Download presentation
Presentation is loading. Please wait.

1
Initial Management of Critical Airway and Breathing Emergencies

2
Does he need to be intubated? If yes, when and how?

3
How would you manage this patient?

4
58 y/o in shock and respiratory failure

5
Four airway questions Is the airway open? Is breathing adequate? Is oxygenation adequate? Is the airway protected? Indications for intubation

6
Do these patients need to be intubated? Failure to maintain and/or protect airway Failure to oxygenate and ventilate Facilitate therapy or diagnostic procedures When to do the intubation?

7
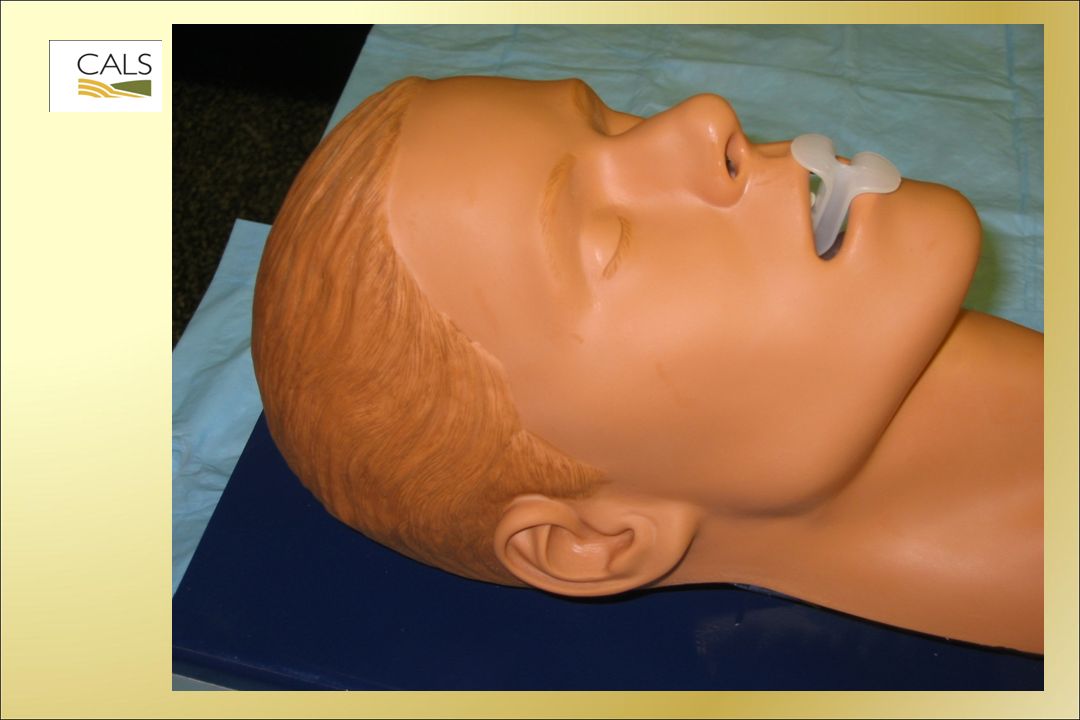
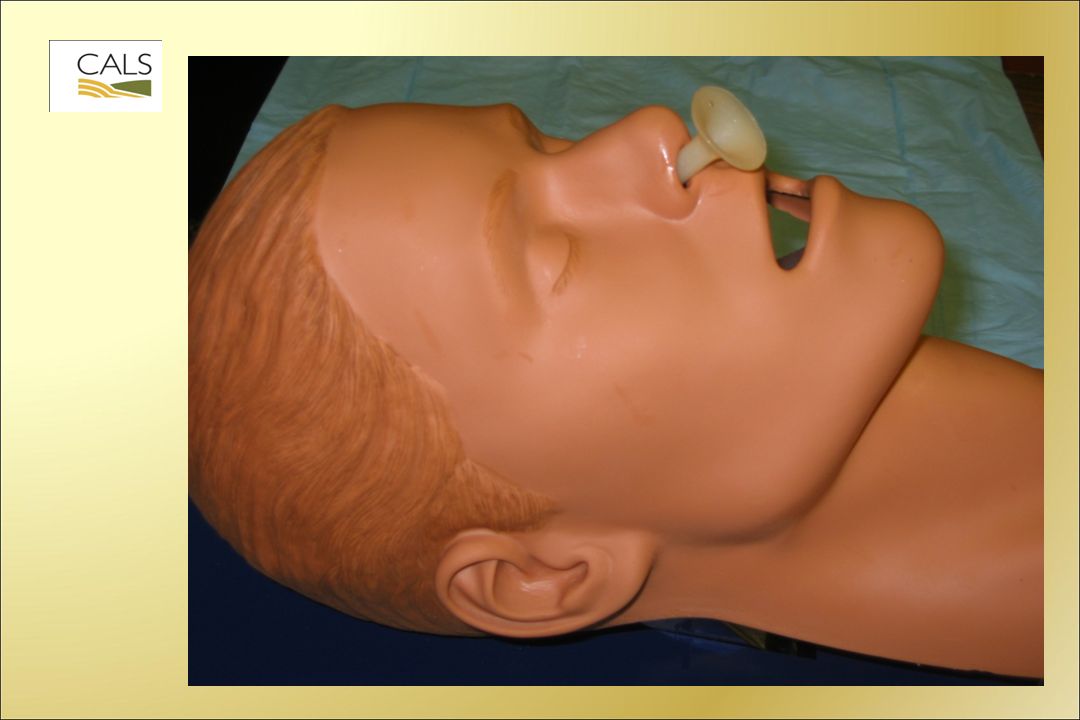
When to intubate? Now? Within 10 minutes? Within 30 minutes? Almost all patients can be managed initially with good BVM ventilation –proper equipment –good technique –airway adjuncts

