Download presentation
Presentation is loading. Please wait.

1
n Dengue Virus n Adenovirus n Non Polio Enteroviruses Coxsackie virus Coxsackie virus Echovirus Echovirus Enterovirus Enterovirus

2
Dengue Clinical Manifestations and Epidemiology

3
I. Virus, Vector and Transmission

4
Dengue Virus n Causes dengue and dengue hemorrhagic fever n Is an arbovirus n Transmitted by mosquitoes n Composed of single-stranded RNA n Has 4 serotypes (DEN-1, 2, 3, 4)
")
5
Dengue Viruses n Each serotype provides specific lifetime immunity, and short-term cross-immunity n All serotypes can cause severe and fatal disease n Genetic variation within serotypes n Some genetic variants within each serotype appear to be more virulent or have greater epidemic potential

6
Transmission of Dengue Virus by Aedes aegypti Viremia Extrinsic incubation period DAYS 0581216202428 Human #1Human #2 Illness Mosquito feeds / acquires virus Mosquito refeeds / transmits virus Intrinsic incubation period Illness

7
Replication and Transmission of Dengue Virus (Part 1) 1. Virus transmitted to human in mosquito saliva 2. Virus replicates in target organs 3. Virus infects white blood cells and lymphatic tissues 4. Virus released and circulates in blood 3 4 1 2

8
Replication and Transmission of Dengue Virus (Part 2) 5. Second mosquito ingests virus with blood 6. Virus replicates in mosquito midgut and other organs, infects salivary glands 7. Virus replicates in salivary glands 6 7 5

9
Aedes aegypti Mosquito

10
Aedes aegypti n Dengue transmitted by infected female mosquito n Primarily a daytime feeder n Lives around human habitation n Lays eggs and produces larvae preferentially in artificial containers

11
II. Epidemiology

12
World Distribution of Dengue - 2005 Areas infested with Aedes aegypti Areas with Aedes aegypti and dengue epidemic activity

13
Mean Annual Number of DHF Cases Thailand, Indonesia and Vietnam, by Decade * Provisional data through 1998

14
III. Disease Pathogenesis

15
Risk Factors Reported for DHF n Virus strain n Pre-existing anti-dengue antibody previous infection previous infection maternal antibodies in infants maternal antibodies in infants n Host genetics n Age

16
Risk Factors for DHF (continued) n Higher risk in secondary infections n Higher risk in locations with two or more serotypes circulating simultaneously at high levels (hyperendemic transmission)
 n Higher risk in secondary infections n Higher risk in locations with two or more serotypes circulating simultaneously at high levels (hyperendemic transmission)")
17
Increased Probability of DHF Hyperendemicity Increased circulation of viruses Increased probability of secondary infection Increased probability of occurrence of virulent strains Increased probability of immune enhancement Increased probability of DHF Gubler & Trent, 1994

18
Hypothesis on Pathogenesis of DHF (Part 1) n Persons who have experienced a dengue infection develop serum antibodies that can neutralize the dengue virus of that same (homologous) serotype
 n Persons who have experienced a dengue infection develop serum antibodies that can neutralize the dengue virus of that same (homologous) serotype")
19
Neutralizing antibody to Dengue 1 virus 1 1 Dengue 1 virus 1 Homologous Antibodies Form Non-infectious Complexes Non-neutralizing antibody 1 1 Complex formed by neutralizing antibody and virus

20
Hypothesis on Pathogenesis of DHF (Part 2) n In a subsequent infection, the pre-existing heterologous antibodies form complexes with the new infecting virus serotype, but do not neutralize the new virus
 n In a subsequent infection, the pre-existing heterologous antibodies form complexes with the new infecting virus serotype, but do not neutralize the new virus")
21
Non-neutralizing antibody to Dengue 1 virus Dengue 2 virus 2 2 2 2 2 Heterologous Antibodies Form Infectious Complexes Complex formed by non-neutralizing antibody and virus 2

22
Hypothesis on Pathogenesis of DHF (Part 3) n Antibody-dependent enhancement is the process in which certain strains of dengue virus, complexed with non- neutralizing antibodies, can enter a greater proportion of cells of the mononuclear lineage, thus increasing virus production
 n Antibody-dependent enhancement is the process in which certain strains of dengue virus, complexed with non- neutralizing antibodies, can enter a greater proportion of cells of the mononuclear lineage, thus increasing virus production")
23
2 2 2 2 2 2 2 2 2 2 Heterologous Complexes Enter More Monocytes, Where Virus Replicates Non-neutralizing antibody Dengue 2 virus 2 Complex formed by non- neutralizing antibody and Dengue 2 virus 2

