Download presentation
Presentation is loading. Please wait.

1
Prevention and Management of HPV and Risk for Other Sexually Transmitted Infections JEAN M. KELLER, PAC ASSISTANT PROFESSOR JOHNS HOPKINS UNIVERSITY GYNECOLOGY AND OBSTETRICS

2
Learning Objectives Understand the incidence, prevalence and natural history of Human Papilloma infection Discuss current HPV vaccine guidelines Understand the risk and prevention strategies of other Sexually transmitted infections. Discuss how HPV can be prevented and prevented

3
Sexually Transmitted Infection Overview CDC defines STDs as various clinical syndromes/infections caused by pathogens that can be acquired through sexual activity Viral Bacterial Protozoan

4
Prevention of STDs Overview Accurate risk assessment Education and counseling of at risk persons Pre-exposure vaccination Identification of asymptomatic and symptomatic persons Effective diagnosis, treatment, counseling and follow up Evaluation, treatment, and counseling of Sex partners

5
STD/HIV Risk Assessment Primary prevention of STDs Behavioral and biologic risk Routine sexual histories Effective interviewing and prevention counseling STD screening of all STDs STDs are biologic markers of risk for HIV acquisition and transmission Identifies asymptomatic infection

6
STD Prevention Counseling USPSTF recommends high-intensity behavioral counseling for SA adults and adolescents at increased risk for HIV and STDs Client centered STD/HPV Prevention counseling Tailor the discussion of risk reduction to the individual situation. Motivational interviewing Achievable risk reduction goals.

7
Prevention Methods Pre-exposure Vaccines HPV, HAV and HBV Abstinence and Reduction of Number of Sex Partners Male condoms (available in latex and polyurethane) Female condom (polyurethane)- available globally FC2 Female Condom, Reddy condom, Cupid female condom, and Woman’s condom. Although limited data on effectiveness - advantage is female controlled Also been used during receptive anal intercourse (unknown efficacy)
.")
8
Prevention Methods Male circumcision- Reduces risk for HIV and Some STDs in heterosexual men Not effective Topical microbicides and spermicides Diaphragm Non barrier contraception Important to discuss with patient that these methods offer no STI or HIV protection

9
Prevention Methods Retesting after treatment to detect Repeat Infections Gonorrhea, chlamydia and trichomoniasis Repeat tests 3 months to assess for re-infection Syphilis- follow-up with serologic syphilis testing HIV prevention PEP- Post exposure prophylaxis Identification and treatment of persons with HIV-use of ARV to suppress HIV PReP- use of TDF and FTC Guidelines for use available Safe conception with discordant couples

10
HPV Prevalence and Incidence U.S. Estimated that most every sexually active man and women will acquire HPV at some point in their lives. 79 million currently infected with HPV 14.1 million new infections each year (incidence of Chlamydia is 2.9 million) 50% occur in youth and young adults 15-24 years old Women incidence peaks in 20’s, decreasing Studies in men show incidence relatively constant over a wide age range. Cost of treatment in US about $1.7 billion Prevalence date based on NHANES (National Health and Nutrition Examination survey) Females only from self collected swabs and other clinical studies CDC Treatment guidelines web site ACIP HPV vaccine guidelines
 50% occur in youth and young adults years old Women incidence peaks in 20’s, decreasing Studies in men show incidence relatively constant over a wide age range. Cost of treatment in US about $1.7 billion Prevalence date based on NHANES (National Health and Nutrition Examination survey) Females only from self collected swabs and other clinical studies CDC Treatment guidelines web site ACIP HPV vaccine guidelines.")
11
HPV Natural History Most infection occurs w/n a few years of SA Most HPV infection (regardless of type) is transient- median duration of 12 month Prevalence declines with increasing age Peak prevalence 20-24 years Gradual decline to about 40-45, but may increase slowly again Multiple infections 13-14% (more than one HPV type) 52% in immuno-compromised patients HIV positive- increased persistence /recurrence
 is transient- median duration of 12 month Prevalence declines with increasing age Peak prevalence years Gradual decline to about 40-45, but may increase slowly again Multiple infections 13-14% (more than one HPV type) 52% in immuno-compromised patients HIV positive- increased persistence /recurrence")
12
Source: http://dceg.cancer.gov/newsle tter/jul06/Cervical_Cancer_fig 1.jpg