12
What is the safest and best method to intubate? Rapid Sequence Intubation Awake intubation techniques –Blind nasotracheal intubation –Awake oral intubation –Fiber optic guided intubation –Retrograde intubation over a catheter Surgical technique

13
Rapid Sequence Intubation (RSI) Simultaneous administration of a potent sedative (anesthetic) and a neuromuscular blocking agent to facilitate endotracheal intubation
 Simultaneous administration of a potent sedative (anesthetic) and a neuromuscular blocking agent to facilitate endotracheal intubation")
14
History of emergency airway management Most ER intubations performed on unresponsive patients Sedation without paralytics C-spine concerns in trauma Blind nasotracheal vs. RSI in the ED

15
Rapid Sequence Intubation “the method of choice for emergency airway management in most patients” RK Knopp: Ann Emerg Med 1998

16
Rapid Sequence Intubation - 9 Ps 1. Preparation 2. Preoxygenate 3. Premedicate 4. Push sedative (Anesthetic) 5. Paralyze 6. Position airway: head/neck position; laryngeal manipulation, BURP, cricoid pressure as needed 7. Pass the tube (intubate) 8. Patent airway assessment 9. Post-intubation plan
 5. Paralyze 6. Position airway: head/neck position; laryngeal manipulation, BURP, cricoid pressure as needed 7. Pass the tube (intubate) 8. Patent airway assessment 9. Post-intubation plan.")
17
RSI: Timing Five minutes before intubation: Preparation including selection of drugs & doses, equipment check and team roles; preoxygenation; premedication. 45 - 60 seconds before intubation: administer sedative and paralytic, start laryngeal manipulation 45 - 60 seconds after drugs, introduce laryngoscope, intubate and immediately prove tracheal intubation. This is the Rapid Sequence! Intubate + 1 minute: Post intubation care

18
Preparation Check equipment –Laryngoscopes, ET tubes, suction, introducer –Back up airway Attach monitors - cardiac, oximetry Establish IV (prefer 2), gather drugs Assign tasks to team members
, gather drugs Assign tasks to team members")
19
Preparation Airway drugs –Draw up drugs –Label syringes –Use ET Flow sheet Shamrock Dispenser

20
Preoxygenate 100% O 2 by mask for 3-5 mins or 3 - 4 vital capacity breaths

21
Undesirable responses to intubation Increases ICP Bronchospasm Bradycardia in children Hypertension/tachycardia Fasciculation's with Succinylcholine

