Download presentation
Presentation is loading. Please wait.

1
Journal Club 埼玉医科大学 総合医療センター 内分泌・糖尿病内科 Department of Endocrinology and Diabetes, Saitama Medical Center, Saitama Medical University 松田 昌文 Matsuda, Masafumi 2015 年 3 月 26 日 8:30-8:55 8階 医局 Merovci A, Mari A, Solis C, Xiong J, Daniele G, Chavez A, Tripathy D, Urban McCarthy S, Abdul-Ghani M, DeFronzo RA. Dapagliflozin Lowers Plasma Glucose Concentration and Improves Beta Cell Function. J Clin Endocrinol Metab. 2015 Feb 24:jc20143472.

2
Pioglitazon と Alogliptin の併用効果 European Journal of Endocrinology 170: 565–574, 2014 PBOALOALO/PIO n 242522 Sex (% men) 836068 Age (years) 59.1±6.258.7±6.559.1±6.9 Weight (kg) 99 (93-111)99 (85-102)93 (86-103) BMI (kg/m 2 ) 32.1±4.031.1±4.231.2±3.5 Systolic blood pressure (mmHg) 141±2140±3139±4 Diastolic blood pressure (mmHg) 86±183±2 Diabetes duration (years) 5.5±3.26.4±3.65.0±3.8 A1C (%) 6.6±0.76.8±0.86.6±0.6 Fasting glucose (mmol/L) 8.9±1.69.3±2.88.5±2.0 Anti-hyperglycemic agent (n, %) 23 (96)22 (88)21 (95) Use of metformin (n, %) 13 (57)13 (60)12 (57) Use of sulfonylurea(n, %) 6 (26)6 (28)8 (38) Use of glinidines (n, %) 4 (17)3 (12)1 (5) Discontinued n=0 Completed n=24 Failed screening n=227 Placebo n=24 Alogliptin 25mg n=25 Alogliptin 25mg pioglitazone 30mg n=22 Randomized n=71 Screened n=298 Completed n=25 Discontinued n=0 Completed n=21 Discontinued n=1
 Age (years) 59.1± ± ±6.9 Weight (kg) 99 (93-111)99 (85-102)93 (86-103) BMI (kg/m 2 ) 32.1± ± ±3.5 Systolic blood pressure (mmHg) 141±2140±3139±4 Diastolic blood pressure (mmHg) 86±183±2 Diabetes duration (years) 5.5±3.26.4±3.65.0±3.8 A1C (%) 6.6±0.76.8±0.86.6±0.6 Fasting glucose (mmol/L) 8.9±1.69.3±2.88.5±2.0 Anti-hyperglycemic agent (n, %) 23 (96)22 (88)21 (95) Use of metformin (n, %) 13 (57)13 (60)12 (57) Use of sulfonylurea(n, %) 6 (26)6 (28)8 (38) Use of glinidines (n, %) 4 (17)3 (12)1 (5) Discontinued n=0 Completed n=24 Failed screening n=227 Placebo n=24 Alogliptin 25mg n=25 Alogliptin 25mg pioglitazone 30mg n=22 Randomized n=71 Screened n=298 Completed n=25 Discontinued n=0 Completed n=21 Discontinued n=1")
3