24
Hypothesis on Pathogenesis of DHF (Part 4) n Infected monocytes release vasoactive mediators, resulting in increased vascular permeability and hemorrhagic manifestations that characterize DHF and DSS
 n Infected monocytes release vasoactive mediators, resulting in increased vascular permeability and hemorrhagic manifestations that characterize DHF and DSS")
25
Viral Risk Factors for DHF Pathogenesis n Virus strain (genotype) Epidemic potential: viremia level, infectivity Epidemic potential: viremia level, infectivity n Virus serotype DHF risk is greatest for DEN-2, followed by DEN-3, DEN-4 and DEN-1 DHF risk is greatest for DEN-2, followed by DEN-3, DEN-4 and DEN-1
 Epidemic potential: viremia level, infectivity Epidemic potential: viremia level, infectivity n Virus serotype DHF risk is greatest for DEN-2, followed by DEN-3, DEN-4 and DEN-1 DHF risk is greatest for DEN-2, followed by DEN-3, DEN-4 and DEN-1")
26
IV. Clinical Manifestations of Dengue and Dengue Hemorrhagic Fever

27
Dengue Clinical Syndromes n Undifferentiated fever n Classic dengue fever n Dengue hemorrhagic fever n Dengue shock syndrome

28
Undifferentiated Fever n May be the most common manifestation of dengue n Prospective study found that 87% of students infected were either asymptomatic or only mildly symptomatic n Other prospective studies including all age- groups also demonstrate silent transmission

29
Clinical Characteristics of Dengue Fever n Fever n Headache n Muscle and joint pain n Nausea/vomiting n Rash n Hemorrhagic manifestations

30
Signs and Symptoms of Encephalitis/Encephalopathy Associated with Acute Dengue Infection n Decreased level of consciousness: lethargy, confusion, coma n Seizures n Nuchal rigidity n Paresis

31
Hemorrhagic Manifestations of Dengue n Skin hemorrhages: petechiae, purpura, ecchymoses n Gingival bleeding n Nasal bleeding n Gastro-intestinal bleeding: hematemesis, melena, hematochezia n Hematuria n Increased menstrual flow

32
Clinical Case Definition for Dengue Hemorrhagic Fever n Fever, or recent history of acute fever n Hemorrhagic manifestations n Low platelet count (100,000/mm 3 or less) n Objective evidence of “leaky capillaries:” elevated hematocrit (20% or more over baseline) elevated hematocrit (20% or more over baseline) low albumin low albumin pleural or other effusions pleural or other effusions 4 Necessary Criteria:
 n Objective evidence of leaky capillaries: elevated hematocrit (20% or more over baseline) elevated hematocrit (20% or more over baseline) low albumin low albumin pleural or other effusions pleural or other effusions 4 Necessary Criteria:")
33
Clinical Case Definition for Dengue Shock Syndrome n 4 criteria for DHF n Evidence of circulatory failure manifested indirectly by all of the following: Rapid and weak pulse Rapid and weak pulse Narrow pulse pressure ( 20 mm Hg) OR hypotension for age Narrow pulse pressure ( 20 mm Hg) OR hypotension for age Cold, clammy skin and altered mental status Cold, clammy skin and altered mental status n Frank shock is direct evidence of circulatory failure
 OR hypotension for age Narrow pulse pressure ( 20 mm Hg) OR hypotension for age Cold, clammy skin and altered mental status Cold, clammy skin and altered mental status n Frank shock is direct evidence of circulatory failure")
34
Four Grades of DHF n Grade 1 Fever and nonspecific constitutional symptoms Fever and nonspecific constitutional symptoms Positive tourniquet test is only hemorrhagic manifestation Positive tourniquet test is only hemorrhagic manifestation n Grade 2 Grade 1 manifestations + spontaneous bleeding Grade 1 manifestations + spontaneous bleeding n Grade 3 Signs of circulatory failure (rapid/weak pulse, narrow pulse pressure, hypotension, cold/clammy skin) Signs of circulatory failure (rapid/weak pulse, narrow pulse pressure, hypotension, cold/clammy skin) n Grade 4 Profound shock (undetectable pulse and BP) Profound shock (undetectable pulse and BP)
 Signs of circulatory failure (rapid/weak pulse, narrow pulse pressure, hypotension, cold/clammy skin) n Grade 4 Profound shock (undetectable pulse and BP) Profound shock (undetectable pulse and BP)")
35
Danger Signs in Dengue Hemorrhagic Fever n Abdominal pain - intense and sustained n Persistent vomiting n Abrupt change from fever to hypothermia, with sweating and prostration n Restlessness or somnolence Martínez Torres E. Salud Pública Mex 37 (supl):29-44, 1995.
:29-44,")
36
Warning Signs for Dengue Shock When Patients Develop DSS: 3 to 6 days after onset of symptoms When Patients Develop DSS: 3 to 6 days after onset of symptoms Initial Warning Signals: Disappearance of fever Drop in platelets Increase in hematocrit Initial Warning Signals: Disappearance of fever Drop in platelets Increase in hematocrit Alarm Signals: Severe abdominal pain Prolonged vomiting Abrupt change from fever to hypothermia Change in level of consciousness (irritability somnolence) Alarm Signals: Severe abdominal pain Prolonged vomiting Abrupt change from fever to hypothermia Change in level of consciousness (irritability somnolence) Four Criteria for DHF: Fever Hemorrhagic manifestations Excessive capillary permeability 100,000/mm 3 platelets Four Criteria for DHF: Fever Hemorrhagic manifestations Excessive capillary permeability 100,000/mm 3 platelets
 Alarm Signals: Severe abdominal pain Prolonged vomiting Abrupt change from fever to hypothermia Change in level of consciousness (irritability somnolence) Four Criteria for DHF: Fever Hemorrhagic manifestations Excessive capillary permeability 100,000/mm 3 platelets Four Criteria for DHF: Fever Hemorrhagic manifestations Excessive capillary permeability 100,000/mm 3 platelets")
37
Unusual Presentations of Severe Dengue Fever n Encephalopathy n Hepatic damage n Cardiomyopathy n Severe gastrointestinal hemorrhage

