Download presentation
Presentation is loading. Please wait.

1
DIFFICULT SMALL BOWEL CROHN’S DISEASE John Northover St Mark’s Hospital, London

3
LOOK BEFORE YOU LEAP

5
Causes of intestinal failure St Mark’s & Hope, 1999-2002

6
Difficult SB Crohn’s Duodenal disease Duodenal disease Multiple strictures Multiple strictures Enterocutaneous fistula Enterocutaneous fistula

7
Duodenal Crohn’s

8
A few facts Rare - <5% Rare - <5% Differential diagnosis Differential diagnosis Rarely sole site Rarely sole site Often overshadowed Often overshadowed

9
Duodenum plus.... D3 stricture D3 stricture Advanced ileal disease Advanced ileal disease

10
Clinical scenarios ‘Peptic ulcer-like’ ‘Peptic ulcer-like’ Obstruction Obstruction Fistula Fistula

11
Patterns of disease *

12
Symptoms ‘Peptic ulcer’ pain 70% ‘Peptic ulcer’ pain 70% Vomiting 50% Vomiting 50% Weight loss 26% Weight loss 26% Diarrhoea 22% Diarrhoea 22% Bleeding 7% Bleeding 7%

13
Investigation Barium studies Barium studies Scanning Scanning Endoscopy Endoscopy

14
Conventional Ba meal Anatomical clarity Anatomical clarity Endoscopy needed Endoscopy needed

15
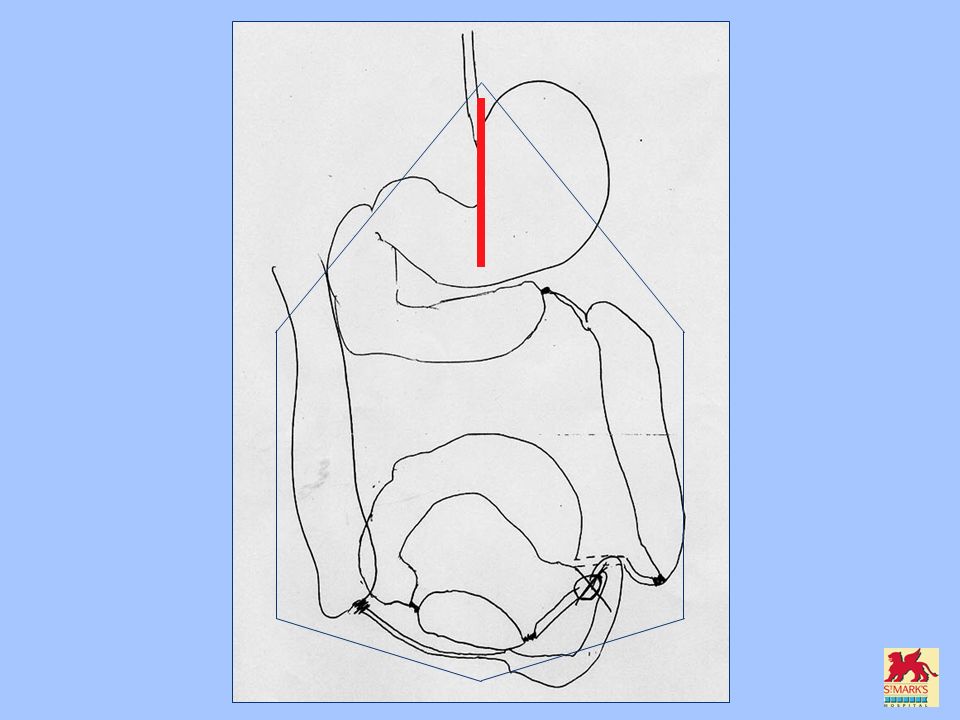
BaM in D3 obstruction Poor view Poor view No distal information No distal information

