Download presentation
Presentation is loading. Please wait.

1
WELCOME Applying Wellbeing Data 23 rd November 2011

2
Applying Wellbeing data: Knowsley’s approach Richard Holford Public Health Development Manager

3
Joint Strategic Needs Assessment (JSNA) Wellbeing identified as one of 34 high level needs. Dedicated technical framework / raised profile Identified gaps in knowledge, understanding and provision Clear recommendations for commissioners

4
Joint Strategic Asset Assessment (JSAA) Early stages but have been looking at ways wellbeing can be included in this. Major limitation / issue – not robust to draw down on a locality level.

5
The contribution of wellbeing to life expectancy: Narrowing the gap in inequalities

6
6

7
7

8
8

10
What we know it isn’t Mental well being (WEMWBS) Rates of relative poverty More likely to smoke More likely to be active More likely to be unemployed or in a household with head unemployed Less likely to join sports, religious of education clubs
 Rates of relative poverty More likely to smoke More likely to be active More likely to be unemployed or in a household with head unemployed Less likely to join sports, religious of education clubs")
11
What we know it could be Less likely to be a harmful drinker Highest likelihood of feeling you belong in your local area Second highest satisfaction with local area as a place to live High assessment of being safe in home at night Highest assessment of being safe outdoors in the day (low; safe outdoors at night) Highest likelihood of talking regularly to neighbours High likelihood of being able to find help in a crisis or if ill
 Highest likelihood of talking regularly to neighbours High likelihood of being able to find help in a crisis or if ill")
12
Good guesses Higher level of community cohesion (families, neighbourhoods) Higher level of access to services Improvements in primary care over the period (from low start) Large numbers engaged in prevention services Integration of health and social care
 Higher level of access to services Improvements in primary care over the period (from low start) Large numbers engaged in prevention services Integration of health and social care")
13
What next? Social networks – building community capacity and social growth Protect integration Mass participation in prevention – community led Access to services – QIPP Research causes - proposal

14
Applying wellbeing data in Sefton Pat Nicholl Deputy Head of Health Improvement

15
Sefton Wellbeing Survey 500 face-to-face interviews April–June 2009 Computer Assisted Personal Interviewing Validated scale – WEMWBS + 44 other questions

16
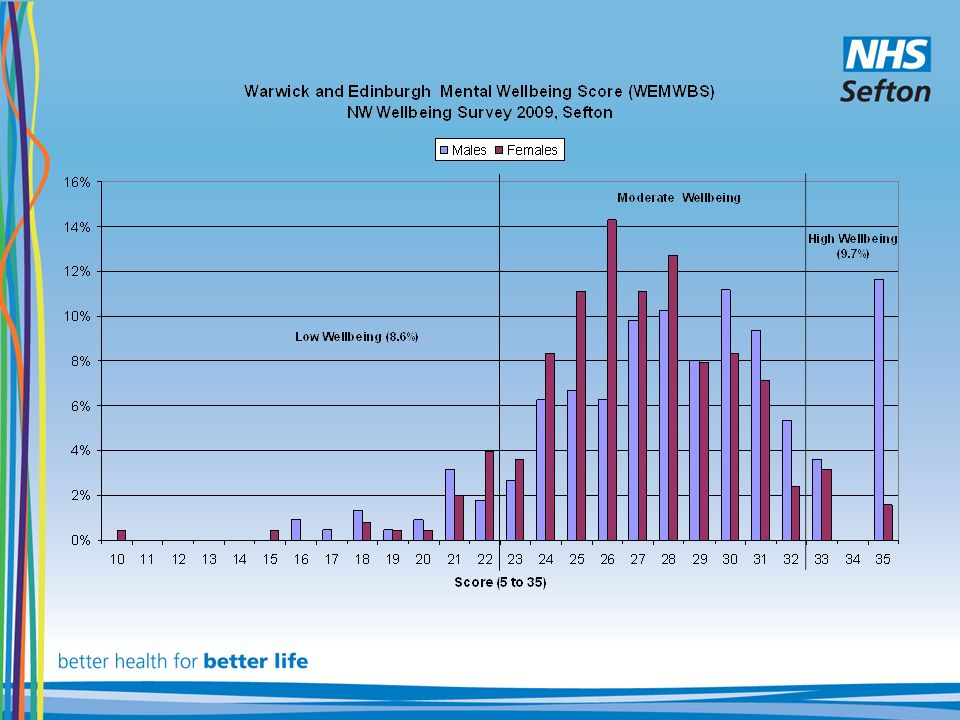
Warwick and Edinburgh Mental Wellbeing Score (WEMWBS) Sefton mean = 27.6 NW mean score = 27.7
 Sefton mean = 27.6 NW mean score = 27.7")
18
Mental Wellbeing distribution More people in Sefton had moderate wellbeing than rest of NW Gender – in Sefton men were significantly more likely to have high mental wellbeing Age – proportion of high mental wellbeing decreased as age increased Deprivation – mental wellbeing reduces as deprivation increases. Ethnicity – lower amongst white than non-white within Regional dataset, not significant in Sefton 8.4%82%9.7%