38
V. Diagnosis

39
General Recommendations for Medical Care n Epidemiologic considerations Season of year Season of year Travel history Travel history n Diagnosis n Treatment n Follow-up

40
Travel History n Important for assessment of symptomatic patients in non- endemic areas n Determine whether the patient travelled to a dengue-endemic area n Determine when the travel occurred If the patient developed fever more than 2 weeks after travel, eliminate dengue from the differential diagnosis If the patient developed fever more than 2 weeks after travel, eliminate dengue from the differential diagnosis

41
Differential Diagnosis of Dengue n Influenza n Measles n Rubella n Malaria n Typhoid fever n Leptospirosis n Meningococcemia n Rickettsial infections n Bacterial sepsis n Other viral hemorrhagic fevers

42
Clinical Evaluation in Dengue Fever n Blood pressure n Evidence of bleeding in skin or other sites n Hydration status n Evidence of increased vascular permeability-- pleural effusions, ascites n Tourniquet test

43
Petechiae

44
Vaughn DW, Green S, Kalayanarooj S, et al. Dengue in the early febrile phase: viremia and antibody responses. J Infect Dis 1997; 176:322-30. A B PEI = A/B x 100 Pleural Effusion Index

45
Tourniquet Test n Inflate blood pressure cuff to a point midway between systolic and diastolic pressure for 5 minutes n Positive test: 20 or more petechiae per 1 inch 2 (6.25 cm 2 )
")
46
Positive Tourniquet Test

47
Laboratory Tests in Dengue Fever n Clinical laboratory tests CBC--WBC, platelets, hematocrit CBC--WBC, platelets, hematocrit Albumin Albumin Liver function tests Liver function tests Urine--check for microscopic hematuria Urine--check for microscopic hematuria n Dengue-specific tests Virus isolation Virus isolation Serology Serology

48
Laboratory Methods for Dengue Diagnosis, CDC Dengue Branch n Virus isolation to determine serotype of the infecting virus n IgM ELISA test for serologic diagnosis