16
CT in D4 obstruction

17
Endoscopy Differential diagnosis Differential diagnosis Dilatation Dilatation

18
Treating obstruction Balloon dilatation Balloon dilatation Bypass Bypass Strictureplasty Strictureplasty

19
Balloon dilatation May avoid surgery May avoid surgery Few data Few data Distal disease Distal disease

20
Bypass Check for distal disease Check for distal disease ? need for vagotomy ? need for vagotomy –“4/6 without re-operation” (Cleveland, ‘83) –“Most re-do surgery after Vx; risk of diarrhoea” (Lahey, ‘89) –“Remains controversial” (B’ham, ‘99)
 – Most re-do surgery after Vx; risk of diarrhoea (Lahey, ‘89) – Remains controversial (B’ham, ‘99).")
21
Strictureplasty 13 patients (10 primary) 13 patients (10 primary) 2/10 leaked 2/10 leaked 6 re-strictured surgery 6 re-strictured surgery Overall 9/13 re-operated Overall 9/13 re-operated Birmingham, 1999
 13 patients (10 primary) 2/10 leaked 2/10 leaked 6 re-strictured surgery 6 re-strictured surgery Overall 9/13 re-operated Overall 9/13 re-operated Birmingham, 1999")
22
‘Plasty v Bypass Historical and parallel comparison Historical and parallel comparison Bypass 21; strictureplasty 13 Bypass 21; strictureplasty 13 Same: Same: – Complications (2/21; 2/13) – Recurrence Re-op. (1/21; 1/13) Cleveland Clinic, 1999
 Cleveland Clinic,")
23
Fistulating duodenal Crohn’s Usually secondary Usually secondary To colon or terminal SB To colon or terminal SB Duodenocutaneous rare Duodenocutaneous rare Most OK for oversew Most OK for oversew

24
D2-transverse colic fistula Normal duodenum Normal duodenum Penetrating ulcers Penetrating ulcers Simple closure after colectomy Simple closure after colectomy

26
Multiple strictures

27
Failure to thrive Failure to thrive Obstruction Obstruction

28
Multiple strictures

29
What trouble are they? What trouble are they? Other modalities? Other modalities? Previous surgery? Previous surgery? Is there a ‘dominant’ stricture? Is there a ‘dominant’ stricture? AND ONLY THEN... AND ONLY THEN...

30
Multiple strictures Might surgery help? Might surgery help? If so, what surgery? If so, what surgery? –(Bypass) –Resection –Strictureplasty
 –Resection –Strictureplasty.")
31
Multiple strictures Pros and cons of strictureplasty Bowel conservation Bowel conservation Safety Safety Relapse rate Relapse rate

32
Multiple strictures Recurrence avoidance Oxford, 1995

33
Multiple strictures Recurrence avoidance 2006 meta analysis Tekkis et al.

34
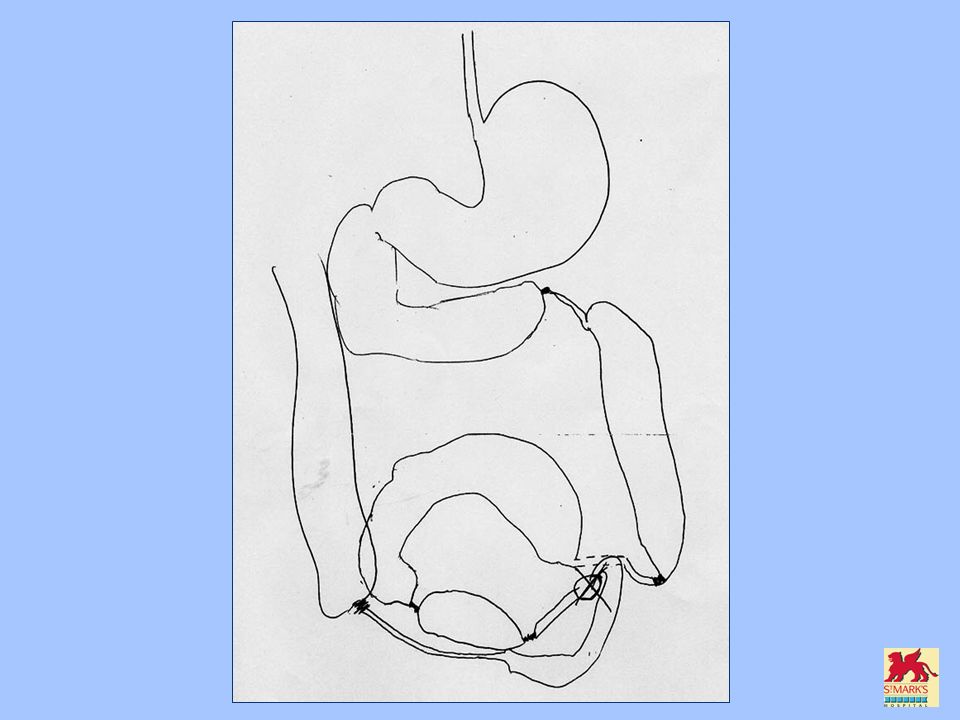
Strictureplasty What’s available?

