Download presentation
Presentation is loading. Please wait.

1
LEUKEMIA Dr. Mohamed Haseen Basha Assistant professor ( Paediatrics) Faculty of Medicine Al Maarefa College of Science and Technology
 Faculty of Medicine Al Maarefa College of Science and Technology.")
2
Hematopoietic Stem Cell Differentiation

3
Paediatric Malignancy Accounts for 10% of deaths in childhood Leukaemia 30% Lymphoma 10% Solid tumours: the rest, i.e. 60%

4
LEUKEMIA “The leukemias may be defined as a group of malignant diseases in which genetic abnormalities in a hematopoietic cell give rise to an unregulated clonal proliferation of cells.” A group of malignant disorders affecting the blood and blood forming tissues of Bone marrow, Lymph system, Spleen. Results in an accumulation of dysfunctional cells because of a loss of regulation in cell division

5
The leukemias are the most common malignant neoplasms in childhood, accounting for approximately 31% of all malignancies that occur in children younger than 15 yr of age. Acute lymphoblastic leukemia (ALL) accounts for approximately 77% of cases of childhood leukemia, acute myelogenous leukemia (AML) for approximately 11%, chronic myelogenous leukemia (CML) for 2-3%, and juvenile myelomonocytic leukemia (JMML) for 1-2%.
 accounts for approximately 77% of cases of childhood leukemia, acute myelogenous leukemia (AML) for approximately 11%, chronic myelogenous leukemia (CML) for 2-3%, and juvenile myelomonocytic leukemia (JMML) for 1-2%..")
6
Etiology and Pathophysiology No single causative agent Most from a combination of factors Genetic and environmental influences Associated with the development of leukemia Chemical agents Chemotherapeutic agents Viruses Radiation Immunologic deficiencies