22
Pretreatment: attenuation of physiologic response to intubation Lidocaine –May block increase in ICP –May attenuate bronchospasm Atropine –Blocks vagal response in children Opioids (Fentanyl) –Blocks cardiovascular response Non-depolarizer –Blocks fasciculation
 –Blocks cardiovascular response Non-depolarizer –Blocks fasciculation")
23
RSI Drugs - pretreatment Lidocaine - head injury, asthma (1.5 mg/kg) Atropine - children <8 (0.02 mg/kg) Fentanyl - 1-2 micrograms/kg
 Atropine - children <8 (0.02 mg/kg) Fentanyl micrograms/kg")
24
RSI Drugs - sedation Etomidate (Amidate) Thiopental Midazolam (Versed) Ketamine Propofol (Diprivan)
 Thiopental Midazolam (Versed) Ketamine Propofol (Diprivan)")
25
Etomidate (Amidate) Dose: 0.3mg/kg Onset: 30-60 seconds Duration: 3-5 minutes Advantages: Short acting, lowers ICP, with no adverse cardiovascular effects, Disadvantages: Nausea, myoclonus, ? Cortisol suppression Ultrashort-acting nonbarbiturate hypnotic

26
Etomidate and septic shock current (2010) controversy Etomidate known to suppress cortisol secretion Ability to mount a cortisol response is thought to be important to outcome in septic shock No studies to date clearly link Etomidate and increased mortality in septic shock Recommended approach: –Use another sedative? –Supplemental steroids if Etomidate used? –Draw cortisol level and give steroids if low?

27
Midazolam (Versed) Short acting benzodiazepine Dose: 0.1-0.3 mg/kg (larger dose /kg in kids; 10 mg usual max single dose for adults) Onset: 30-60 seconds Duration: 30-80 minutes Cautions: Reduces SVR, myocardial depressant
 Short acting benzodiazepine Dose: mg/kg (larger dose /kg in kids; 10 mg usual max single dose for adults) Onset: seconds Duration: minutes Cautions: Reduces SVR, myocardial depressant")
28
Ketamine Dose: 1-2 mg/kg IV, may give 4mg/kg IM Advantages: Bronchodilator as well as anesthetic; induction agent of choice in asthma. Disadvantages: Emergence reactions in adults (age > 15), increases ICP so contraindicated in head injury *For most RSI - other sedatives are preferable
, increases ICP so contraindicated in head injury *For most RSI - other sedatives are preferable.")
29
RSI Drugs – neuromuscular blockers (paralytics) Depolarizing NMBA – Succinylcholine Non-depolarizing NMBA – Vecuronium (Norcuron) – Rocuronium (Zemuron)
 Depolarizing NMBA – Succinylcholine Non-depolarizing NMBA – Vecuronium (Norcuron) – Rocuronium (Zemuron)")
30
Succinylcholine Ultra short-acting depolarizing neuromuscular blocker Dose:2.0 mg/kg IV Onset:45-60 seconds Duration:4-6 minutes Precautions:Burns or crush injuries greater than one week, increased intraocular pressure, hyperkalemia

31
Succinylcholine-induced hyperkalemic cardiac arrest Acetylcholine Receptor Up-regulation –Extensive burns, extensive muscle trauma (crush injuries) –Denervation: spinal cord injury, stroke, Guillain- Barre –Extensive atrophy or prolonged immobilization Myopathic Processes –Muscular dystrophy –Rare Idiopathic Granert, Anesthesiology. March 2001

32
K+ = 8

33
Rocuronium (Zemuron) Competitive nondepolarizing agent Dose:0.6 – 1.0 mg/kg IV Onset:70 seconds Duration:30 minutes Indications:When Succinylcholine is contraindicated, post-intubation paralysis
 Competitive nondepolarizing agent Dose:0.6 – 1.0 mg/kg IV Onset:70 seconds Duration:30 minutes Indications:When Succinylcholine is contraindicated, post-intubation paralysis")
34
Vecuronium (Norcuron) Competitive non-depolarizing agent Dose:0.1 mg/kg IV Onset:2-3 minutes Duration:45 minutes Indications:When succinylcholine is contraindicated, post-intubation paralysis
 Competitive non-depolarizing agent Dose:0.1 mg/kg IV Onset:2-3 minutes Duration:45 minutes Indications:When succinylcholine is contraindicated, post-intubation paralysis")
35
Whatever drugs and equipment you decide to use, always use a written reference or at least a calculator for drug doses, volumes and equipment needs

