellular metabolism are sodium, potassium, calcium, magnesium, chloride, sulfate, phosphate, bicarbonate, and hydrogen ions. - Electrolytes may be obtained from food or drink or produced as a by-product of metabolism.

70
Electrolyte Balance Regulation of Electrolyte Intake - A person ordinarily obtains sufficient electrolytes from foods eaten. - A salt craving may indicate an electrolyte deficiency. Electrolyte Output - Losses of electrolytes occur through sweating, in the feces, and in urine.

71
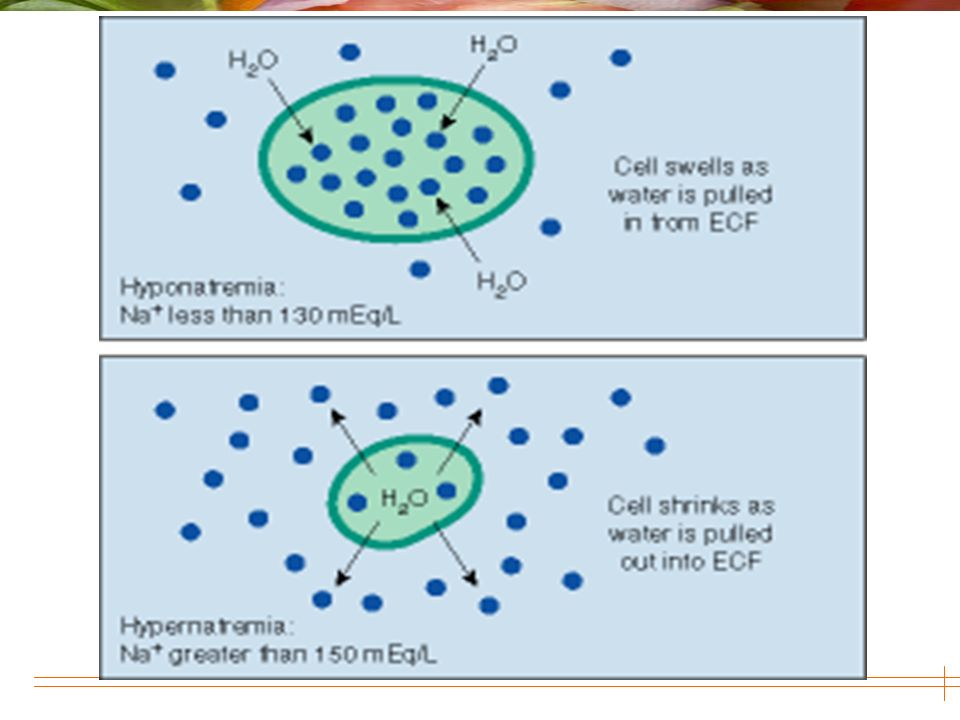
Electrolyte Imbalances 1. Sodium – Hyponatremia – Hypernatremia 2. Potassium – Hypokalemia – Hyperkalemia 3. Calcium – Hypocalcemia – Hypercalcemia 4. Magnesium – Hypomagnesemia – Hypermagnesemia 5. Phosphorus – Hypophosphatemia – Hyperphosphatemia

72
Calcium More than 99% of total body calcium is stored in the bones and teeth where it functions to support their structure. The remaining 1% is found throughout the body in blood, muscle, and the fluid between cells.

73
function Calcium is also critical for the normal transmission of nerve impulses. Calcium flows into nerve cells and stimulates the release of molecules called neurotransmitters. Calcium also plays the role in muscle contraction, healthy blood pressure, the initiation of blood clotting, and the regulation of various hormones and enzymes.

74
Food Sources : Best sources: milk and milk product; Good sources: beans, vegetables, fish, cabbage,broccoli

75
Three Forms of Circulating Ca2+

76
Calcium Balance Intake = output Negative calcium balance: Output > intake Neg Ca 2+ balance leads to osteoporosis Positive calcium balance: Intake > output Occurs during growth Calcium is essential, we can’t synthesize it

77
Calcium and the Cell Translocation across the plasma membrane Translocation across the ER and mitochondrion; Ca2+ ATPase in ER and plasma membrane

78
Anatomy and Feedback Inhibition

79
Regulation of PTH Secretion and Biosynthesis Extracellular Ca 2+ regulates secretion of PTH Low Ca 2+ increases High Ca 2+ decreases Ca2+ also regulates transcription High levels of 1,25 dihydroxyvitamin D3 inhibit transcription

80
Calcitonin This decreases serum Ca2+ Promotes renal excretion of Ca2+ Probably not essential for human survival Potential treatment for hypercalcemia

81
Transport and Metabolic Sequence of Activation of Vitamin D

82
Vitamin D-dependent Ca2+ Absorption Duodenum>jejunum>ileum Absorption is greater at low pH The pH of the stomach is about 2 Peak absorption at the beginning of the duodenum