7
Classification Acute versus chronic Cell maturity Acute: clonal proliferation of immature hematopoietic cells Chronic: mature forms of WBC; onset is more gradual Nature of disease onset Type of white blood cell (WBC) Acute lymphocytic leukemia (ALL) Acute myelogenous leukemia (AML) Chronic myelogenous leukemia (CML) Chronic lymphocytic leukemia (CLL)
 Acute lymphocytic leukemia (ALL) Acute myelogenous leukemia (AML) Chronic myelogenous leukemia (CML) Chronic lymphocytic leukemia (CLL)")
8
Clinical Manifestations Relate to problems caused by Bone marrow failure Overcrowding by abnormal cells Inadequate production of normal marrow elements Anemia, thrombocytopenia, ↓ number and function of WBCs Leukemic cells infiltrate patient’s organs Splenomegaly Hepatomegaly Lymphadenopathy Bone pain, meningeal irritation, oral lesions (chloromas)
")
9
Clinical Approach to Leukemia History Fever Pallor- increasingly pale with time, Weakness, fatigue, Giddiness, Anorexia, Palpitation, breathlessness, No response to iron therapy. Bleeding manifestations - Petechiae ( 10 mm), gum bleeding, epistaxis, hematemesis, malena and hemoptysis Lump in the abdomen Swelling in the neck Convulsions Signs of congestive cardiac failure Pruritis Facial swelling, dysphagia -signs of mediastinal compression
, gum bleeding, epistaxis, hematemesis, malena and hemoptysis Lump in the abdomen Swelling in the neck Convulsions Signs of congestive cardiac failure Pruritis Facial swelling, dysphagia -signs of mediastinal compression.")
10
GENERAL PHYSICAL EXAMINATION Vitals Anthropometry Pallor / Clubbing / cyanosis / edema feet Lymphadenopathy (lymphoma/leukemia/infectious mononucleosis) Jaundice Sternal tenderness (acute leukemia) Any hemorrhagic manifestation (hemorrhage in to skin, epistaxis, gum bleeding, hemarthrosis, hematuria) Examination of the mouth (oral cavity) and skin thoroughly Ophthalmic examination for any retinal hemorrhage, exudate, papilledema
 Jaundice Sternal tenderness (acute leukemia) Any hemorrhagic manifestation (hemorrhage in to skin, epistaxis, gum bleeding, hemarthrosis, hematuria) Examination of the mouth (oral cavity) and skin thoroughly Ophthalmic examination for any retinal hemorrhage, exudate, papilledema")
11
DIFFERENTIAL DIAGNOSIS Leukemoid reaction: Bacterial infection, acute hemolysis, tuberculosis, sarcoidosis, histoplamosis or metastatic tumors, Increased WBC (up to 50 × 109/l) and peripheral immature granulocyte precursors are seen. Lymphocytosis: Pertussis and other viral infections, Infants and small children often have physiological lymphocytosis Infectious mononucleosis: Aplastic anemia: Pancytopenia and hypoplastic bone marrow. Idiopathic thrombocytopenic purpura(ITP): Patients with ITP do not have anemia (with exception of children with severe bleeding) and have normal morphology of white blood cell differentiation.
: Patients with ITP do not have anemia (with exception of children with severe bleeding) and have normal morphology of white blood cell differentiation..")
12
Bone marrow infiltration by a solid tumor (metastatic disorder): Neuroblastoma (increased level of urine catecholamines) Non-Hodgkin lymphoma (NHL with more than 25% of blasts in the bone marrow are defined as leukemia) Rhabdomyosarcoma and retinoblastoma may have a similar infiltration of the bone marrow as leukemia, but they generally have clusters of malignant cells. Rheumatoid fever and rheumatoid arthritis can often be confused with leukemia (because bone pain is present in 25% of leukemia cases), but alteration of peripheral blood cell count and bone marrow abnormalities are not seen.
, but alteration of peripheral blood cell count and bone marrow abnormalities are not seen..")
13
Diagnostic Studies To diagnose and classify – Peripheral blood evaluation (CBC and blood smear) – Bone marrow evaluation To identify cell subtype and stage – Morphologic, histochemical, immunologic, and cytogenic methods
 – Bone marrow evaluation To identify cell subtype and stage – Morphologic, histochemical, immunologic, and cytogenic methods")
14
INVESTIGATIONS Complete Blood Count Red Cells Hb is often moderate to low, Low number of reticulocytes. White Blood Cell Count Number of white blood cells can be normal, low or high, In children with leucopenia, few or no atypical lymphoblasts are detected. In children with a high WBC, leukemic blast cells are often present In children with a high WBC (more than 100 × 10 9 white blood cells/L) the lymphoblasts are predominant (together with marked visceromegaly). Platelets The platelet count is usually low 50% of children less than 50 × 10 9 /L Spontaneous hemorrhage appears in children with less than 20-30 × 10 9 platelets/L.
 the lymphoblasts are predominant (together with marked visceromegaly). Platelets The platelet count is usually low 50% of children less than 50 × 10 9 /L Spontaneous hemorrhage appears in children with less than × 10 9 platelets/L..")
15
Serum Chemistry Serum Chemistry Hyperuricemia: Uric acid level is often high initially. Hyperkalemia: (due to massive cell lysis) Hypokalemia (potassium level may be low in malnourished or due to renal tubular loss) Hypocalcemia (due to renal insufficiency or due to calcium binding to phosphate released by leukemic cells) Hypercalcemia (due to marked leukemic bone infiltration) Abnormal liver function tests like increased level of transaminases with/without hyperbilirubinemia (due to liver infiltration by leukemic cells or as a side effect of treatment) Serum immunoglobulin levels: In 20% of children with ALL low serum IgG and IgM levels.
 Hypokalemia (potassium level may be low in malnourished or due to renal tubular loss) Hypocalcemia (due to renal insufficiency or due to calcium binding to phosphate released by leukemic cells) Hypercalcemia (due to marked leukemic bone infiltration) Abnormal liver function tests like increased level of transaminases with/without hyperbilirubinemia (due to liver infiltration by leukemic cells or as a side effect of treatment) Serum immunoglobulin levels: In 20% of children with ALL low serum IgG and IgM levels..")
16
Bone Marrow Analysis Bone marrow analysis serves to characterize the blast cells and to determine hyper or hypocellularity It can be used for morphological, immunological, biochemical, and cytogenetic analyses. To rule out aplastic anemia and myelodysplastic syndrome.