49
Virus Isolation: Cell Culture

51
Virus Isolation: Mosquito Inoculation

52
Virus Isolation: Fluorescent Antibody Test

53
ELISA Test for Serologic Diagnosis

54
ELISA Plate

55
Collection and Processing of Samples for Laboratory Diagnosis Type of Specimen Time of Collection Type of Analysis Acute-phase blood (0-5 days after onset) When patient presents; collect second sample during convalescence Virus isolation and/or serology Convalescent-phase blood ( 6 days after onset) Between days 6 and 21 after onset Serology
 When patient presents; collect second sample during convalescence Virus isolation and/or serology Convalescent-phase blood ( 6 days after onset) Between days 6 and 21 after onset Serology")
56
Temperature, Virus Positivity and Anti-Dengue IgM, by Fever Day Dengue IgMMean Max. TemperatureVirus Adapted from Figure 1 in Vaughn et al., J Infect Dis, 1997; 176:322-30. Fever Day 0 20 40 60 80 100 Percent Virus Positive -4-3-20123456 39.5 39.0 38.5 38.0 37.5 37.0 Temperature (degrees Celsius) Dengue IgM (EIA units) 300 150 0 75 225
 Dengue IgM (EIA units)")
57
VI. Treatment

58
Outpatient Triage n No hemorrhagic manifestations and patient is well-hydrated: home treatment n Hemorrhagic manifestations or hydration borderline: outpatient observation center or hospitalization n Warning signs (even without profound shock) or DSS: hospitalize
 or DSS: hospitalize")
59
Patient Follow-Up n Patients treated at home Instruction regarding danger signs Instruction regarding danger signs Consider repeat clinical evaluation Consider repeat clinical evaluation n Patients with bleeding manifestations Serial hematocrits and platelets at least daily until temperature normal for 1 to 2 days Serial hematocrits and platelets at least daily until temperature normal for 1 to 2 days n All patients If blood sample taken in first 5 days after onset, need convalescent sample between days 6 - 30 If blood sample taken in first 5 days after onset, need convalescent sample between days 6 - 30 All hospitalized patients need samples on admission and at discharge or death All hospitalized patients need samples on admission and at discharge or death

60
Treatment of Dengue Fever (Part 1) n Fluids n Rest n Antipyretics (avoid aspirin and non- steroidal anti-inflammatory drugs) n Monitor blood pressure, hematocrit, platelet count, level of consciousness
 n Fluids n Rest n Antipyretics (avoid aspirin and non- steroidal anti-inflammatory drugs) n Monitor blood pressure, hematocrit, platelet count, level of consciousness")
61
Mosquito Barriers n Only needed until fever subsides, to prevent Aedes aegypti mosquitoes from biting patients and acquiring virus n Keep patient in screened sickroom or under a mosquito net

62
Treatment of Dengue Fever (Part 2) n Continue monitoring after defervescence n If any doubt, provide intravenous fluids, guided by serial hematocrits, blood pressure, and urine output n The volume of fluid needed is similar to the treatment of diarrhea with mild to moderate isotonic dehydration (5%-8% deficit)
 n Continue monitoring after defervescence n If any doubt, provide intravenous fluids, guided by serial hematocrits, blood pressure, and urine output n The volume of fluid needed is similar to the treatment of diarrhea with mild to moderate isotonic dehydration (5%-8% deficit)")
63
Treatment of Dengue Fever (Part 3) n Avoid invasive procedures when possible n Unknown if the use of steroids, intravenous immune globulin, or platelet transfusions to shorten the duration or decrease the severity of thrombocytopenia is effective n Patients in shock may require treatment in an intensive care unit
 n Avoid invasive procedures when possible n Unknown if the use of steroids, intravenous immune globulin, or platelet transfusions to shorten the duration or decrease the severity of thrombocytopenia is effective n Patients in shock may require treatment in an intensive care unit")
64
Indications for Hospital Discharge n Absence of fever for 24 hours (without anti-fever therapy) and return of appetite n Visible improvement in clinical picture n Stable hematocrit n 3 days after recovery from shock Platelets 50,000/mm 3 Platelets 50,000/mm 3 n No respiratory distress from pleural effusions/ascites
 and return of appetite n Visible improvement in clinical picture n Stable hematocrit n 3 days after recovery from shock Platelets 50,000/mm 3 Platelets 50,000/mm 3 n No respiratory distress from pleural effusions/ascites")
65
Common Misconceptions about Dengue Hemorrhagic Fever 8 Dengue + bleeding = DHF 4 Need 4 WHO criteria, capillary permeability 8 DHF kills only by hemorrhage 4 Patient dies as a result of shock 8 Poor management turns dengue into DHF 4 Poorly managed dengue can be more severe, but DHF is a distinct condition, which even well-treated patients may develop 8 Positive tourniquet test = DHF 4 Tourniquet test is a nonspecific indicator of capillary fragility

