Download presentation
Presentation is loading. Please wait.

1
sirolimus Sirolimus is a relatively new immunosuppressant drug used to prevent rejection in organ transplantation, and is especially useful in kidney transplants. It is also known as rapamycin. Sirolimus is a macrolide antibiotic ("-mycin") first discovered as a product of the bacterium Streptomyces hygroscopicus in a soil sample from an island called Rapa Nui. Rapamycin originally was developed as an antifungal agent. However,when it was discovered rapamycin had potent immunosuppressive. rejectionorgan transplantationkidneymacrolideantibioticRapa Nuirejectionorgan transplantationkidneymacrolideantibioticRapa Nui
 first discovered as a product of the bacterium Streptomyces hygroscopicus in a soil sample from an island called Rapa Nui. Rapamycin originally was developed as an antifungal agent. However,when it was discovered rapamycin had potent immunosuppressive. rejectionorgan transplantationkidneymacrolideantibioticRapa Nuirejectionorgan transplantationkidneymacrolideantibioticRapa Nui.")
2
Chemical structure: Formula C51 C79 NO31

3
Physical properties: Names: Rapamycin, sirolimus, rapamune Melting point 183-185 C Mol. Wt. 914.18

4
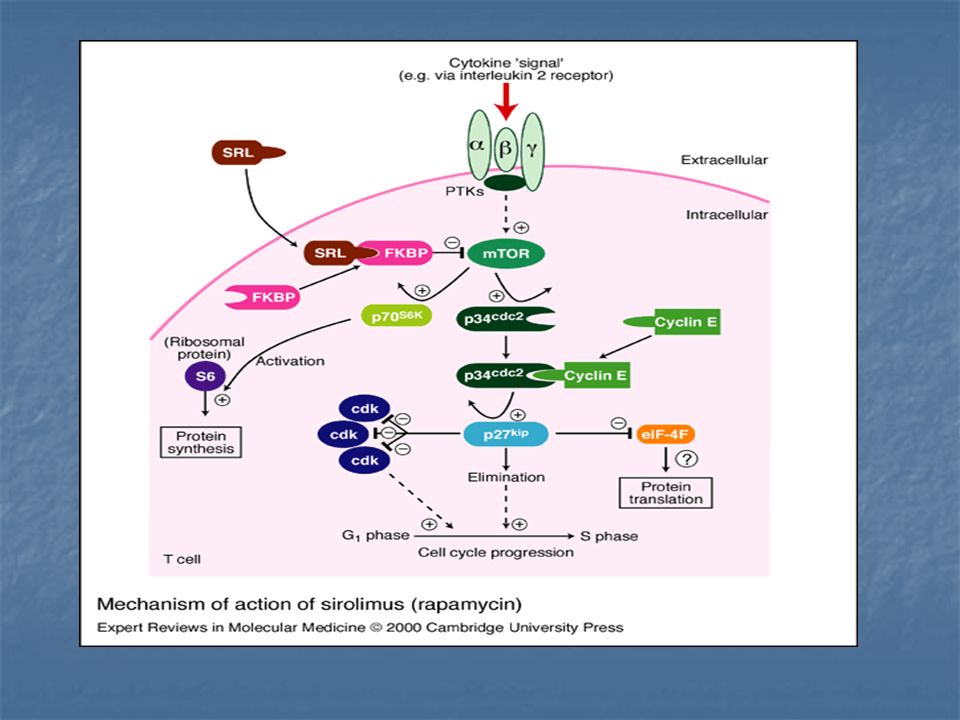
Mechanism of Action: RAPA blocks T lymphocyte proliferation. RAPA ’ s effects are not limited to IL-2- or IL-4 mediated growth of T cells, as it has been found to inhibit IL-12, IL-7, and IL-15 driven proliferation of activated T cells RAPA blocks cell cycle progression in mid-to-late G1 phase, RAPA blocks lymphocyte proliferation. RAPA inhibits IL-2 dependent and independent proliferation of purified normal human B lymphocytes stimulated with Staphylococcus aureus (SA). It also prevents SA and IL-2 or IL-6 dependent differentiation into antibody-producing cells, thereby decreasing IgM, IgG and IgA production. SRL binding to specific cytosolic binding proteins called immunophilins (FKBPs). This complex inhipits isomerase activity (PPlase). FKBP 12 is the most relevant binding protein for the immunosuppressive effects of RAPA. Mechanism of Action: RAPA blocks T lymphocyte proliferation. RAPA ’ s effects are not limited to IL-2- or IL-4 mediated growth of T cells, as it has been found to inhibit IL-12, IL-7, and IL-15 driven proliferation of activated T cells RAPA blocks cell cycle progression in mid-to-late G1 phase, RAPA blocks lymphocyte proliferation. RAPA inhibits IL-2 dependent and independent proliferation of purified normal human B lymphocytes stimulated with Staphylococcus aureus (SA). It also prevents SA and IL-2 or IL-6 dependent differentiation into antibody-producing cells, thereby decreasing IgM, IgG and IgA production. SRL binding to specific cytosolic binding proteins called immunophilins (FKBPs). This complex inhipits isomerase activity (PPlase). FKBP 12 is the most relevant binding protein for the immunosuppressive effects of RAPA.