0.4 Pioglitazon と Alogliptin の併用効果 European Journal of Endocrinology 170: 565–574, 2014 Changes in parameters of glucose metabolism after treatment with alogliptin/pioglitazone (ALO/PIO) combination therapy, ALO monotherapy, or placebo (PBO) treatment for 16 weeks. A1C (A) and fasting glucose concentrations (B) were reduced by ALO/PIO combination therapy to a greater extent than ALO monotherapy as compared with PBO. Similarly, postprandial glucose levels were lower following ALO/PIO combination therapy then ALO monotherapy as compared with PBO (C, D and E). **P<0.01; ***P<0.001. ● ■ ▲ Change in A1C (%) 1.0 0.5 0.0 -0.5 -1.5 *** -0.4 -0.9 *** ***** 0.7 -1.2 -1.9 6.7 -12.2 -22.1 1 0 -2 -3 PBOALOALO/PIOPBOALOALO/PIO PBOALOALO/PIO 14 12 10 8 6 4 Glucose (mmol/L) 012345678 *** ** Time (h) Change in FPG (mmol/L) 14 12 10 8 6 4 Glucose (mmol/L) Week 0Week 16 012345678 Time (h) 10 0 -10 -20 -30 Change in AUC glucose (mmol/L×8h) PBO ALO ALO/PIO ● ■ ▲ PBO ALO ALO/PIO AB CDE
 and fasting glucose concentrations (B) were reduced by ALO/PIO combination therapy to a greater extent than ALO monotherapy as compared with PBO. Similarly, postprandial glucose levels were lower following ALO/PIO combination therapy then ALO monotherapy as compared with PBO (C, D and E). **P<0.01; ***P< ● ■ ▲ Change in A1C (%) *** *** ***** PBOALOALO/PIOPBOALOALO/PIO PBOALOALO/PIO Glucose (mmol/L) *** ** Time (h) Change in FPG (mmol/L) Glucose (mmol/L) Week 0Week Time (h) Change in AUC glucose (mmol/L×8h) PBO ALO ALO/PIO ● ■ ▲ PBO ALO ALO/PIO AB CDE.")
4
Pioglitazon と Alogliptin の併用効果 インスリン分泌の改善! European Journal of Endocrinology 170: 565–574, 2014 Week0Week16 Change from baseline Weight (kg) PBO99 (93 to 111)100 (94 to 112)0.6 (-0.2 to 1.3) ALO99 (85 to 102)95 (84 to 102)-0.1 (-1.8 to 1.5) ALO/PIO93 (86 to 103)95 (89 to 101)1.4 (-0.2 to 2.5) 1,000 750 500 250 0 Insulin secretion rates (pmol/min per m 2 ) 581114 1,000 750 500 250 0 581114 Week 0Week 16 ● ■ ▲ PBO ALO ALO/PIO Glucose (mmol/L) Insulin secretion rates (pmol/min per m 2 ) ● ■ ▲ PBO ALO ALO/PIO
 PBO99 (93 to 111)100 (94 to 112)0.6 (-0.2 to 1.3) ALO99 (85 to 102)95 (84 to 102)-0.1 (-1.8 to 1.5) ALO/PIO93 (86 to 103)95 (89 to 101)1.4 (-0.2 to 2.5) 1, Insulin secretion rates (pmol/min per m 2 ) , Week 0Week 16 ● ■ ▲ PBO ALO ALO/PIO Glucose (mmol/L) Insulin secretion rates (pmol/min per m 2 ) ● ■ ▲ PBO ALO ALO/PIO")
5
J Clin Endocrinol Metab. 2015 Feb 24:jc20143472. DOI: http://dx.doi.org/10.1210/jc.2014-3472

