Download presentation
Presentation is loading. Please wait.

1
Poisoning and child safety Block 10 Dr Mulaudzi M.C Paediatrics UP

2
General info Most common in the age group 1-5 yrs olds Route of poisoning skin contamination Inhaled fumes Ingestion-this is the most common form of poisoning Eye contamination Major poisons Medicines and drugs left where children can reach Paraffin Cleaning liquids insecticides Death from poisoning is an unnatural death

3
General information Poisoning can be accidental, suicidal or Para suicidal When there is use of traditional medicine remember to look for the underlying disease. Older children needs psychologist Parents often need counselling Nature of accident Prevention of accidental poisoning in future Crisis management esp. when child severely ill or dies or complications

4
Major patterns of presentation Change in level of consciousness/coma Respiratory distress Metabolic acidosis Gastrointestinal complaints Abnormal cardiac rhythm convulsions

5
Other Recognized syndromes in presentation of poisoning in children 1.Increased sympathetic activity 2.Anti-cholinergic activity 3.Cholinergic activity 4.Metabolic acidosis

6
Increased sympathetic nervous system activity Symptoms – Pyrexia – Flushing – Tachycardia – Pupilary constriction – Hypertension – sweating Possible toxins – Cough and cold preparations – Amphetamines – Cocaine – Ecstasy – theophylines

7
Anti-cholinergic activity Symptoms – Pupilary dilatation – Dry mouth Possible toxins – Tricyclic antidepressants – Antihistamines – Mushroom – Drugs for parkinsonism

8
Increased parasympathetic activity (Cholinergic) Symptoms – Pupilary constriction – Salivation – Diarrhoea – Urinary incontinence – Muscle fasciculation – paralysis Possible toxins – Organophosphates pesticides – Pyridostigmine (Rx for myasthenia gravis)
 Symptoms – Pupilary constriction – Salivation – Diarrhoea – Urinary incontinence – Muscle fasciculation – paralysis Possible toxins – Organophosphates pesticides – Pyridostigmine (Rx for myasthenia gravis)")
9
Metabolic Acidosis Symptoms – Tachypnoea – Kussmaul breathing Possible toxins – Salicylates – Ethanol – Diabetic oral meds – Carbon monoxides – Iron

10
Management of children presenting with poisoning

11
Management principles First aid at home Resuscitation (ABC) Supportive therapy Eliminating and preventing absorption of the poison/toxin : – Emesis – Gastric lavage – Activated charcoal Specific poisons and antidotes Prevention
 Supportive therapy Eliminating and preventing absorption of the poison/toxin : – Emesis – Gastric lavage – Activated charcoal Specific poisons and antidotes Prevention")
12
First aid at home Inhaled: remove from the gas, open windows and doors, get fresh air Skin contamination : remove all clothes wash with water then with soap Eye contact : irrigate with Lukewarm water Ingested poisons : do not induce vomiting in following conditions – Depressed level of consciousness – Hydrocarbons, paraffin, acids, alkali

13
Resuscitation and Supportive care Adequate airway and ventilation Treatment of hypoglycaemia Treat volume depletion and hypotension Treat convulsions Investigations: – UKE, LFT,anion gap, blood gas, glucose, FBC, clotting profile, urine analysis and ECG may be more rewarding than toxic screen

14
Emesis Is of value up to six hours of ingestion Epecacuanha may be used Contra-indications – Depressed level of consciousness – coma – Convulsions – Hydrocarbons, petroleum products, paraffin – Poisoning with corrosives, acids and alkali

15
Gastric lavage Effective within 2 hrs of ingestion Contraindication Comatose unless ETT is inserted Volatile hydrocarbons, petroleum products Corrosives, acids, alkali Procedure Position on left side with head in slightly lower position than the body Saline is used

16
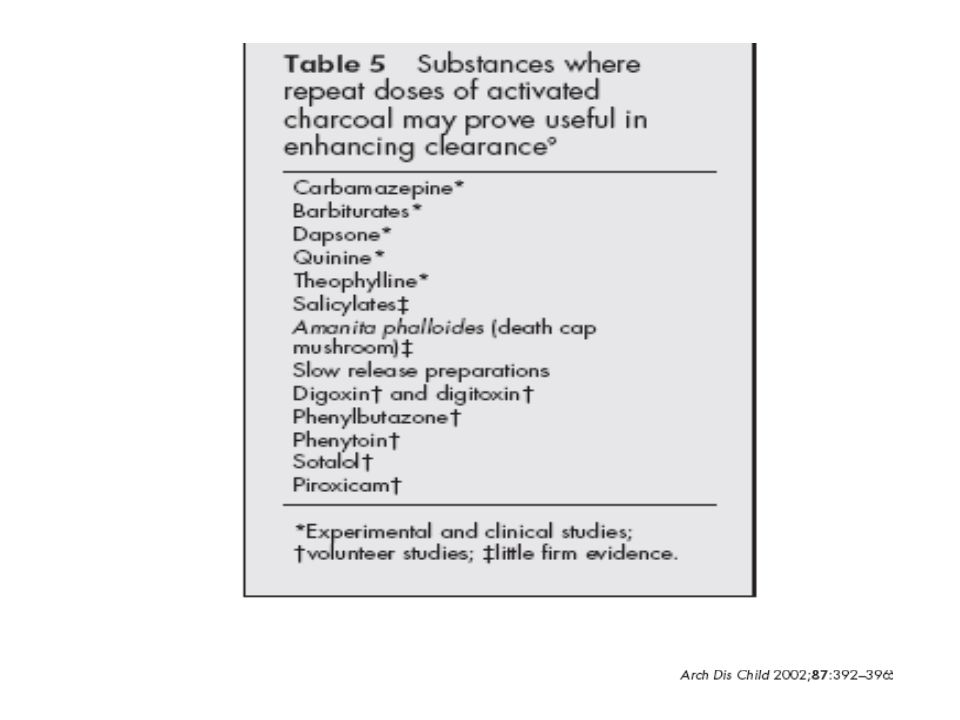
Activated charcoal Binds and minimize the absorption of the poison Not of benefit in corrosives, and not very effective in poisoning due to lithium, organophosphates, petroleum products and organic solvents like methanol, ethylene glycol. Maximal benefit within 1 hour of ingestion S/Evomiting, constipation, gastrointestinal obstruction and perforation Given oral/via NGT 10g in 100mls of water and in children >6 yrs 20-50g in 100-300mls of water