13
HPV Over 300 HPV sub-types (strains) identified 2 major branches: cutaneous or mucosal 40 mucosal or urogenital types Transmissible through sexual contact Infects the ano-genital and other mucosal tissue Most classified as : Low risk or non-oncogenic types Genital warts Benign/low grade cervical cellular changes High risk or oncogenic types (ie. 16 and 18) Associated with cancers of vulva, vagina, anus, penis and oropharynx
 Associated with cancers of vulva, vagina, anus, penis and oropharynx.")
14
Human Papilloma Virus (HPV) and Cervical Cancer 1990’s Epidemiologic studies Molecular technologies Certain types established as a central cause of ICC Using the most sensitive detection assays, 99.7% of ICC found to be HPV (+) - Clifford, et al, Br J Cancer, 2003 - Walboomers, et al, J Pathol, 1999 Source: http://wehonews.com/z/wehonews/archive/ images/hpv.jpg Photo of HPV
 and Cervical Cancer 1990’s Epidemiologic studies Molecular technologies Certain types established as a central cause of ICC Using the most sensitive detection assays, 99.7% of ICC found to be HPV (+) - Clifford, et al, Br J Cancer, Walboomers, et al, J Pathol, 1999 Source: images/hpv.jpg Photo of HPV")
15
HPV Types and Lower Genital Tract Neoplasia- Relative Risk

16
HPV and Cervical Cancer

17
HPV Cancer HR HPV (types 16,18) Anogenital cancers Cervix:66% Vagina:55% Anal:79% Oro-pharyngeal62% HPV 16 linked with oro-pharyngeal cancer Each year 26,000 new cancers are attributable to HPV
 Anogenital cancers Cervix:66% Vagina:55% Anal:79% Oro-pharyngeal62% HPV 16 linked with oro-pharyngeal cancer Each year 26,000 new cancers are attributable to HPV")
18
HPV infection HPV cervical cancer disproportionately higher among minorities than whites including: Hispanics Blacks American Indians Alaskan natives HPV vaginal cancer rates higher in blacks HPV vulva cancer rates higher in whites HPV oropharyngeal increasing frequency males >females in all racial groups except blacks

19
CIN and Invasive Risk Co-factors in the development of Cervical Cancer Epidemiologic Early Sexual Experience # of sexual partners Male partner factors (# sex partners, hx/o STI’s) Smoking Nutritional Carotenoids, vitamin A, retinoids Vitamins C, E, and folate
 Smoking Nutritional Carotenoids, vitamin A, retinoids Vitamins C, E, and folate")
21
System Failures leading to Cervical Cancer Diagnosis Women do not come in for screening Health care providers do not screen women at visits Evaluation of Abnormal screen Not done Patient does not get Appropriate therapy Patient gets Cervical cancer Source: P Pronovost