66
More Common Misconceptions about Dengue Hemorrhagic Fever 8 DHF is a pediatric disease 4 All age groups are involved in the Americas 8 DHF is a problem of low income families 4 All socioeconomic groups are affected 8 Tourists will certainly get DHF with a second infection 4 Tourists are at low risk to acquire DHF

67
Dengue Vaccine? n No licensed vaccine at present n Effective vaccine must be tetravalent n Field testing of an attenuated tetravalent vaccine currently underway n Effective, safe and affordable vaccine will not be available in the immediate future

68
VII. Prevention

69
Early Eradication Campaigns Succeeded n Adequate local and external funding for personnel, equipment and insecticides n Emphasis on source reduction n Effective residual insecticide n Centralized, vertically-structured programs with military-type organization, strict supervision, high level of discipline

70
Reinfestation by Aedes aegypti 1930s 1970 1998

71
Lessons for Future Dengue Prevention Programs n Efforts should focus on sustainable environmental control rather than eradication n Control programs should be community-based and -integrated. They cannot rely solely on insecticides nor require large budgets n Need to promote dengue as a priority among health officials and the general public

72
Community Approaches n Typically define communities geographically n More likely to be sustainable n Advantages: built-in manpower, help develop resources and empower community organizations n Disadvantages: more difficult to organize, take longer to get off the ground

73
Community Participation n First must educate the public in the basics of dengue, such as: Where the mosquito lays her eggs Where the mosquito lays her eggs The link between larvae and adult mosquitoes The link between larvae and adult mosquitoes General information about dengue transmission, symptoms and treatment General information about dengue transmission, symptoms and treatment

74
Barriers and Motivation (Part 2) n Structural factors laws regarding Aedes aegypti habitats laws regarding Aedes aegypti habitats n Environmental factors lack of potable water, need to store water lack of potable water, need to store water inadequate solid waste disposal inadequate solid waste disposal n Attitudinal factors beliefs: causes, treatment, prevention of febrile illnesses beliefs: causes, treatment, prevention of febrile illnesses n Community factors community history and structure community history and structure other priority problems in the community other priority problems in the community
 n Structural factors laws regarding Aedes aegypti habitats laws regarding Aedes aegypti habitats n Environmental factors lack of potable water, need to store water lack of potable water, need to store water inadequate solid waste disposal inadequate solid waste disposal n Attitudinal factors beliefs: causes, treatment, prevention of febrile illnesses beliefs: causes, treatment, prevention of febrile illnesses n Community factors community history and structure community history and structure other priority problems in the community other priority problems in the community")
75
Cues: Water Shortages and Rationing n For locations where there are seasonal or other temporary water shortages n Provide information on how to properly store water

76
Cues: Rainfall n Link rainfall to the creation of larval habitats n This mental link can remind people to look for and eliminate larval habitats after it rains n Eliminates larval habitats influenced by rainfall, and perhaps others as well

77
Adenovirus Infection Age incidence: 6mo – 5 y/o Mode of transmission 1.Direct contact – airborne or droplet 2.Indirect contact with articles and environment 3.Fecal oral route Incubation period: 2-14 days – respiratory 3-10 days - GIT

78
Adenovirus Infection Clinical Manifestations: 3. GIT a. gastroenteritis b. mesenteric lymphodenitis c. intususception d. appendicitis e. hepatitis

79
Adenovirus Infection 51 serotypes Types 3, 4, 7, 21 – respiratory 8, 18, 37 – epidemic heretoconjunctivitis 40, 41, 31 - gastroenteritis

80
Adenovirus Infection Clinical Manifestations: 1.Respiratory a. Colds/nasopharyngitis, tonsillitis b. Pharyngo- conjunctival fever c. bronchitis d. pneumonia e. pertussis – like syndrome 2. Ocular - epidemic conjunctivitis

81
Adenovirus Infection Clinical Manifestations: 3. GIT a. gastroenteritis b. mesenteric lymphodenitis c. intususception d. appendicitis e. hepatitis

82
Adenovirus Infection Clinical Manifestations: 4. GUT a. acute hemorrhagic cystitis b. nephritis c. orchitis 5. Heart a. myocarditis/pericarditis 6. Neurology a. meningitis/encephalitis

83
Adenovirus Infection Diagnosis 1.Clinical 2.Viral isolation 3.Other: a.Immunoflourescence b.ELISA c.PCR d.Electron microscopy