6
Background: Beta cell dysfunction is a core defect in T2DM and chronic, sustained hyperglycemia has been implicated in progressive beta cell failure, i.e. glucotoxicity. The aim of the present study was to examine the effect of lowering the plasma glucose concentration with dapagliflozin, a glucosuric agent, on beta cell function in T2DM individuals.

7
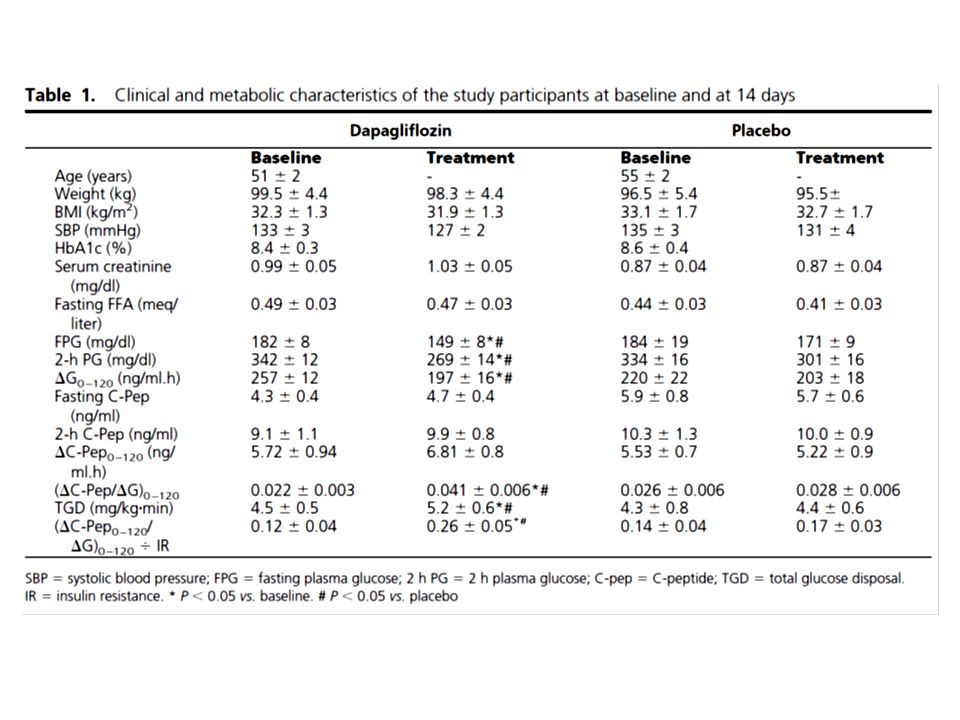
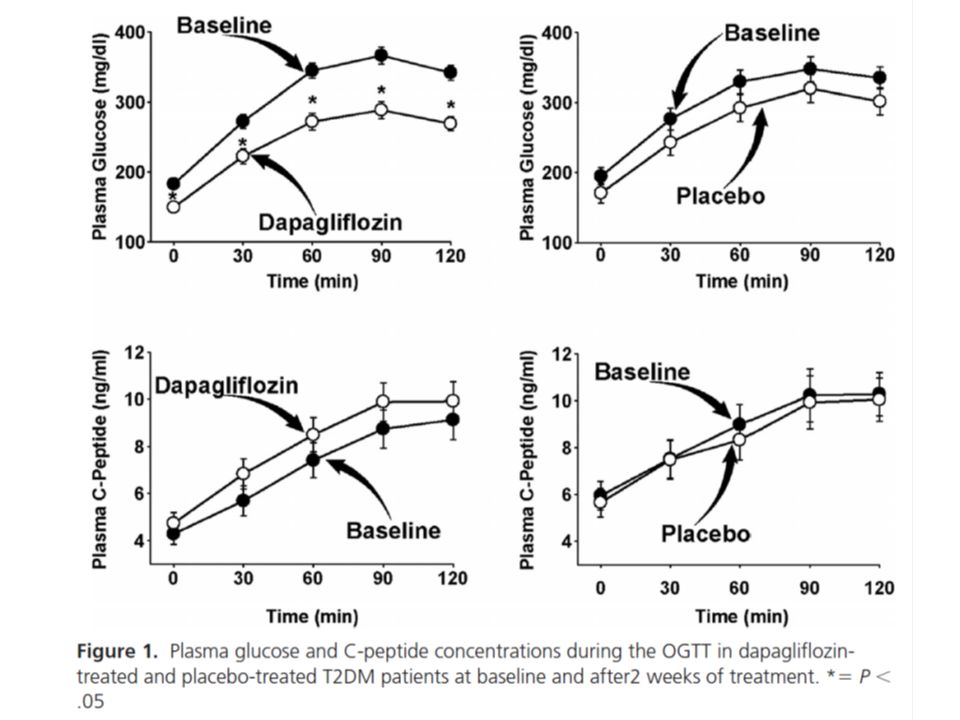
Research Design and Methods: 24 subjects with T2DM received dapagliflozin (n=16) or placebo (n=8) for 2 weeks, and a 75- gram OGTT and insulin clamp were performed before and after treatment. Plasma glucose, insulin, and C-peptide concentrations were measured during the OGTT.