83
Sequence of Adjustments to Hypocalcemia

84
SODIUM (NA)* Normal Serum [Na] (135-145 mEq/L) Main extracellular fluid (ECF) cation Influences water distribution (with chloride )
![SODIUM (NA)* Normal Serum [Na] ( mEq/L) Main extracellular fluid (ECF) cation Influences water distribution (with chloride )](http://images.slideplayer.com/27/8930586/slides/slide_84.jpg "SODIUM (NA)* Normal Serum [Na] ( mEq/L) Main extracellular fluid (ECF) cation Influences water distribution (with chloride )")
85
Sodium Functions Transmission and conduction of nerve impulses Responsible for osmolarity of vascular fluids Regulation of body fluid levels Sodium shifts into cells and potassium shifts out of the cells (sodium pump) Assists with regulation of acid-base balance by combining with Cl or HCO3 to regulate the balance
 Assists with regulation of acid-base balance by combining with Cl or HCO3 to regulate the balance")
89
MAGNESIUM Magnesium is a cofactor in more than 300 enzyme systems that regulate diverse biochemical reactions in the body, including protein synthesis, muscle and nerve function, blood glucose control, and blood pressure regulation

90
Food Sources Green vegetables such as spinach because the center of the chlorophyll molecule(which gives green vegetables their color) Legumes(beans and peas) Nuts and seeds
 Legumes(beans and peas) Nuts and seeds")
91
Daily Requirement ADULT MEN 19 to 30400mg 31 yrs and older420mg ADULT WOMEN 19 to 30310mg 31 yrs and older320mg

92
Approximately 30% to 40% of the dietary magnesium consumed is typically absorbed by the body Typical magnesium absorption involves: 40% of magnesium intake absorbed in the small intestine 5% absorbed in the large intestine 55% leaving the body as waste

93
Potassium Dominant cation in intracellular fluid (ICF) Serum potassium3.5 – 5 mmol/L K+ intake 4700mg from vegetable and fruit K+ excretion: Kidney : approximately 90% of dietary potassium GI tract: only about 10 % Major organ of excretion potassium: kidney Regulative site: renal distal tubule
 Serum potassium3.5 – 5 mmol/L K+ intake 4700mg from vegetable and fruit K+ excretion: Kidney : approximately 90% of dietary potassium GI tract: only about 10 % Major organ of excretion potassium: kidney Regulative site: renal distal tubule")
94
Factors of affecting renal handling potassium Aldosterone Activates Na+-K+ ATPase Sodium channels in the luminal membrane Na+reabsorption Potassium channels in the luminal membrane Intracellular potassium content Secretion Urine flow rate Secretion Distal delivery of sodium Secretion Acid-base balance: Acute acidosis Secretion

95
2) Balance of potassium distribution: It is depended Na+—K+—ATPase on the cellular membrane(pump leak). consumption of 1 ATP → pumping 3 Na+ out off and 2 K+ into the cell Total body potassium approximately 98% in ICF 50-55mmol/kg B.W approximately 2% in ECF ICF (3500mmol ): 150-160mmol/L ECF (70 mmol ): serum potassium 3.5-5.5mmol/L
: mmol/L ECF (70 mmol ): serum potassium mmol/L.")
96
Phosphorous (P) How is P used in organisms? Biomolecules ADP and ATP nucleic acids phospholipids (cell membranes) apatite (bones and tooth 80%)
 apatite (bones and tooth 80%).")
97
Serum Phosphorous 2.4– 4.6 mgl/dL Food Sources: meat & milk

98
Acid-Base Balance 7.35-7.45

99
Definitions Acid: is a substance that can donate hydrogen ions in solution. Strong acid such as hydrochloric acid (HCl)release all the H+. Weak acids like carbonic acid (H2CO3) release some H+. Base or Alkali: is a substance that can accept hydrogen ions in solution. Acidity or alkalinity is measured by pH. ACID-BASE BALANCE
release all the H+. Weak acids like carbonic acid (H2CO3) release some H+. Base or Alkali: is a substance that can accept hydrogen ions in solution. Acidity or alkalinity is measured by pH. ACID-BASE BALANCE.")
100
Definitions 2 pH: means the concentration of hydrogen ions [H+] of the solution. In the body, weak acids and weak bases regulate acid- base balance to prevent sudden changes in the pH of the body fluids. Normal pH= 7.35 – 7.45. 7.45 = alkalosis
![Definitions 2 pH: means the concentration of hydrogen ions [H+] of the solution.](http://images.slideplayer.com/27/8930586/slides/slide_100.jpg " In the body, weak acids and weak bases regulate acid- base balance to prevent sudden changes in the pH of the body fluids. Normal pH= 7.35 – 7.45 = alkalosis.")
101
ACID-BASE BALANCE Governed by the regulation of hydrogen ion (H+) concentration in the body pH = negative logarithm of the H+ concentration Acids - proton donors & give up H+ Bases - H+ acceptors Acidic - inc. in concentration of H+ Basic - dec. in concentration of H+