17
Cytogenetics In 85% of children with leukemia, an abnormal karyotype in the malignant clone is detectable. The analysis combines chromosome banding with fluorescence in situ hybridization (FISH) with spectral karyotyping and with comparative genomic hybridization. The cytogenetic abnormalities reflect the number of chromosomes (ploidy) and the structure of chromosomes (rearrangements). Translocation t(9;22) (BCR-ABL fusion protein) is present in 5% of children with ALL and is characteristic of a protein with tyrosine kinase activity with the ability to immortalize progenitors and is correlated with an unfavorable prognosis.
 with spectral karyotyping and with comparative genomic hybridization. The cytogenetic abnormalities reflect the number of chromosomes (ploidy) and the structure of chromosomes (rearrangements). Translocation t(9;22) (BCR-ABL fusion protein) is present in 5% of children with ALL and is characteristic of a protein with tyrosine kinase activity with the ability to immortalize progenitors and is correlated with an unfavorable prognosis..")
18
Flow Cytometry Flow cytometry can measure the DNA and RNA content of individual cells. It provides: incidence of cells in different phases of the cell cycle, determination of the DNA content of leukemic cells for prognosis. The DNA index (DI) defines the cellular DNA content determined by flow cytometry
 defines the cellular DNA content determined by flow cytometry.")
19
Management Goal is to attain remission (when there is no longer evidence of cancer cells in the body) Chemotherapeutic treatment – Induction therapy Attempt to induce or bring remission Seeks to destroy leukemic cells in the tissues, peripheral blood, bone marrow Patient may become critically ill – Provide psychological support as well
 Chemotherapeutic treatment – Induction therapy Attempt to induce or bring remission Seeks to destroy leukemic cells in the tissues, peripheral blood, bone marrow Patient may become critically ill – Provide psychological support as well")
20
– Intensification therapy High-dose therapy May be given after induction therapy Same drugs at higher doses and/or other drugs – Consolidation therapy Started after remission is achieved Purpose is to eliminate remaining leukemic cells that may not be evident – Maintenance therapy Lower doses of the same drug

21
Combination chemotherapy – Mainstay treatment – 3 purposes ↓ drug resistance ↓ drug toxicity to the patient by using multiple drugs with varying toxicities Interrupt cell growth at multiple points in the cell cycle

22
Bone Marrow and Stem Cell Transplantation Goal Totally eliminate leukemic cells from the body using combinations of chemotherapy with or without total body irradiation Eradicates patient’s hematopoietic stem cells Replaced with those of an HLA-matched (Human Leukocyte Antigen) Sibling Volunteer Identical twin Patient’s own stem cells removed before
 Sibling Volunteer Identical twin Patient’s own stem cells removed before")
23
ACUTE LYMPHOBLASTIC LEUKEMIA

24
ALL peak incidence at 2-3 yr of age and occurs more in boys than in girls. The disease is more common in children with certain chromosomal abnormalities, such as Down syndrome, Bloom syndrome, ataxia- telangiectasia, and Fanconi anemia. Among identical twins, the risk to the second twin if 1 twin develops leukemia is greater than that in the general population.

25
ETIOLOGY Etiology of ALL is unknown, although several genetic and environmental factors are associated with childhood leukemia. Most cases of ALL are thought to be caused by post conception somatic mutations in lymphoid cells. Exposure to medical diagnostic radiation both in utero and in childhood is associated with an increased incidence of ALL. In certain developing countries, there is an association between B-cell ALL (B-ALL) and Epstein-Barr viral infections.
 and Epstein-Barr viral infections..")
26
Factors predisposing to Childhood Leukemia