8
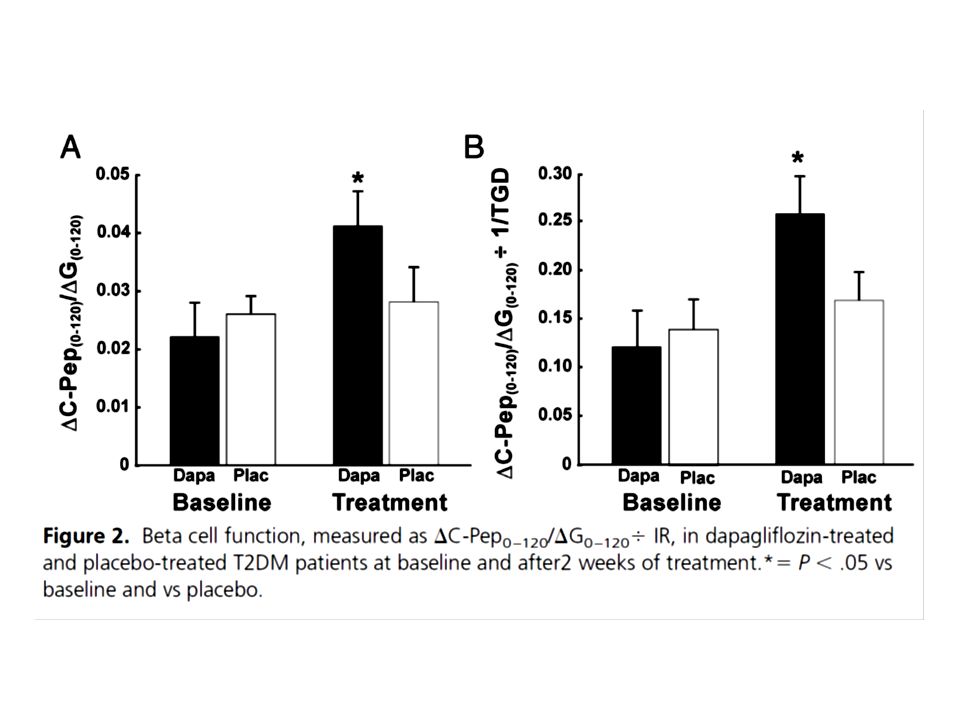
The incremental area under the plasma glucose, insulin, and C- peptide concentration curves was calculated with the trapezoid rule. Insulin secretion was measured as the ratio between the incremental area under the plasma C-peptide concentration to the incremental area under the plasma glucose concentration during the OGTT (Cpep 0–120 /G 0–120 ). Beta cell function was measured as the insulin secretion/insulin resistance or disposition index, where insulin resistance was the inverse of TGD measured with the euglycemic insulin clamp (Cpep 0–120 /G 0–120 ÷ IR). This index is widely used for the assessment of beta cell health (17, 19–22). Beta cell sensitivity to glucose was calculated using the Mari model as previously described (23, 24).
. Beta cell function was measured as the insulin secretion/insulin resistance or disposition index, where insulin resistance was the inverse of TGD measured with the euglycemic insulin clamp (Cpep 0–120 /G 0–120 ÷ IR). This index is widely used for the assessment of beta cell health (17, 19–22). Beta cell sensitivity to glucose was calculated using the Mari model as previously described (23, 24)..")
13
Results: Dapagliflozin significantly lowered both the fasting and 2-hour plasma glucose concentrations and the incremental area under the plasma glucose concentration curve (ΔG0–120) during OGTT by −33±5 mg/dl, −73±9mg/dl and −60±12 mg/dlmin, respectively, compared to −13±9, −33±13 and −18±9 reductions in placebo-treated subjects (both p<0.01). The incremental area under the plasma C-peptide concentration curve tended to increase in dapagliflozin-treated subjects, while it did not change in placebo-treated subjects. Thus, ΔC-Pep0– 120/ΔG0–120 increased significantly in dapagliflozin-treated subjects, while it did not change in placebo-treated subjects (0.019±0.005 vs 0.002±0.006, p<0.01). Dapagliflozin significantly improved whole body insulin sensitivity (insulin clamp). Thus, beta cell function, measured as ΔC-Pep0– 120/ΔG0–120 ÷ insulin resistance, increased by 2-fold (p<0.01) in dapagliflozin-treated versus placebo-treated subjects.
. Dapagliflozin significantly improved whole body insulin sensitivity (insulin clamp). Thus, beta cell function, measured as ΔC-Pep0– 120/ΔG0–120 ÷ insulin resistance, increased by 2-fold (p<0.01) in dapagliflozin-treated versus placebo-treated subjects..")
14
Conclusion: Lowering the plasma glucose concentration with dapagliflozin markedly improves beta cell function, providing strong support in man for the glucotoxic effect of hyperglycemia on beta cell function.