23
Prevention - HPV Vaccine Three licensed prophylactic vaccines are available Bivalent*, Quadrivalent and 9-valent HPV vaccines Each protects against HPV 16 and 18. Quadrivalent additional protection for 6 and 11 Prevents 90% of genital warts 9-valent- additional protection for HPV 31,33,45,52, and 58)
.")
24
HPV Vaccine 9-valent HPV 9-Valent Vaccine (Gardasil-9) Additional protection against cervical cancer (15%) Protect against vaginal and vulvar cancers Anal cancer in females and men Protects against genital warts
 Additional protection against cervical cancer (15%) Protect against vaginal and vulvar cancers Anal cancer in females and men Protects against genital warts")
25
HPV Vaccine- Treatment vaccines Safety, Efficacy and Immunogenicity of VGX-3100 Randomized treatment vaccine for CIN 2/3 with HPV 16 and HPV 18 167 patients randomized to Vaccine (125) or placebo (42) Primary efficacy endpoint- CIN1 or normal pathology 36 weeks after the first dose Findings Vaccine group 53/107 (49.5%) vs. 11/36 (30.6%) showed regression (p=0.034) VGX-3100 is the first therapeutic vaccine to show efficacy against CIN 2/3
 showed regression (p=0.034) VGX-3100 is the first therapeutic vaccine to show efficacy against CIN 2/3.")
27
Other HPV Vaccine Information ACIP: recommends MSM/Bisexual men be vaccinated through age 26 years. Can continue with the 9-valent HPV vaccine if the series is started with a different HPV vaccine http://www.cdc.gov/vaccines/who/teens/downl oads/9vHPV-guidance.pdf

28
Pap Smears Widespread introduction of Pap smear began in 1949 Mortality from cervical cancer in US decreased from approximately 10/100,000 in 1950 to <3/100,000 in 1994 93% of cervical cancers could be prevented by Screening and HPV vaccination

29
Role of Cervical Cancer Screening (Pap smear) Significant reduction of Cervical ca in U.S. 13,000 new cases each year Cervical ca mortality- 4,400 Counsel patients on the purpose and importance of routine pap smears External warts are not an indication for more frequent pap smears

30
Liquid-based Collection and Thin-Layer Processing Minimal cell loss with immediate fixation Decreased unsatisfactory rate 63% Decreased ASCUS/AGCUS 3.0 - 26.6% SIL detection increased by 52.2 - 65.0% Enhanced sensitivity No loss in specificity Lee. Obstet Gynecol 1997; 90:278 Papillo. Acta Cytol 1998; 42:203 Guidos. Diagn Cytopathol 1999; 20:70

31
Cervical Cancer Screening Cervical cancer screening should begin at age 21 years. Women under 21 should not be tested Women between 21 and 29 HPV testing should not be used for screening in this age group Women between 30 and 65 Cervical pap every 3 years With HPV (co-testing) every 5 years (preferred) Women over 65 years If past regular screening tests normal stop screening (ACOG recommendation) If history of serious dysplasia continue for 20 years after the diagnosis regardless of age.
 every 5 years (preferred) Women over 65 years If past regular screening tests normal stop screening (ACOG recommendation) If history of serious dysplasia continue for 20 years after the diagnosis regardless of age..")
32
Cervical Cancer Screening History of hysterectomy - no screening if negative history of severe dysplasia or cervical cancer. HPV vaccinated Should still follow screening recommendations for her age group APP for smart phone: Pap guide

33
Roles for HPV Testing in Cervical Screening Programs Cervical cancer screening in conjunction with Pap Negative HPV in women >30 can increase time between screening from 3-5 years Triage of abnormal cervical cytology ASCUS Follow up after treatment of Cervical dysplasia (precancerous) Future- Primary screening
 Future- Primary screening")
34
HPV Testing Several FDA approved HPV tests in the US Available for women >30 years undergoing cervical cancer screening Should not be used to Screen men for HPV In women <30 years As a general STI screening test

35
AGCUS or AIS > 35 years must be evaluated with endometrial biopsy < 35 years Endometrial biopsy should be performed if risk factors for endometrial neoplastic lesions Unexplained vaginal bleeding Chronic conditions suggesting anovulation