. It also prevents SA and IL-2 or IL-6 dependent differentiation into antibody-producing cells, thereby decreasing IgM, IgG and IgA production. SRL binding to specific cytosolic binding proteins called immunophilins (FKBPs). This complex inhipits isomerase activity (PPlase). FKBP 12 is the most relevant binding protein for the immunosuppressive effects of RAPA. Mechanism of Action: RAPA blocks T lymphocyte proliferation. RAPA ’ s effects are not limited to IL-2- or IL-4 mediated growth of T cells, as it has been found to inhibit IL-12, IL-7, and IL-15 driven proliferation of activated T cells RAPA blocks cell cycle progression in mid-to-late G1 phase, RAPA blocks lymphocyte proliferation. RAPA inhibits IL-2 dependent and independent proliferation of purified normal human B lymphocytes stimulated with Staphylococcus aureus (SA). It also prevents SA and IL-2 or IL-6 dependent differentiation into antibody-producing cells, thereby decreasing IgM, IgG and IgA production. SRL binding to specific cytosolic binding proteins called immunophilins (FKBPs). This complex inhipits isomerase activity (PPlase). FKBP 12 is the most relevant binding protein for the immunosuppressive effects of RAPA..")
6
Pharmacokinetics: 1-Adminstration: Oral solution or tablets. 2-Absorption: SRL reaches maximum concentration in the blood in 2 h with the solution, compared to 6 h with the tablet formulation. Oral bioavailability is low (around 15% when administered with cyclosporine A (CsA)). 3-distribution: Due to its lipophilic nature, SRL is extensively distributed to fatty tissues and so has a large volume of distribution (5.6 – 16.7 L/kg). Within plasma, SRL is extensively bound to plasma proteins. SRL has a long half-life (60 h) so, when commencing SRL, a loading dose is necessary. 4-metabolism: The metabolites of SRL are inactive.Sirolimus is metabolized by the cytochrome P450 – 3A4 Isoenzyme so its effected by enzyme inducers &inhibitor. The clearance of SRL approximates that of liver blood flow, so dose reductions may be needed in patients with hepatic impairment. 5-excretion: SRL is excreted by the liver.
). 3-distribution: Due to its lipophilic nature, SRL is extensively distributed to fatty tissues and so has a large volume of distribution (5.6 – 16.7 L/kg). Within plasma, SRL is extensively bound to plasma proteins. SRL has a long half-life (60 h) so, when commencing SRL, a loading dose is necessary. 4-metabolism: The metabolites of SRL are inactive.Sirolimus is metabolized by the cytochrome P450 – 3A4 Isoenzyme so its effected by enzyme inducers &inhibitor. The clearance of SRL approximates that of liver blood flow, so dose reductions may be needed in patients with hepatic impairment. 5-excretion: SRL is excreted by the liver..")
7
Pharmacological Action: *Sirolimus does not block IL production by activated T cells but instead blocks the response of T cells to cytokines. *It is a potent inhibitor of B cell proliferation &immunoglobulin Production. *Sirolimus also inhibits the mononuclear cell proliferative response to colony stimulation factors &suppresses hematopoietic recovery after myelotoxic treatment in mice. * sirolimus displayed comparatively lower platelet and white blood cell counts. * SRL increases total cholesterol, LDL, triglycerides, apoB- 100, and apoC-III; these effects are repeatable, dose-dependent and reversible. * Sirolimus causes anaemia, thrombocytopaenia and leukopaenia due to bone marrow suppression.