19
Health Behaviours Physical activity 74% not meeting target. Those with high mental wellbeing were 9 times more likely to meet target Smoking 22% said they currently smoke and 23% were ex-smokers. Those with high mental wellbeing significantly more likely to be ex- smokers. Men were more likely to smoke than women and those aged 25-39 yrs Alcohol No significant difference in relation to wellbeing. 6% were hazardous and 3% harmful drinkers. This data is out of line with other public health data on alcohol and reflects the common issue of self- reporting on this topic

20
Linking public health intelligence Lifestyle Expectancy females in deprived quintiles dipped 2008 & static 2009-10 Liverpool Heart & Chest NHS Trust social marketing programme CVD research by Claro on women’s attitudes

21
Comparing data sources WEMWBS scores (short 7 question) LowModerateHigh Lifestyle Survey 2010 29.567.33.2 Citizens Panel 2010 29.963.86.3 Citizens Panel 2007 28.167.44.5 NW Survey – Sefton 8.681.79.7 NW Well Being Survey 16.862.820.4
 LowModerateHigh Lifestyle Survey Citizens Panel Citizens Panel NW Survey – Sefton NW Well Being Survey")
22
Look After Yourself Target population- women 40-60 in Bootle Engagement & consultation-wellbeing insight Proposal: programme based on 5 ways Engage existing community groups Improve wellbeing scores, CVD risk, awareness and prevention

23
6 community events targeting 300 women Health checks Holistic therapies Five Ways & wellbeing advice

24
Health Check Results 157 health checks 38% were referred to GP or other lifestyle agency 28% had increased CVD risk 48% had raised blood glucose 66% were overweight or obese 32% had a medium or high alcohol risk 29% were smokers.

25
Five Ways Pledges Connect- 80% pledged to connect & improve relationships Be Active –walking most popular pledge Take Notice- appreciate nature Keep Learning- cookery course Give- most popular –’me time Over 50% achieved connect 50% achieved the walking pledge Over 50% achieved take notice and 30% enjoyed time to themselves 20% had signed up to a course in September 2011 66% had given to others and 20% made donations to charity

26
Mental Wellbeing & Health Behaviours Follow-up wemweb & lifestyle survey Wemweb before 24.7After 25.2 Shift from 3.5 to 6.1% with higher wellbeing 30% noticed improvement in mental wellbeing Diet & physical activity of over 66% improved 20% improved smoking habits Alcohol unchanged

27
Next steps Sefton Sanctuary Phase 2 Feedback to participants Creativity & Five Ways Mid-life wellness programme

28
Mid-life health behaviours Eastern Southport Crosby, Thornton, Lydiate Bootle, Seaforth, Litherland All 40-59s Current smokers18.0%8.2%30.5%16.6% Self Assessed Health – Bad or Very Bad5.7%9.3%10.9%9.2% Mental well being – below average33.4%37.9%43.1%35.8% Alcohol – consuming more than recommended weekly allowance 17.0%27.1%30.2%23.5% Alcohol – binge drinking28.0%37.7%42.2%37.7% BMI – overweight35.4%38.3%34.5%38.2% BMI – obese19.2%19.8%28.7%24.1% Physical Activity – meeting CMO 5*3065.3%61.2%64.8%65.6% 5 a day62.0%62.8%43.5%56.4%

29
Applying Wellbeing Data CHAMPS 23 rd November 2011 Tom Hennell Senior Public Health Analyst Department of Health North West Thomas.hennell@dh.gsi.gov.uk 0776 803 0463 0161 625 7452