84
Adenovirus Infection Treatment: Supportive

85
Enterovirus Infection RNA varices 1.Coxsackievirus group A 2.Coxsackievirus group B 3.Echovirus 4.enterovirus

86
Nonpolio Enteroviruses Exanthems n Coxsackievirus group A n Coxsackievirus group B n Echoviruses n Enteroviruses

87
Enterovirus Infection Sources: feces oropharyngeal secretions Mode of transmission: Oral fecal route Oral – oral route Increase incidence: 1. young children 2. low socio-economic group 3. unhygienic, economically deprived population Incubation period: 3-6 days

88
Coxsackievirus Coxsackievirus group A 6 Various presentation of rash Erythematous and maculopapular Vesicular Urticaria and Urticaria plus fever: r/o infectious origin

89
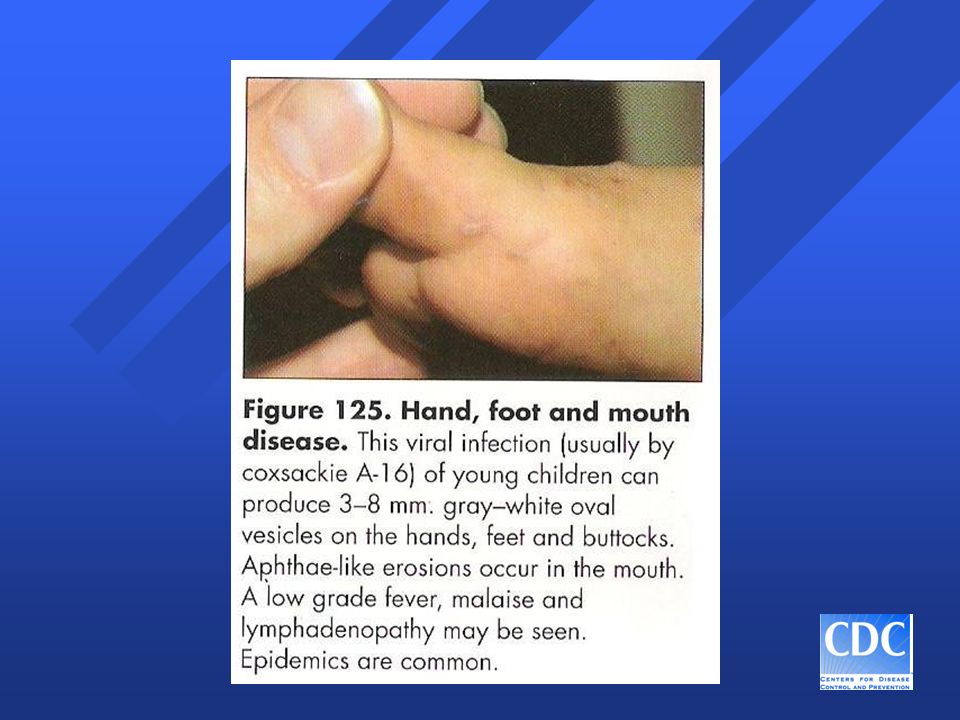
Coxsackievirus Coxsackievirus group A 16 Hand-foot and mouth syndrome Enanthem: large vesicularicular lesions (1- 2cm.) on buccal surfaces, tongue, palate, uvula, anterior tonsil pillars, and gums Exanthem: large vesicular lesions on hand feet, and buttocks
 on buccal surfaces, tongue, palate, uvula, anterior tonsil pillars, and gums Exanthem: large vesicular lesions on hand feet, and buttocks")
92
Echovirus 9 Associated with epidemics Incubation period: 4-6 days Clinical manifestations: 1.Noexudative pharyngitis (50%) 2.Cough, sore throat 3.Cervical lymphadenopathy 4.Abdominal pain
 2.Cough, sore throat 3.Cervical lymphadenopathy 4.Abdominal pain")
93
Echovirus 9 Clinical manifestations: 5. Aseptic meningitis 6. Rash: a. Erythematous b. Maculopapular c. Petechial/petechial component

94
Echovirus 9 Laboratory: Pleocytosis with predominance of neutrophils Differential diagnosis: Meningococcemia

95
Thank You!

Similar presentations












 Walden University PUBH 8165 Instructor: Dr. Fredric Grant Summer 2013.>")
 are viruses that can be transmitted to man by arthropod vectors. Arboviruses belong to three.>")






 Virus>")