36
Recommendations for Screening for Other Anogenital HPV-related Disease Careful examination of vulva, vagina, perinal region for possible HPV-related lesions Biopsy atypical-appearing lesions Routinely question about rectal bleeding or pain Anal cytology: consider if resources are available to evaluate (high resolution anoscopy) and treat abnormal findings (Aberg 2009)
 and treat abnormal findings (Aberg 2009)")
37
HPV Transmission HPV is a double stranded DNA virus of the Papilomaviridae family and are obligatory intra- nuclear organisms. Genital types have specific affinity for genital skin and mucosal surfaces. Three possible events at entry into the cell Viral DNA are intranuclear, but extra-chromosomal replicating with the cell establishing latent infection Conversion from latent into productive infection with assembly of complete infective virions; or Integration of the DNA into the host cellular genome seen in HPV infection associated with malignancies

38
HPV Transmission Transmission can occur by auto- and hetero- inoculation from common skin warts Fomites have been found on surfaces but only fully formed virion known to be infectious Most frequent sites are those susceptible to micro trauma during intercourse Introitus peri-anal and intra-anal membranes Increased risk of transmission Hormonal contraception Pregnancy Impaired cell mediated immunity

39
HPV Diagnosis Presumptive Typical warts on skin Detection of lesion by colposcopy Detection of subclinical lesion by application of 5% acetic acid Suggestive Demonstration of typical cytologic changes on pap smear

40
HPV Diagnosis Definitive Identification of characteristic change on biopsy (koilocytosis) Detection of HPV in smear material HPV and Pap co-testing
 Detection of HPV in smear material HPV and Pap co-testing")
41
HPV Spectrum of disease Condyloma acuminata (genital warts) Subclinical disease (cervical cellular abnormalities) Some anogenital squamous cell carcinomas Other types of cancers ( oropharyngeal cancers) Recurrent respiratory papilomatosis Latent/asymptomatic infection No evidence of disease Viral shedding and transmission possible
 Subclinical disease (cervical cellular abnormalities) Some anogenital squamous cell carcinomas Other types of cancers ( oropharyngeal cancers) Recurrent respiratory papilomatosis Latent/asymptomatic infection No evidence of disease Viral shedding and transmission possible")
42
Differential Diagnosis Genital Warts Normal anatomic structures Pearly penile papules Sebaceous Tyson’s glands Micropapillomatosis or vestibular papillae (exaggerated version of physiologic vulvar skin)
")
43
Squamous papillomatosis Squamous Papillomatosis

44
Genital Warts Differential Diagnosis (Acquired conditions) Bowenoid papules Bushke-Lowenstein tumor ( Verrucous Carcinoma ) Lichen planus Lichen nitidus Melanocytic nevi Pseudoverrucous papules Molluscum contagiousum seborrheic keratosis Condyloma lata Crohn’s disease Skin tags VIN
 Bowenoid papules Bushke-Lowenstein tumor ( Verrucous Carcinoma ) Lichen planus Lichen nitidus Melanocytic nevi Pseudoverrucous papules Molluscum contagiousum seborrheic keratosis Condyloma lata Crohn’s disease Skin tags VIN")
45
Lichen simplex chronicus