30
ONS Programme: Measuring National Wellbeing Discussion paper on domains and measures – 31 st October 2011. –Response to national debate and research –Consultation until 23 rd January 2012. Sets out domains (aspects of wellbeing) Proposes headline measures of national wellbeing.
 Proposes headline measures of national wellbeing..")
31
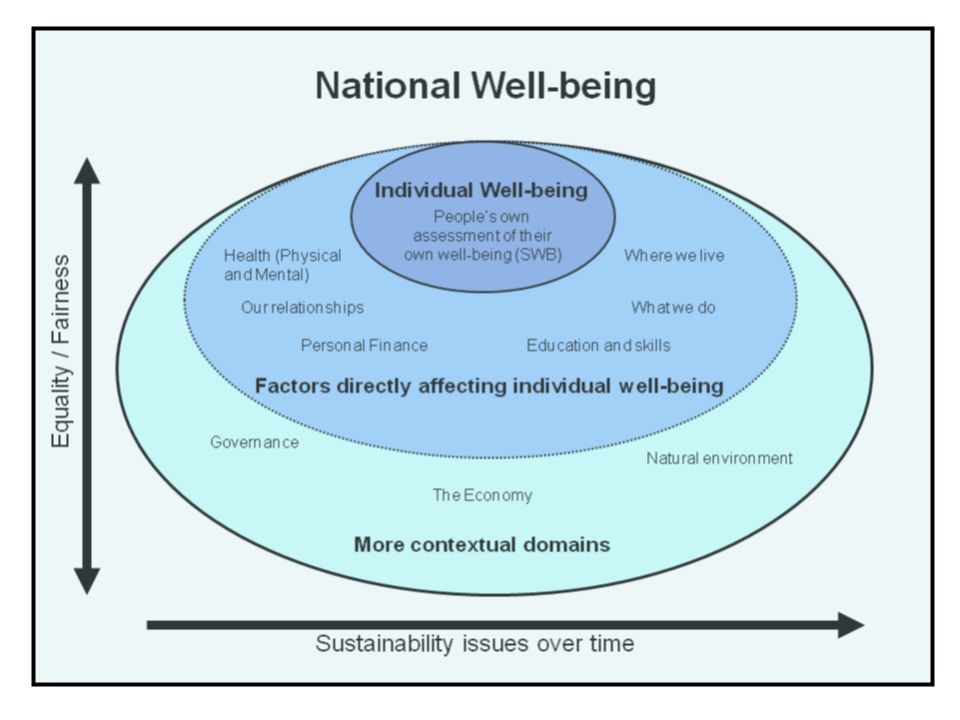
National Wellbeing Framework Surveyed self-assessed individual wellbeing central to understanding national wellbeing. Self-assessed wellbeing needs to be understood in terms of a series of individual and reciprocal factors that directly affect it: –Health, relationships, finance, education, work, household This complex of individual and reciprocal factors is to be understood as relating to social factors within contextual domains; –Equality, Fairness and Sustainability (Attempts to satisfy both those who seek a psychometric wellbeing measure, and those who regard fairness and sustainability and as irreducible wellbeing determinants)
.")
33
Proposed Domains Individual self assessed wellbeing –Life satisfaction, sense of purpose, positive and negative emotions Factors directly affecting individual wellbeing –Our relationships (family, friends and community) –Health (subjective and objective measures) –What we do (work and leisure) –Where we live (housing and neighbourhood) –Personal finance (income and wealth, both absolute and distribution) –Education and Skills (lifelong stock of human capital) More Contextual Domains –Governance (democracy and trust) –The economy (economic output and stock) –The natural environment (climate change and sustainability)
 –Health (subjective and objective measures) –What we do (work and leisure) –Where we live (housing and neighbourhood) –Personal finance (income and wealth, both absolute and distribution) –Education and Skills (lifelong stock of human capital) More Contextual Domains –Governance (democracy and trust) –The economy (economic output and stock) –The natural environment (climate change and sustainability)")
34
Four experimental questions (asked in ONS Opinions Survey 2011) 'Overall, how satisfied are you with your life nowadays? Overall, how happy did you feel yesterday? Overall, how anxious did you feel yesterday? Overall, to what extent do you feel the things you do in your life are worthwhile?'