15
Message SGLT2 阻害薬で筋肉のインスリン感受性がよく なることが示されている。一方で膵 β 細胞機能が よくなることも明確に示された。 糖毒性解除という概念の上での役割が強調されて いるようだが、実際には膵 β 細胞機能維持でこそ この薬剤の真価は発揮できると感じるのだが。

18
Aims/Hypothesis: The insulin secretion/insulin resistance (disposition) index (ΔI/ΔG÷IR) commonly is used as a measure of beta cell function (Δ=change from baseline). This relationship is curvilinear and becomes linear when log transformed. ΔI is determined by two variables: insulin secretory rate (ISR) and metabolic clearance of insulin (MCR I ). We postulated that the characteristic curvilinear relationship would be lost if Δ plasma C-peptide (instead of Δ plasma insulin) was plotted against insulin sensitivity.
 and metabolic clearance of insulin (MCR I ). We postulated that the characteristic curvilinear relationship would be lost if Δ plasma C-peptide (instead of Δ plasma insulin) was plotted against insulin sensitivity..")
19
Methods: 441 IGT individuals from ACT NOW received an OGTT and were randomized to pioglitazone or placebo for 2.4 years.

25
Results: Pioglitazone reduced IGT conversion to diabetes by 72% (p<0.0001). ΔI/ΔG vs Matsuda Index (MI) of insulin sensitivity showed the characteristic curvilinear relationship. However, when ΔCP/ΔG or ΔISR/ΔG was plotted against MI, the curvilinear relationship was completely lost. This discordance was explained by two distinct physiologic effects that altered plasma insulin response in opposite directions: (i) increased ISR and (ii) augmented MCR I. The net result was a decline in plasma insulin response to hyperglycemia during OGTT. These findings demonstrate a physiologic control mechanism wherein the increase in ISR ensures adequate insulin delivery into portal circulation to suppress HGP while delivering reduced but sufficient amount of insulin to peripheral tissues to maintain the pioglitazone-mediated improvement in insulin sensitivity without excessive hyperinsulinemia.
 of insulin sensitivity showed the characteristic curvilinear relationship. However, when ΔCP/ΔG or ΔISR/ΔG was plotted against MI, the curvilinear relationship was completely lost. This discordance was explained by two distinct physiologic effects that altered plasma insulin response in opposite directions: (i) increased ISR and (ii) augmented MCR I. The net result was a decline in plasma insulin response to hyperglycemia during OGTT. These findings demonstrate a physiologic control mechanism wherein the increase in ISR ensures adequate insulin delivery into portal circulation to suppress HGP while delivering reduced but sufficient amount of insulin to peripheral tissues to maintain the pioglitazone-mediated improvement in insulin sensitivity without excessive hyperinsulinemia..")
26
Conclusions: These results demonstrate the validity of disposition index when relating plasma insulin response to insulin sensitivity, but underscore the pitfall of this index when drawing conclusions about beta cell function, since insulin secretion declined despite an increase in plasma insulin response.

27
Message Disposition index についてはともかく、 Pioglitazone による血糖改善時に ISR とインス リン濃度が乖離しているのが元々の現象のようで ある。 ともかく、 pioglitazone による血糖改善がイン スリン分泌改善ということをはっきり支持するた めに必要な議論と思われる。

Similar presentations















行列式の定義には、数学的な概念がいろいろ必要である。まずそれらを順に見ていく。>")






を体験したことにより興味を惹かれ るきっかけとなった。主な目的は、これ.>")