46
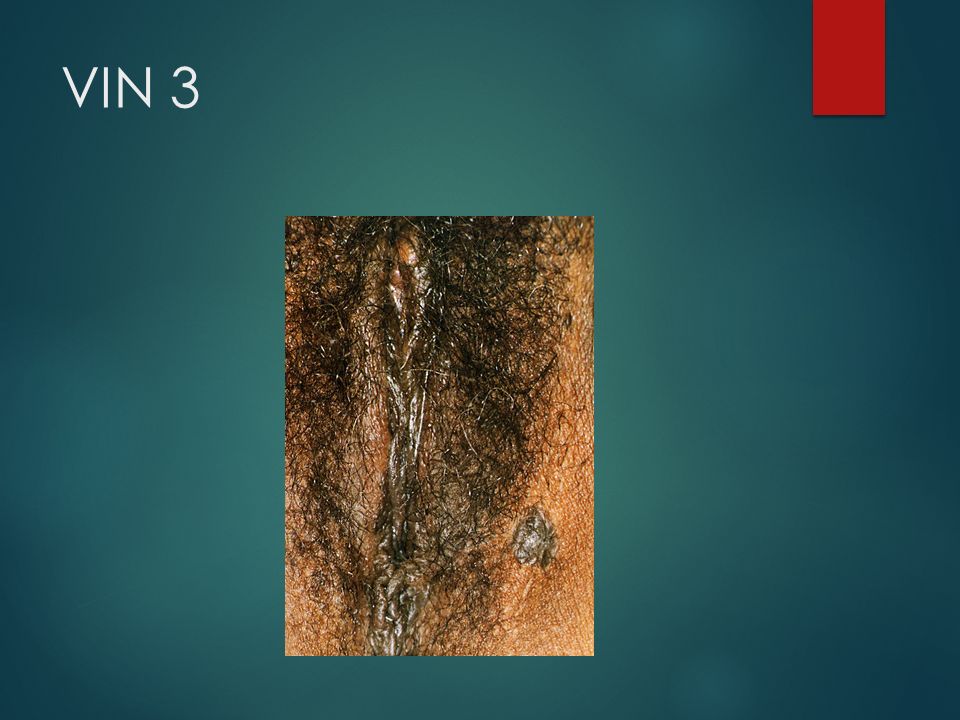
VIN 3

50
Breakdown Indurated mass Left Labial Lesion 2.5 x 7 x 5.7 cm lesion

51
Clinical Manifestations Genital warts Condylomata acuminata Smooth papules Flat papules Keratotic warts (can resemble seborrheic keratosis)
")
52
Condyloma Accuminata (Genital Warts) Incubation period 3weeks to 8 months Usually asymptomatic but occasionally itching, burning, pain, or bleeding Spontaneous regression and recurrence common No increased prevalence HSIL HPV type 6, 11- 10% contain HPV 16
 Incubation period 3weeks to 8 months Usually asymptomatic but occasionally itching, burning, pain, or bleeding Spontaneous regression and recurrence common No increased prevalence HSIL HPV type 6, % contain HPV 16")
53
Condyloma Accuminata Typically raised lesions with a warty granular appearance May be flat or hyper-pigmented* *Most suspicious for VIN Most often multifocal Women located introitus, labia minora, majora and perianal skin Men located distal half of the penis and the urethral meatus

54
HPV – Indications for biopsy anogenital lesions Diagnosis uncertain Lesions do not respond to therapy Diagnosis worsens during therapy Lesion atypical, indurated, pigmented, fixed, bleeding or ulcerated Patient with compromised immunity (more likely to have anogenital dysplasia

55
Condylomata Accuminata

58
HPV Treatment of External Genital Warts Cytotoxic agents and keratolytic agents: .5% podofilox (self treatment liquid nitrogen 50-80% bichloroacetic or trichloroacetic acid Podophylin Cytodestructive techniques CO2 laser vaporization electroexcision/fulguration (LEEP) Cryotherapy Sinecatechin ointment (green tea extract) Self applied TID up to 16 weeks
 Cryotherapy Sinecatechin ointment (green tea extract) Self applied TID up to 16 weeks")
59
HPV Treatment of genital warts Surgical excision Immune-modulating agents Imiquimod (Aldara)- interferon and cytokine inducer 5-Fluorouracil Alpha-interferon- recalcitrant lesions can be used in combination with laser or electro surgery 80% complete or partial response vs. placebo

60
HPV-(subclinical manifistations) Lower Anogenital Tract Neoplasias More common than genital warts Lower anogenital tract neoplasia- AIN, VIN, VAIN, CIN Represents 60% & 90% of all HPV infections of the external anogenital tract and cervix respectively Best seen with 5% acetic acid solution and colposcopic / anoscopic examination
 Lower Anogenital Tract Neoplasias More common than genital warts Lower anogenital tract neoplasia- AIN, VIN, VAIN, CIN Represents 60% & 90% of all HPV infections of the external anogenital tract and cervix respectively Best seen with 5% acetic acid solution and colposcopic / anoscopic examination")
61
AGCUS 17-34% associated intraepithelial or invasive lesions Associated lesions: Cervical adenocarcinoma Endometrial adenocarcinoma Metastatic Ca Risk of HGSIL: Premenopausal 30.4% Postmenopausal 7.4% Kennedy. Gynecol Oncol 1996; 63:14 Korn. JRM 1998; 43:774 Duska. Obstet Gynecol 1998; 91:278