35
North West Public Health Observatory Centre for Public Health Liverpool John Moores University Liverpool L3 2ET Latest segmentation and insight analysis Clare Perkins and Ian Jarman Acknowledgements: Helen Carlin, Simon Chambers, Lynn Deacon and Jude Stansfield

36
North West Public Health Observatory Centre for Public Health Liverpool John Moores University Liverpool L3 2ET Content Introduction Survey and further analyses - Profiles of wellbeing, what influences wellbeing, employment and resilience, and focus on ethnicity Profiles of wellbeing Influences on wellbeing Employment and resilience Themes

37
North West Public Health Observatory Centre for Public Health Liverpool John Moores University Liverpool L3 2ET Introduction A successful society is one in which people have high levels of wellbeing which is sustained over time. Therefore maintaining and improving wellbeing in the future is important. 2 Analysis undertaken of the wellbeing survey - segmentation based on persons responses - generate insight into the influences on wellbeing 2 New Economics Foundation (2011). Measuring our Progress. The Power of Wellbeing. London: NEF.
. Measuring our Progress. The Power of Wellbeing. London: NEF..")
38
North West Public Health Observatory Centre for Public Health Liverpool John Moores University Liverpool L3 2ET North West wellbeing survey Sample 18,500 residents random selection of LSOA’s within PCT boundary, random selection of households within LSOA, person over 16 in household by next birthday. minimum of 500 per PCT, 18 PCTs bought at least one sample of at least 500 Face-to-face interviews: March–June 2009

39
North West Public Health Observatory Centre for Public Health Liverpool John Moores University Liverpool L3 2ET Developed to measure positive mental health The survey users a shorter seven question version Validated scale – WEMWBS (7 item) I’ve been able to make up my own mind about things I’ve been feeling close to other people I’ve been thinking clearly I’ve been dealing with problems well I’ve been feeling relaxed I’ve been feeling useful I’ve been feeling optimistic about the future Warwick-Edinburgh Mental Wellbeing Scale (WEMWBS)
 I’ve been able to make up my own mind about things I’ve been feeling close to other people I’ve been thinking clearly I’ve been dealing with problems well I’ve been feeling relaxed I’ve been feeling useful I’ve been feeling optimistic about the future Warwick-Edinburgh Mental Wellbeing Scale (WEMWBS)")
40
North West Public Health Observatory Centre for Public Health Liverpool John Moores University Liverpool L3 2ET

41
North West Public Health Observatory Centre for Public Health Liverpool John Moores University Liverpool L3 2ET Segmentation analysis “The aim of any segmentation should be to define a small number of groups so that: all members of a particular group are as similar to each other as possible, and they are as different from the other groups as possible”. 1 1 Association of Public Health Observatories (2009). Technical Briefing 5 Geodemographic Segmentation [Online]. Available at: www.apho.org.uk/resource/item.aspx?RID=67914
. Technical Briefing 5 Geodemographic Segmentation [Online]. Available at: RID=")
42
North West Public Health Observatory Centre for Public Health Liverpool John Moores University Liverpool L3 2ET Cluster and segmentation analysis

43
North West Public Health Observatory Centre for Public Health Liverpool John Moores University Liverpool L3 2ET Working Age, Struggling

44
North West Public Health Observatory Centre for Public Health Liverpool John Moores University Liverpool L3 2ET Working Age, Comfortable

45
North West Public Health Observatory Centre for Public Health Liverpool John Moores University Liverpool L3 2ET Multiple Challenges

46
North West Public Health Observatory Centre for Public Health Liverpool John Moores University Liverpool L3 2ET Retired, Thriving

47
North West Public Health Observatory Centre for Public Health Liverpool John Moores University Liverpool L3 2ET Segment observations Clear differences between groups in terms of - Age - their perceived financial situation - Health - Wellbeing - level of deprivation in which they live

48
Health behaviours Those having the lowest levels of wellbeing are more likely to drink at harmful levels Groups with higher wellbeing tend to have more people who demonstrate an ability to change their health behaviour, such as giving up smoking Retired, Coping and Retired, Thriving both have older age profiles, yet the health of those in Retired, Coping is far worse

49
Segmentation insights a starting point for understanding differences between groups of people highlights groups of factors that may be indicative of a high risk of poor wellbeing and may assist in targeting interventions Changes in factors that influence wellbeing suggest the transitory nature of people between groups

51
Influences on wellbeing State-of-the-art statistical techniques to investigate relationships between all questions in the survey Produces a ‘mind map’ – visualising all the inter-relationships between survey questions Aids understanding to what factors influence respondents’ wellbeing scores