27
Classification of ALL

28
Common chromosomal abnormalities in ALL

29
CLINICAL MANIFESTATIONS initial presentation of ALL usually is nonspecific and relatively brief. Anorexia, fatigue, malaise, and irritability often are present, as is an intermittent, low-grade fever. Bone or joint pain, particularly in the lower extremities may be of several months’ duration, can include joint swelling. Bone pain is severe and can wake the patient at night. As the disease progresses, Bone marrow failure - pallor, fatigue, exercise intolerance, bruising, or epistaxis, as well as fever, which may be caused by infection or the disease. Organ infiltration - lymphadenopathy, hepatosplenomegaly, testicular enlargement, or central nervous system (CNS) involvement (cranial neuropathies, headache, seizures). Respiratory distress - severe anemia or mediastinal node compression of the airways.
 involvement (cranial neuropathies, headache, seizures). Respiratory distress - severe anemia or mediastinal node compression of the airways..")
30
On physical examination, findings of pallor, listlessness, purpuric and petechial skin lesions, or mucous membrane hemorrhage can reflect bone marrow failure. The proliferative nature of the disease -lymphadenopathy, splenomegaly, or, less commonly, hepatomegaly. patients with bone or joint pain, there may be exquisite tenderness over the bone or objective evidence of joint swelling and effusion. Nonetheless, with marrow involvement, deep bone pain may be present but tenderness will not be elicited. Rarely, show signs of increased intracranial pressure that indicate leukemic involvement of the CNS. These include papilledema, retinal hemorrhages, and cranial nerve palsies.

31
Respiratory distress related to anemia but can occur in patients with an obstructive airway problem (wheezing) as the result of a large anterior mediastinal mass (e.g., in the thymus or nodes). This problem is most typically seen in adolescent boys with T-cell ALL (T-ALL). T-ALL also usually has a higher leukocyte count. B-lymphoblastic leukemia is the most common immunophenotype, with onset at 1-10 yr of age. The median leukocyte count at presentation is 33,000/μL, thrombocytopenia is seen in 75% of patients, and hepatosplenomegaly is seen in 30-40% of patients. In all types of leukemia, CNS symptoms are seen at presentation in 5% of patients (5-10% have blasts in the cerebrospinal fluid [CSF]). Testicular involvement is rarely evident at diagnosis,
. T-ALL also usually has a higher leukocyte count. B-lymphoblastic leukemia is the most common immunophenotype, with onset at 1-10 yr of age. The median leukocyte count at presentation is 33,000/μL, thrombocytopenia is seen in 75% of patients, and hepatosplenomegaly is seen in 30-40% of patients. In all types of leukemia, CNS symptoms are seen at presentation in 5% of patients (5-10% have blasts in the cerebrospinal fluid [CSF]). Testicular involvement is rarely evident at diagnosis,.")
32
DIAGNOSIS The diagnosis of leukemia - Typical signs and symptoms, anemia, thrombocytopenia, and elevated white blood count with blasts present on smear. peripheral blood findings that indicate bone marrow failure. Anemia and thrombocytopenia Many patients with ALL present with total leukocyte counts of <10,000/μL. In such cases, the leukemic cells often are reported initially to be atypical lymphocytes, and it is only on further evaluation that the cells are found to be part of a malignant clone. analysis of peripheral blood suggest the possibility of leukemia, the bone marrow should be examined promptly to establish the diagnosis. It is important that all studies necessary to confirm a diagnosis and adequately classify the type of leukemia be performed, including bone marrow aspiration and biopsy, flow cytometry, cytogenetics, and molecular studies.

33
ALL is diagnosed by a bone marrow evaluation that demonstrates >25% of the bone marrow cells as a homogeneous population of lymphoblasts. If lymphoblasts are found and the CSF leukocyte count is elevated, overt CNS or meningeal leukemia is present. This finding reflects a worse stage and indicates the need for additional CNS and systemic therapies. The staging lumbar puncture may be performed in conjunction with the first dose of intrathecal chemotherapy. traumatic lumbar puncture is associated with an increased risk of CNS relapse.