62
HPV Subclinical Manifestations Histologic findings alone have little predicative value of HPV type HPV typing determines whether low vs high risk for progression to invasive disease

63
HPV Subclinical Manifestations Best appreciated with magnification & 5% acetic acid solution (colposcope) Slightly elevated, well demarcated focal lesions with or without mosaic patterns or punctations Commonly seen on labia minora, perianal, vestibular skin & cervical transformation zone
 Slightly elevated, well demarcated focal lesions with or without mosaic patterns or punctations Commonly seen on labia minora, perianal, vestibular skin & cervical transformation zone")
64
Cervical Ectopy

65
CINCIN 1 1

66
CIN 33

67
CIN 22

68
CIN 1 (higherCIN 1 magnification)
")
69
CIN 3- CA in situ (coarse punctation and coarse mosaic)
")
70
Leukoplakia

71
Numerous cysts in an established transformation zone

72
HPV Management of Subclinical Disease Management determined by the location, severity and number of lesions LSIL- Observation, 70% of low grade lesions will regress spontaneously HSIL- 80% progression if untreated Ablative or excisional dependent on the size and location of the lesion Endocervical lesions should be managed with excisional therapy Cervical, vulvar, vaginal ca- refer gyn oncologist

73
HPV Management of Subclinical Disease Cervical, vaginal, and vulvar intraepithelial lesions (CIN, VAIN, VIN respectively) Management usually based on colposcopic directed biopsy results and pap smear Cervical lesions- cure rates related to size and distribution of lesions, not morphologic grade or HPV type
 Management usually based on colposcopic directed biopsy results and pap smear Cervical lesions- cure rates related to size and distribution of lesions, not morphologic grade or HPV type")
74
Treatment of Cervical Dysplasia Excisional procedure recommended (LEEP or cervical conization) Pathologic analysis, including margin status Lesions may involve larger area of cervix
 Pathologic analysis, including margin status Lesions may involve larger area of cervix")
75
HPV Treatment of Cervical Warts Dysplasia must be excluded before treatment is begun Management should be carried out in consultation with an expert

76
HPV Subclinical Management Ablative vs. Excisional Treatment Ablative- 80-90% effective but, may be used inadvertently in early invasive disease Excisional-Best for treatment of CIN, especially high grade endocervical lesions

77
HPV Subclinical Manifestations Advantages of LEEP/LLETZ Low risk for missing invasive disease Diagnosis and therapy in one session Office procedure Low cost of equipment May be used for treatment of condylomata, intraepithelial lesions of the vagina & external anogenital epithelium

78
HPV Management of Sex Partners Evaluation of sex partners is not necessary Role of infection is minimal No practical screening tests available for subclinical disease

79
Viral STIs HPV There is no cure for HPV Genital warts can be removed Most HPV infection will go away on its own However, persistent infection is more likely related to (high risk) cancer-types Immunosuppressed individuals are more likely to have persistent infection
 cancer-types Immunosuppressed individuals are more likely to have persistent infection")
Similar presentations









>")








 By: Nathalia Cruz. What is a Virus? ► Exceptionally simple living microbes. ► Contain a single type of nucleic acid (DNA or.>")
 STELLA O. AKPUAKA; KORLU KUYON; AMANDA ROTHENBECKER; ANGELINEMOTARI.>")






 James R. Ginder, MS, WEMT,PI, CHES Health Education Specialist Hamilton County Health Department www.co.hamilton.in.us James.>")