102
Regulation of Acid-Base Balance Normal Values: pHPCO2HCO3 7.35 – 7.45 35 – 45 mm Hg 22 – 26 mEq / L

103
Acid – Base Balance

104
Acid Base Balance

105
Arterial Blood Gases (ABGs)
")
106
Arterial Blood Gases (ABG) pH 7.35-7.45 PaCO2 35-45 mm Hg Pa O2 80-100 mm Hg O2 sat. 95-99% HCO3- 22-26mEq/L

107
Acid-Base Balance The Respiratory Center - The respiratory center in the brain stem helps to regulate hydrogen ion concentration by controlling the rate and depth of breathing. - During exercise, the carbon dioxide, and thus the carbonic acid, levels in the blood increase. - In response, the respiratory center increases the rate and depth of breathing, so the lungs excrete more carbon dioxide.

108
Acid-Base Balance The Kidneys - Nephrons secrete excess hydrogen ions in the urine.

109
Acid-Base Imbalances Chemical and physiological buffer systems usually keep body fluids within very narrow pH ranges but abnormal conditions may prevent this. CHEMICAL BUFFER SYSTEMS - bicarbonate, phosphate, protein, hemoglobin LUNGS - carbonic acid broken down into CO2 & H2O KIDNEYS - increasing or decreasing bicarbonate ions

110
Acid-Base Imbalances Acidosis Two major types of acidosis are respiratory and metabolic acidosis. - Respiratory acidosis results from an increase of carbonic acid caused by respiratory center injury, air passage obstructions, or problems with gas exchange. - Metabolic acidosis is due to either an accumulation of acids or a loss of bases and has many causes including kidney disease, vomiting, diarrhea, and diabetes mellitus.

111
Acid-Base Imbalances Increasing respiratory rate or the amount of hydrogen ions released by the kidney can help compensate for acidosis.

112
Respiratory Acidosis * pH < 7.35 PaCO2 > 45mm Hg Due to inadequate alveolar ventilation Tx aimed at improving ventilation Respiratory Opposite

113
Respiratory Alkalosis* pH > 7.45 PaCO2 < 35mm Hg Due to alveolar hyperventilation & hypocapnia Tx depends on underlying cause

114
Metabolic Acidosis* pH < 7.35 HCO3 < 22mEq/L Due to gain of acids or loss of base (like excessive GI loss from diarrhea) May have associated hyperkalemia Tx aimed at correcting metabolic defect Metabolic Even
 May have associated hyperkalemia Tx aimed at correcting metabolic defect Metabolic Even")
115
Metabolic Alkalosis* pH > 7.45 HCO3 > 26 mEq/L Due to loss of acid or gain of base (most common is vomiting or gastric suction) Hypokalemia may produce alkalosis Tx aimed at underlying disorder
 Hypokalemia may produce alkalosis Tx aimed at underlying disorder")
116
Respiratory acidosis Risk FactorsClinical ManifestationNursing Intervention Acute lung disease: pneumonia, acute pulmonary edema, aspiration of foreign body… Chronic lung disease: asthma, cystic fibrosis, emphysema Overdose of narcotics Brain injury Airway obstruction Chest injury Increased pulse Increased respiratory rate Headache Confusion Convulsions Warm flushed skin Assess respiratory status and lung sound Monitor air way and ventilation Inhalation therapy Percussion and postural drainage Monitor fluid intake and output Measure vital signs Measure arterial blood gases

117
Respiratory alkalosis Risk FactorsClinical ManifestationNursing Intervention Hyperventilation due to: -Extreme anxiety -Elevated body temp. -Overventilation -Hypoxia -Salicylate overdose Brain energy Fever Increased basal metabolic rate Shortness of breath Chest tightness Numbness and tingling of extrimities Difficulty concentrating Blurred vision Monitor vital signs and ABGs Assist client to breath more slowly Help client breath in a paper bag

118
Metabolic acidosis Risk FactorsClinical Manifestation Nursing Intervention Increase of non volatile acids in blood: -renal impairment -DM Decrease in bicarbonates: -Prolonged diarrhea Excessive NaCl infusion Salicylates overdose Cardiac arrest Deep rapid respiration Lethargy, confusion Headache Weakness Nausea and vomiting Monitor ABG values Monitor intake and output Monitor of LOC Administer IV sodium bicarbonate

119
Metabolic alkalosis Risk FactorsClinical Manifestation Nursing Intervention Excessive acid base due to: -Vomiting -Gastric suction Excessive use of K-losing diuiretics Excessive adrenal corticoid hormones due to: -Cushing’s syndrome -Hyperaldosteronism Excessive bicarbonate intake from: -Antacids -Parenteral NaHCO 3 Increase respiratory rate and depth Dizziness Numbness and tingling of the extremities Hypertonic muscles, tetany Monitor intake and output Monitor vital signs especially respiration and LOC Administer IV fluid carefully

120
http://irhk.ir /

Similar presentations


























 Newborn (77%) Adult male (60%) Adult female (54%) Elderly (45%) Adipose.>")

 Potassium (K + )>")