52
Influences: ‘mind map’

53
First level influence on wellbeing Explanation

54
Influence of money on wellbeing

55
Money Nearly half the people with low mental wellbeing had been worried about money almost all the time or quite often over the last few weeks – 2.4 times the proportion of those with high mental wellbeing. Adults with high level of mental wellbeing were 1.5 times more likely to be able to ask for help from others than adults with a low level of mental wellbeing (86.2% compared with 55.9%).
..")
56
Influence of sedentary time

57
Sedentary time Enough time to do enjoyable things. related to whether people have responsibility for caring for somebody. – Care! due to the small number of carers in the sample. Care needs to be taken in interpreting sedentary activity – related to age – and age is also related to household economic type, having time to do enjoyable things and caring for someone

58
Influence of life satisfaction

59
Life satisfaction Health: strong influence on life satisfaction – 79.6% satisfied with life have very good or good health gay/lesbian/bisexual tend to score lower – numbers are small, treat result with caution Those satisfied with life, more likely to feel satisfied with their local area Those living comfortably or coping on present income: more likely to be satisfied with life

60
Employment and wellbeing, health and health behaviours Health question – less than good health (EQ5D)% of employed% unemployed How good is your health in general? Fair, bad or very bad 14.631.1 Mobility: some problems walking about or confined to bed* 5.612.6 Self care: problems with, or unable to, wash and dress self* 0.81.8 Some problems with, or unable to, perform usual activities* 5.512.5 Moderate or extreme pain or discomfort* 16.723.3 Moderate or extreme anxiety / depression* 10.620.4 Health behaviours% of employed % of unemployed Hazardous drinker 13.612.4 Harmful drinker 2.75.9 Current smoker 27.455.5 Ex-smoker 20.610.3 Meet physical activity target 35.032.3 Cannabis use - ever used 12.014.6 Cannabis use last 30 days 2.110.8 Differences in health behaviours of the employed and unemployed North West, 2009 Differences in perceived health between employed and unemployed: less than good health North West, 2009.

61
Wellbeing components (felt often or all the time)% of employed% of unemployed I've been feeling optimistic about the future 58.546.1 I've been feeling useful 73.754.3 I've been feeling relaxed 64.455.2 I've been dealing with problems well 75.664.1 I've been thinking clearly 80.569.8 I've been feeling close to other people 78.364.5 I've been able to make up my own mind on things 85.376.7 Employment and wellbeing - wellbeing Proportions of employed and unemployed people who responded positively to the wellbeing questions, North West, 2009
% of employed% of unemployed I ve been feeling optimistic about the future I ve been feeling useful I ve been feeling relaxed I ve been dealing with problems well I ve been thinking clearly I ve been feeling close to other people I ve been able to make up my own mind on things Employment and wellbeing - wellbeing Proportions of employed and unemployed people who responded positively to the wellbeing questions, North West, 2009")
62
Wellbeing of the employed, by deprivation (IMD 2007) North West 2009 Wellbeing, employment and area deprivation
 North West 2009 Wellbeing, employment and area deprivation")
63
Wellbeing, unemployment and area deprivation Unemployed by level of wellbeing and deprivation (IMD 2007) North West, 2009
 North West, 2009")
64
Well-being and redundancy Wellbeing by change in employment status in last 12 months, North West, 2009.

65
Household employment status Individual employment status Mean wellbeing score Sample size Employed 28.337,871 Employedunemployed 28.032,011 Unemployedunemployed 26.011,155 EmployedRedundancy-employed 28.49179 EmployedRedundancy-unemployed 28.04146 UnemployedRedundancy-unemployed 26.58145 Wellbeing, redundancy and household employment status

66
Redundancy and ‘social connectedness’ Percentage of people with below average wellbeing by redundancy status and social contact North West, 2009

67
Employment Adults with higher mental wellbeing significantly more likely to be in employment Redundancy has a negative impact on wellbeing Economic status of households is important in determining wellbeing Significant proportion of those in employment have health and wellbeing issues Important implications for both unemployment and employment policy

68
Conclusions Many factors influence wellbeing Many inter-connections between factors Interventions and policies should therefore consider the wide range of influences Developing holistic approaches may be prove more successful The analysis supports the development of integrated wellness services and multi-sector health and wellbeing strategies.

Similar presentations