36
The rapid sequence Push sedative Push paralytic Position airway ( Sellick's maneuver may be used) Wait 45 seconds Do not ventilate unless the patient is hypoxic Laryngoscope and pass the tube Check the tube
 Wait 45 seconds Do not ventilate unless the patient is hypoxic Laryngoscope and pass the tube Check the tube")
37
Pass the tube (intubate) Wait 45-60 seconds after Succinylcholine Position airway after Succinylcholine Maintain in-line cervical immobilization in patients with suspected C-spine injury
 Wait seconds after Succinylcholine Position airway after Succinylcholine Maintain in-line cervical immobilization in patients with suspected C-spine injury")
38
Laryngoscopy Laryngeal anatomy (epiglottis, glottis, aryepiglottic folds, posterior cartilages, interarytenoid notch, vocal cords) Patient positioning, mouth opening, tongue Blade selection / light source Laryngeal manipulation / cricoid pressure Stylet shaping, ET tube railroading Pediatric, obese
 Patient positioning, mouth opening, tongue Blade selection / light source Laryngeal manipulation / cricoid pressure Stylet shaping, ET tube railroading Pediatric, obese")
39
Laryngoscopy practice Training videos Laryngoscopy courses Operating room opportunities Discuss cases with colleagues In studies, ED & OR intubation success rates increased from 40-90+% with training Practice will improve first pass success!

40
Failed airway Always be prepared for a failed airway First try to ventilate, then try again – Bag/valve/mask, Combitube/King tube, LMA If able to ventilate, try another technique – Fiberoptic intubation – Retrograde intubation – Use of bougie Unable to intubate or ventilate, then surgical airway

41
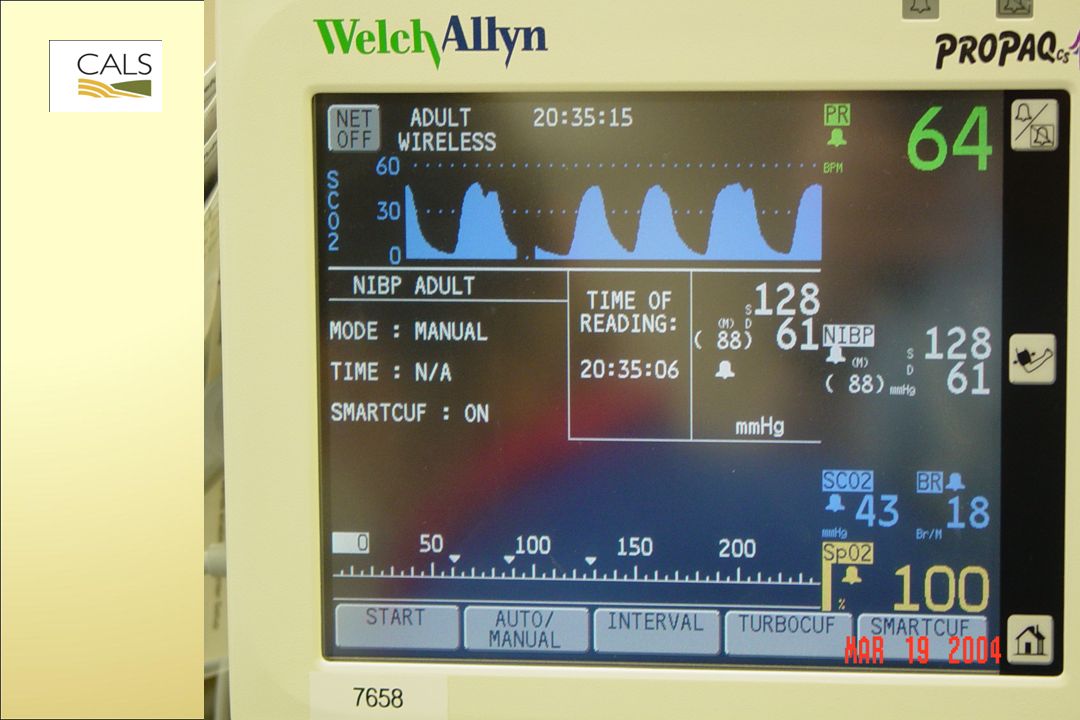
Patent airway assessment This is done immediately after intubation CO 2 detection with capnography or colorimetric device Suction device (esp. in cardiac arrest) Breath sounds, oximetry and X-ray confirm proper placement
 Breath sounds, oximetry and X-ray confirm proper placement.")
43
Post intubation management Secure tube Chest X-ray Continued SEDATION (Midazolam 0.1 mg/kg) and PARALYSIS (Vecuronium 0.15 mg/kg ) Maintain cervical spine immobilization Pass OG tube
 and PARALYSIS (Vecuronium 0.15 mg/kg ) Maintain cervical spine immobilization Pass OG tube")
44
Post-intubation management II Be aware of malignant hyperthermia: rare but lethal Check temperature at least once 15 -30 minutes after intubation and/or before transfer Watch for muscular rigidity especially masseter spasm, unexplained tachycardia, labile BP, increased End tidal CO 2 and increased temperature If suspected, follow CALS protocol and notify anesthesia/critical care/referral center

