Download presentation
Presentation is loading. Please wait.

1
Reducing Wrong RN Calls Kaitlin Baron Josh Macht

2
Reasons for Action ● Nurses often call the wrong team room, which can cause delays in patient care and waste everyone’s time ● Process Start: When the patient is admitted ● Process End: When the patient is discharged ● In Scope: The 4 VA medicine teams ● Out of Scope: The other medicine teams

3
Current State Decision to admit ER or admitting resident placed white card Admitting Dept processes white card, assigned pt an attending and team if all data is correct Admitting Dept assigns pt to correct CPRS list, calls unit and gives them correct team name to place on wall and on paper chart Likelihood of calls to wrong team significantly reduced, however RN still has no way to know intern A/B assignment Or Else Admitting Dept assigns pt to wrong CPRS list, unit given wrong information which is placed on wall and paper chart Likelihood of wrong calls significantly increased No current workflow to fix this mistake. Misinformation persists throughout hospitalization leading to wrong calls and delays in care. ●Talked to nurses on 3A and 3B about how they figure out which team the patients are on ●Talked to ward clerks about what they do with printed orders such as the adjusted whitecard ●Talked to case managers about how they figure which patients are on their team ●METRIC: Tally survey from 4 medicine teams about the number of calls to the team room about patients not on their team for 4 days

4
Target State Decision to admit ER or admitting resident placed white card Admitting Dept processes white card, assigned pt an attending and team if all data is correct Admitting Dept assigns pt to correct CPRS list, calls unit and gives them correct team name to place on wall and on paper chart Likelihood of calls to wrong team significantly reduced, however RN still has no way to know intern A/B assignment Or Else Admitting Dept assigns pt to wrong CPRS list, unit given wrong information which is placed on wall and paper chart Likelihood of wrong calls significantly increased Upon receiving a new patient (during call day, or the next AM on short/long call), the resident checks white card, fixes mistakes and adds intern A/B assignment White card printed to appropriate nursing station, ward clerk updates the board and binder with correct information All locations RNs look for team assignments that are now corrected, and the likelihood of wrong calls is significantly reduced ●GOAL: 50% reduction in wrong calls
, the resident checks white card, fixes mistakes and adds intern A/B assignment White card printed to appropriate nursing station, ward clerk updates the board and binder with correct information All locations RNs look for team assignments that are now corrected, and the likelihood of wrong calls is significantly reduced ●GOAL: 50% reduction in wrong calls")
5
Gap Analysis Decision to admit ER or admitting resident placed white card Admitting Dept processes white card, assigned pt an attending and team if all data is correct Admitting Dept assigns pt to correct CPRS list, calls unit and gives them correct team name to place on wall and on paper chart Likelihood of calls to wrong team significantly reduced, however RN still has no way to know intern A/B assignment Else Admitting Dept assigns pt to wrong CPRS list, unit given wrong information which is placed on wall and paper chart Likelihood of wrong calls significantly increased Upon receiving a new patient (during call day, or the next AM on short/long call), the intern checks white card, fixes mistakes and adds intern A/B assignment White card printed to appropriate nursing station, unit secretary updates the board with correct information All locations RNs look for team assignments are now corrected, likelihood of wrong calls significantly reduced Difficult to completely solve: -ER doesn’t know admitting team -Resident doesn’t know admitting team -White card signed with missing information -Admitting team changed by the time pt arrives Easier to solve. Plus, even if you could fix the initial problem, you would still need a workflow to correct mistakes New Workflow

6
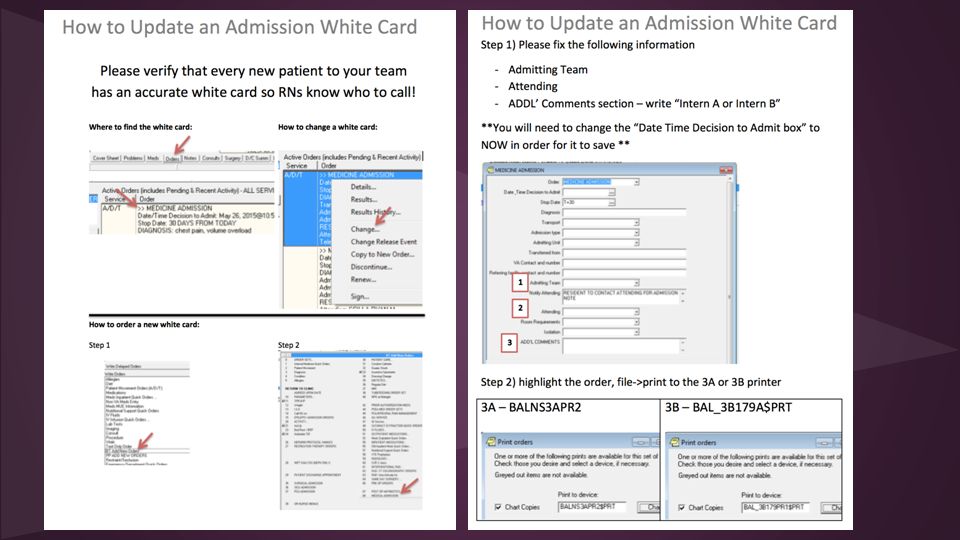
Countermeasures / Solution Approach ● If we teach residents how to put in/adjust a white card... then we expect they will do this for each patient to make sure the team color, attending name, and A or B intern will be correct. ● If we teach nurses where to find the white card… then we expect they will know the right team for each patient. ● If we teach ward clerks to look at the printed out order with the adjusted white card… then we expect them to update the patient’s team on the whiteboard and binder.

8
Countermeasures / Solution Approach ● If we teach the case managers to look at the adjusted white card… then we expect them to add the patients to the right team list. ● If we get residents access to adjusting the team lists… then we expect the team lists to be accurate all of the time.

9
Rapid Experiments # of Wrong Calls to all 4 Team Rooms Over 4 Days Week 1 - Pre- intervention 36 Week 2 - Post- intervention 19 OVERALL: 47% REDUCTION IN WRONG CALLS!!

10
Raw Data GreenPurpleYellowOrange Monday1221 Tuesday7232 Wednesday3332 Thursday1022 GreenPurpleYellowOrange Monday1205 Tuesday0021 Wednesday2200 Thursday3010 Pre Post

11
Implementation / Completion Plans ● Residents on each team update the white cards for their new patients each morning after sign out to reflect the accurate team color, attending, and intern A or B. ● Nurses are trained on where to find the white cards, which are now going to be correct all of the time. ● Ward clerks are trained to look at the printed adjusted white cards and adjust the whiteboard and binders accordingly.

12
Implementation / Completion Plans ● Case managers are trained on how to find the adjusted white cards and update the team lists each morning. ● ULTIMATE GOAL: Residents are able to update the team lists themselves!!! (Mona is going to talk to the administration about this possibility. )
.")
13
Insights ● Residents don’t mind performing this new workflow, but need more formal training on how to complete it properly and more time to remember to integrate it into their daily routine. ● RNs need formal training on where to find the white card and how to read it for the information they need. ● Ward clerks need formal training on reading white cards that come off the printer, and more motivation to participate in this new workflow. ● Case management struggles with this same problem daily, goes to each team room to look at the board and fix their own personal team list. They could easily be hooked into this process as another way to catch errors, and possibly to fix them. ● Once this workflow is running smoothly and catching all team assignment errors it should go back and work on the root problem of the initial white card being incomplete/incorrect.

Similar presentations

: An Intervention to Learn form Mistakes and Improve Safety Culture.>")




.>")







 Use Your Planner>")