35
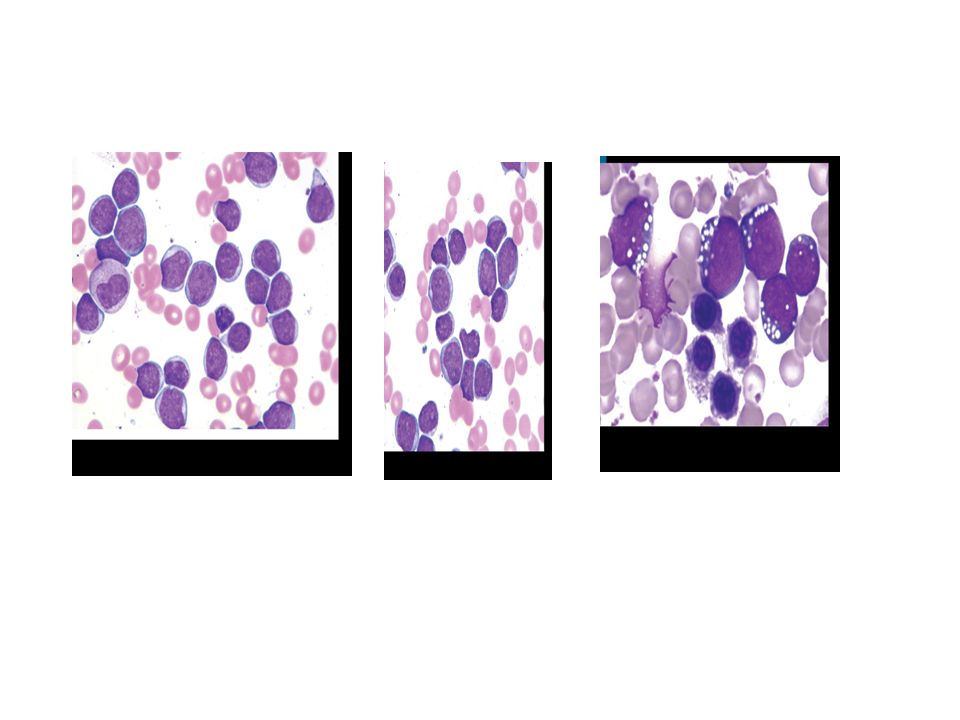
FAB classification based on morphologic criteria (cell size, cytoplasm, nucleoli, basophilia, and vacuolation) L1 ALL - uniform small blasts, scanty cytoplasm, high nuclear cytoplasmic ratio L2 ALL - blast cells are larger, heterogeneous, lower nuclear cytoplasmic ratio, prominent nucleoli L3 ALL – blasts are large with prominent nucleoli, strongly basophilic cytoplasm, and cytoplasmic vacuoles
 L1 ALL - uniform small blasts, scanty cytoplasm, high nuclear cytoplasmic ratio L2 ALL - blast cells are larger, heterogeneous, lower nuclear cytoplasmic ratio, prominent nucleoli L3 ALL – blasts are large with prominent nucleoli, strongly basophilic cytoplasm, and cytoplasmic vacuoles")
36
DIFFERENTIAL DIAGNOSIS The diagnosis of leukemia - Typical signs and symptoms, anemia, thrombocytopenia, and elevated white blood count with blasts present on smear. Elevation of the LDH is often a clue to the diagnosis of ALL. When only pancytopenia is present,-aplastic anemia (congenital or acquired) and myelofibrosis should be considered. Failure of a single cell line, as seen in transient erythroblastopenia of childhood, immune thrombocytopenia, and congenital or acquired neutropenia, is rarely the presenting feature of ALL. A high index of suspicion is required to differentiate ALL from infectious mononucleosis in patients with acute onset of fever and lymphadenopathy and from juvenile idiopathic arthritis in patients with fever, bone pain but often no tenderness, and joint swelling. ALL must be differentiated from AML and other malignant diseases that invade the bone marrow and can have clinical and laboratory findings similar to ALL, including neuroblastoma, rhabdomyosarcoma, Ewing sarcoma, and retinoblastoma.
 and myelofibrosis should be considered. Failure of a single cell line, as seen in transient erythroblastopenia of childhood, immune thrombocytopenia, and congenital or acquired neutropenia, is rarely the presenting feature of ALL. A high index of suspicion is required to differentiate ALL from infectious mononucleosis in patients with acute onset of fever and lymphadenopathy and from juvenile idiopathic arthritis in patients with fever, bone pain but often no tenderness, and joint swelling. ALL must be differentiated from AML and other malignant diseases that invade the bone marrow and can have clinical and laboratory findings similar to ALL, including neuroblastoma, rhabdomyosarcoma, Ewing sarcoma, and retinoblastoma..")
37
Treatment of ALL Risk-directed therapy has become the standard of current ALL treatment and takes into account age at diagnosis, initial white blood cell count, immunophenotypic and cytogenetic characteristics of blast populations, rapidity of early treatment response (i.e., how quickly the leukemic cells can be cleared from the marrow or peripheral blood), The treatment of ALL is subdivided into remission, induction, consolidation with CNS prophylaxis and maintenance phase.
, The treatment of ALL is subdivided into remission, induction, consolidation with CNS prophylaxis and maintenance phase.")
38
Risk stratification of ALL