36
What do they achieve?

37
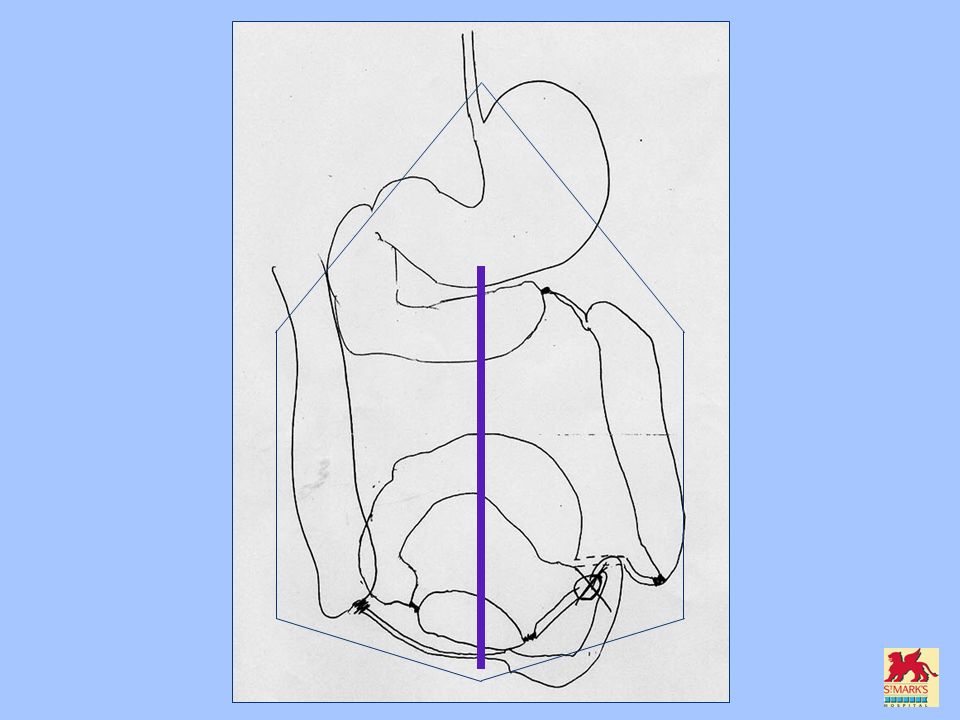
Strictureplasty What’s available?

38
Strictureplasty Beware the occult stricture

39
Strictureplasty Pick ‘n’ Mix...

41
Enterocutaneous fistula

42
Surgery rarely avoided

43
Avoiding re-operation

44
NO UNEXPECTED EXTRA PROCEDURES

45
Avoiding DISASTER DON’T GO IN TOO EARLY

46
Avoiding DISASTER DON’T GO IN TOO EARLY

47
Avoiding DISASTER DON’T GO IN TOO EARLY WAIT!!

48
Avoiding DISASTER DON’T GO IN TOO EARLY WAIT!! and PREPARE

49
Exclude distal obstruction Exclude septic collections Find the optimal entry site Pre-operative preparation

50
Avoiding re-operation ROADMAP ROADMAP Composite image Composite image Pre-operate in head Pre-operate in head

57
DIFFICULT SMALL BOWEL CROHN’S DISEASE John Northover St Mark’s Hospital, London

Similar presentations