45
Anticipate the difficult airway Severe facial trauma Penetrating or blunt neck trauma Laryngeal edema or inhalation injuries Short neck, receding mandible Prominent upper incisors Limited mouth opening Limited ability to extend at atlanto-occipital joint

46
Mallampati airway classification

47
How would you handle this airway?

48
Management of Difficult Airway Tracheal tube introducer

49
Blind nasotracheal intubation Requires breathing, somewhat cooperative patient Anesthetize the airway with 4% Lidocaine and 1/2% Neo-synephrine Mild sedation Use standard ET tube without the stylet Pass tube gradually listening for increasing breath sounds Pass tube through cords on inspiration

50
Awake oral intubation Requires breathing, somewhat cooperative patient Anesthetize the airway with 4% Lidocaine and 1/2% Neo-synephrine Conscious sedation with Midazolam and Fentanyl Perform gentle laryngoscopy to attempt to visualize the cords May then give neuromuscular blocker If cords are seen, may attempt to pass the tube at that time or perform RSI

51
Case: Head injury 9 y/o fell off bicycle, hit head on large rock. Unconscious at scene. On arrival he was semi-conscious, moaning, and withdrawing to any painful stimulation. GCS = 10. BP 100/60, HR 102, R 16, SpO 2 100% on 10 LPM by NRB mask. Lungs clear with good air movement. Pupils - 3 mm, reactive. Motor exam - withdraws all extremities symmetrically.

52
Does he need to be intubated? If yes, when and how?

53
Head injury - 9 yr old Preoxygenate:100% O 2 Pretreatment:Lidocaine 1.5 mg/kg Atropine 0.02 mg/kg Sedation:Etomidate 0.3 mg/kg Paralytic:Succinylcholine 2 mg/kg Post intubation:Versed 0.1 mg/kg Vecuronium 0.15 mg/kg

55
Case: Asthma 5 y/o child with a history of asthma presents with severe difficulty breathing. On arrival she is only able to gasp out one word at a time. She appears mildly cyanotic on room air. BP 120/60, HR 160, R 30. O 2 started with Albuterol neb. IV established. ABGs pending. She becomes obtunded with decreasing respiratory effort.

56
How would you manage this patient?

57
Asthma: 5 yr old Preoxygenate:100% O 2 Pretreatment:Lidocaine 1.5 mg/kg, Atropine 0.02 mg/kg Sedation:Ketamine 1 - 2 mg/kg Versed 0.1 mg/kg Paralytic:Succinylcholine 2.0 mg/kg Post intubation:Versed 0.1 mg/kg Vecuronium 0.15 mg/kg

58
58 y/o in shock and respiratory failure

59
Nebulize: 4% Lidocaine, 0.5% phenylephrine

60
Insert endotracheal tube into nose

61
Successful awake intubation

62
Summary Most patients can and should be managed initially by good basic airway techniques Many critically ill or injured patients will benefit from intubation Intubation may be accomplished by several different techniques: RSI, blind nasal tracheal, cricothyrotomy, etc. –Always a planned procedure –Always a foolproof rescue plan

Similar presentations





, FAAP(PEM)>")









 5 3.>")