39
Induction of Remission is designed to eradicate the leukemic cells from the bone marrow. remission, as defined by <5% blasts in the marrow and a return of neutrophil and platelet counts to near-normal levels after 4-5 wk of treatment. Regression of visceromegaly can be observed within the first 2 weeks. Rate of first remission in ALL: More than 90%. For prophylaxis of CNS leukemic disease intrathecal application of methotrexate before, during, and after remission has to be performed. The addition of preventive irradiation is probably necessary in children at high-risk of ALL as determined in most studies. Drugs commonly used in Induction phase: Prednisolone, Vincristine, Daunorubicin, L-Asparginase and Methotrexate.

40
Consolidation Treatment Without continuation of treatment leukemia will reappear within weeks. When remission with normal hematopoiesis is achieved further intensive chemotherapy is necessary to reach a complete eradication of leukemic cells. consolidation, focuses on intensive CNS therapy in combination with continued intensive systemic therapy in an effort to prevent later CNS relapses. CNS relapse is thereby reduced to <5%. Patients with a high risk of CNS relapse may receive irradiation to the brain in later phases of therapy. Includes patients who, at the time of diagnosis, have lymphoblasts in the CSF and either an elevated CSF leukocyte count or physical signs of CNS leukemia, such as cranial nerve palsy. Drugs commonly used in Consolidation phase: Cyclophosphamide, Vincristine, Cytosine Arabinoside and 6 Mercaptopurine.

41
Maintenance Treatment Duration of treatment is 1.5-2.5 years with daily 6-mercaptopurine and once weekly methotrexate, with or without reinduction treatment are commonly used A lifestyle as normal as possible as before the diagnosis has to be followed during maintenance treatment Drugs commonly used in maintenance phase: Prednisolone, Vincristine, Daunorubicin, L-Asparginase, 6 Mercaptopurine and Methotrexate.

42
Treatment of Relapse The major impediment to a successful outcome is relapse of the disease. Relapse occurs in the bone marrow in 15-20% and carries the most serious implications, especially if it occurs during or shortly after completion of therapy. Intensive chemotherapy with agents not previously used in the patient followed by allogeneic stem cell transplantation can result in long-term survival for some patients with bone marrow relapse The incidence of CNS relapse has decreased to <5% since introduction of preventive CNS therapy. The diagnosis of CNS relapse confirmed by demonstrating the presence of leukemic cells in the CSF. The treatment includes intrathecal medication and cranial or craniospinal irradiation. Testicular relapse occurs in less than 2% of boys with ALL, usually after completion of therapy. Such relapse occurs as painless swelling of 1 or both testes. The diagnosis is confirmed by biopsy of the affected testis. Treatment includes systemic chemotherapy and possibly local irradiation.

43
SUPPORTIVE CARE Close attention to the medical supportive care Patients with high white blood counts are prone to tumor lysis syndrome The kidney failure associated with very high levels of serum uric acid can be prevented or treated with allopurinol or urate oxidase. Chemotherapy often produces severe myelosuppression, which can require erythrocyte and platelet transfusion and which always requires a high index of suspicion and aggressive empiric antimicrobial therapy for sepsis in febrile children with neutropenia. Patients must receive prophylactic treatment for Pneumocystis jiroveci pneumonia during chemotherapy and for several months after completing treatment.

44
The successful therapy of ALL is a direct result of intensive and often toxic treatment, can incur substantial academic, developmental, and psychosocial costs for children with ALL and considerable financial costs and stress for their families. Both long-term and acute toxicity effects can occur. cancer care professionals with training and experience in addressing the myriad of problems that can arise is essential to minimize the complications and achieve an optimal outcome.

45
THANK YOU

Similar presentations

1 CHILDHOOD LEUKAEMIA. TA OGUNLESI (FWACP)2 LEUKAEMIA Heterogenous group of malignant disorders Characterised by uncontrolled clonal.>")



 CHEMOTHERAPY Adult Medical-Surgical Nursing.>")







>")


>")
 Nicola Davis.>")