18
Specific poisons Salicylates Tricyclic anti-depressants Paracetamol Organophosphate/Carbamates Hydrocarbons Caustic agents Others

19
Salicylate poisoning Source: oral and or topical Features: Hyperventilation, fever, respiratory failure, CNS depression Pathology Uncoupling of oxidative phosphorylation resulting in – metabolic acidosis- tachypnoea, Kausmal breathing – Hepatotoxicity – Glucose metabolism disturbances Investigations Salicylate levels Supportive - glucose, electrolytes, blood gas, urine output, liver functions and ammonia to exclude Reye’ syndrome Treatment General measures Correct hypoglycaemia, dehydration, and acidosis Sodium bicarbonate infusion to maintain urine pH above 7.5 Dialysis may be done in severe cases

20
Tricyclic anti depressants Problem therapeutic/toxic ratio is narrow Symptoms - Get anti-cholinergic effects Delirium, fever, dry mouth, tachycardia, urinary retention, dilated pupils arrhythmias Treatment “Tri”: Induce emesis, do gastric lavage, administer activated charcoal. Monitor for arrhythmias and treat when present Keep the pH between 7,45 and 7,55 with the use of sodium bicarbonate infusion

21
Paracetamol Common agent in suicide attempt with adolescents Pathology - centrilobular necrosis of the liver Clinical features usually delayed for 48 to 72 hrs Nausea, vomiting, pallor, jaundice, liver failure Treatment Use activated charcoal N-acetylcysteine is given (most effective within 16 hrs of ingestion) Paracetamol levels helps to give prognoses
 Paracetamol levels helps to give prognoses")
22
Organophosphates and carbamates Used as insecticides Poisoning due to organophosphate is a notifiable condition Pathology Inhibition of cholinesterase resulting in accumulation of acetylcholine Clinical features Muscuranic symptoms: Salivation, sweating, increased bronchial secretion, diarrhoea, pinpoint pupils Nicotinic symptoms: fasciculation, confusion, convulsion, and coma Treatment General measures Atropine initially at a dose of 0.05mg/kg then a continuous infusion Pralidoxime may be given with organophosphate, it disrupt the phosphate-cholinesterase bond

23
Volatile Hydrocarbons E.g paraffin, thinners Clinical presentation Aspiration or inhalation causing a chemical pnuemonitis CNS depression Fever Paraffin may be associated with fires and burns Treatment No emesis or gastric lavage Maintaining hydration, oxygenation Relieving fever

24
Caustic agents Presentation Dysphagia, epigastric pain, oral mucosal burns, and low grade fever and drooling Patients with oesophageal lesions may not have oral lesions Alkali tend to cause more damage than acids because acids may limit the injury because of the bitter/sour taste Therapy Initially, dilution by drinking milk or water vomiting should not be attempted Latter depends on the degree of injury to the oesophagus Endoscope if persistent dysphagia and drooling Referral to paediatric surgeons

25
Others Carbon monoxide Headaches, dizziness, coma, skin bullae Treatment with 100%, hyperbaric oxygen Prescribed drugs E,G digoxin, phenothiazines, iron, benzodiazepines, betablockers, etc some have their specific antidotes

26
Specific antidote

27
Prevention safe keeping of medicines and cleaning agents preferably in a lockable cupboard or child proof cupboards Do not tell your children that your tablets are adults sweets Children should not take their medicine unsupervised Return or dispose your unused medicine properly (return them back to pharmacy) Empty the suspensions down the drain Do not leave alcohol, medicines, cleaning agents within reach for children Be careful and read labels especially with over the counter medicines
 Empty the suspensions down the drain Do not leave alcohol, medicines, cleaning agents within reach for children Be careful and read labels especially with over the counter medicines")
28
Prevention Paraffin and pesticides Never place non-edible products in food containers or visa versa e.g. paraffin in a juice/milk or cool drink bottles Use funnel to refill paraffin appliances rather than a cup Water to drink should be accessible for children to drink otherwise they will drink paraffin Before applying pesticides remove children and their toys Children need constant supervision

29
Prevention child safety Prevent chocking – Keep small object out of reach of small children – A plastic bag can be lethal to a child – Do not give small children peanuts Prevent children from drowning – Pools appropriately secured – Children can drown from buckets and bath there should not be left unsupervised in the bath or around buckets filled with water – Empty bath and container after use Prevent other injuries from falling drowning – Most accidents happen after nappy change – Use safety rail on a bed or use a cot to prevent fall

30
Emergency contacts Know emergency casualty numbers for hospitals in your area Poisoning centre number: 0800 333 444 Tygerberg Hospital 021 931 6129 Red cross hospital: 012 658 5428 Police: 10 111

Similar presentations





 in the lungs and in the.>")



 needed to regulate blood glucose levels is ineffective; Glucose levels can get too high or too low Type I - patients.>")


 enquiries.>")