8
Sirolimus in CVS: SRL has not been shown so far to increase cardiovascular morbidity or mortality but SRL may improve the cardiovascular risk of patients post- transplantation. In cardiac allograft recipients treated with CsA and steroids, SRL was found to be superior to azathioprine in preventing cardiac transplant vasculopathy. SRL is associated with less hypertension compared to CNI-based regimes and may be less diabetogenic, but does increase lipid levels.

9
Therapeutic Uses: A- In Adult: 1- Kidney : sirolimus as a primary agent with cyclosporine and prednisone reduced the overall incidence of acute allograft rejection episodes from 32 to 7.5%. 2-Islet: In a widely heralded initial experience, reported the successful use of sirolimus as a primary immunosuppressive agent in seven patients with type 1 diabetes who underwent islet cell transplantation. This glucocorticoid-free regimen combined sirolimus, tacrolimus, and daclizumab. 3-liver: Sirolimus has been used in combination with tacrolimus after liver transplantation to allow the subtherapeutic use of tacrolimus.

10
B-In Children: Pharmacokinetics different in children compared with adults. Half-life (h) of sirolimus is shorter in children because of rapid metabolism and some children may need twice a day dosing. 1-Kidney: Studies in children using sirolimus for primary immunosuppression are still limited. 2-Liver: Sirolimus was used as primary immunosuppression in combination with subtherapeutic tacrolimus. 3- Intestine: Addition of sirolimus to a tacrolimus decreased early rejection and improved graft survival in children and adults receiving intestinal transplants compared with control.
 of sirolimus is shorter in children because of rapid metabolism and some children may need twice a day dosing. 1-Kidney: Studies in children using sirolimus for primary immunosuppression are still limited. 2-Liver: Sirolimus was used as primary immunosuppression in combination with subtherapeutic tacrolimus. 3- Intestine: Addition of sirolimus to a tacrolimus decreased early rejection and improved graft survival in children and adults receiving intestinal transplants compared with control..")
11
C- In Cancer: The anti-proliferative effects of sirolimus may have a role in treating cancer. Recently, it was shown that sirolimus inhibited the progression of dermal Kaposi's sarcoma in patients with renal transplants. As with all immunosuppressive medications, rapamycin decreases the body's inherent anti-cancer activity and allows some cancers which would have been naturally destroyed to proliferate. Kaposi's sarcomaKaposi's sarcoma

12
Adverse Effect: A- Major Adverse Effect: 1- Hyperlipidaemia: A major effect on lipid metabolism. SRL increases total cholesterol, LDL, triglycerides, apoB- 100, and apoC-III; these effects are repeatable, dose- dependent and reversible. 2-Wound Complications: Sirolimus is associated with a high wound complication in the early stages post-transplantation, with rates varying between 6 – 15% due to its anti-proliferative properties Wound complications include delayed wound healing, lymphocoele, haematoma, incisional hernia and relaparotomy for wound complication. Adverse Effect: A- Major Adverse Effect: 1- Hyperlipidaemia: A major effect on lipid metabolism. SRL increases total cholesterol, LDL, triglycerides, apoB- 100, and apoC-III; these effects are repeatable, dose- dependent and reversible. 2-Wound Complications: Sirolimus is associated with a high wound complication in the early stages post-transplantation, with rates varying between 6 – 15% due to its anti-proliferative properties Wound complications include delayed wound healing, lymphocoele, haematoma, incisional hernia and relaparotomy for wound complication.

13
3- Haematological: Sirolimus causes anaemia, thrombocytopaenia and leukopaenia due to bone marrow suppression, but rarely leads to discontinuation of therapy. 4- Thrombosis: SRL was not associated with an increased risk of deep vein thrombosis (DVT), but the DVT that did develop were preceded by lymphocoele in threequartersof cases. 5-Oral Ulcers: Initially, it was assumed that these aphthous ulcers were due to herpes simplex infection but this has not been confirmed and it is now assumed that they result from a direct toxic effect of SRL. 6- Lung Toxicity: In a phase II trial of SRL, an increased incidence of Pneumocystis carinii pneumonia (PCP) was reported in a single centre that did not use routine PCP prophylaxis.
, but the DVT that did develop were preceded by lymphocoele in threequartersof cases. 5-Oral Ulcers: Initially, it was assumed that these aphthous ulcers were due to herpes simplex infection but this has not been confirmed and it is now assumed that they result from a direct toxic effect of SRL. 6- Lung Toxicity: In a phase II trial of SRL, an increased incidence of Pneumocystis carinii pneumonia (PCP) was reported in a single centre that did not use routine PCP prophylaxis..")
14
Drug – Drug Interaction: Sirolimus and CNI are both metabolized by the cytochrome p450 3A4 isoenzyme. SRL blood concentration is 30% higher with CsA To minimize this interaction, SRLshould be given 4 h after CsA. SRL does not appear to have a pharmacokinetic interaction with tacrolimus. Mycophenolic acid AUC is higher when SRL and mycophenolate mofetil (MMF) does not affect SRL exposure. compared to co-administration of SRL and CsA. Enzymes inhibitor increase its concentration. Enzymes inducer decrease its concentration.
 does not affect SRL exposure. compared to co-administration of SRL and CsA. Enzymes inhibitor increase its concentration. Enzymes inducer decrease its concentration..")
15
Dosage: The maintenance sirolimus doses ranged from 0.5 to 15 mg once daily. The dose was only reduced in the presence of drug – indused toxicity. Missed Dose: Do not double doses. If you miss a dose of sirolimus and remember it within 12 hours, take the missed dose as soon as you remember. However, if it is almost time for the next dose, skip the missed dose, go back to your regular dosing schedule, and check with your doctor.

16
Sirolimus Monotherapy: Monotherapy to 29 primary renal transplant patients show acute rejection developed in eightout of 29 (five of which were antibody- mediated). One graft was lost to rejection. All other patients tolerated therapy well. Combination Therapy: A-with CsA: show reduction in the incidence of acute allograft rejection episodes to 7.5% over3 years. B-with tacrolimus: SRL and TRL might compete for FK-binding proteins (FKBP), producing antagonistic effects, the large amount of cytosolic FKBP seems to obviate this possibility.
, producing antagonistic effects, the large amount of cytosolic FKBP seems to obviate this possibility..")
Similar presentations









>")







 The measure of the apparent space in the body available to contain.>")

 reactivation and immunosupression in allogeneic transplantation Marie Waller Bone Marrow Transplant Coordinator Manchester Royal.>")