Download presentation
Presentation is loading. Please wait.

1
“Advanced” EKG Reading Stefan Da Silva With special guest…. Dr. S. Weeks

2
Outline Quick review of EKG basic interpretation Dr. Weeks to take over

3
Basics Can’t really do the “advanced” without the basics. Rate, Rhythm, Axis, Intervals, Infarction

4
Basics Rate –SA node NORMALLY sets rate, usually cannot fire faster then ~ 220 bpm. –Ectopic beats will fire whenever they want and are usually considered abnormal (PVC, PAC, etc). Atrial ectopic pacemakers inherently fires ~75 bpm AV nodal pacemaker enjoys ~60 bpm Ventricular pacemaker likes 30 – 40 bpm (idoventricular rhythm) HOWEVER, all the above will fire between 150 – 250 bpm in pathological and emergency situations and ectopic pacemakers will take over the rhythm when they are firing faster that SA node. When the SA node fails and the “ectopic” site takes over that = escape beat/rhythm. Tachycardia and Bradycardia 300, 150, 100 then 75, 60, 50 (measured from R wave to R wave)
. Atrial ectopic pacemakers inherently fires ~75 bpm AV nodal pacemaker enjoys ~60 bpm Ventricular pacemaker likes 30 – 40 bpm (idoventricular rhythm) HOWEVER, all the above will fire between 150 – 250 bpm in pathological and emergency situations and ectopic pacemakers will take over the rhythm when they are firing faster that SA node. When the SA node fails and the ectopic site takes over that = escape beat/rhythm. Tachycardia and Bradycardia 300, 150, 100 then 75, 60, 50 (measured from R wave to R wave).")
5
Basics Rhythm –Sinus vs non-sinus –Regular vs Irregular –Sinus: P wave in front of every QRS with P wave positive in II, III, aVF and neg in aVR. –Sinus arrhythmia: Irregular rhythm but identical p waves –Non-sinus Can be: varying rhythm, extra/skipped beats, rapid rhythm, heart blocks.

6
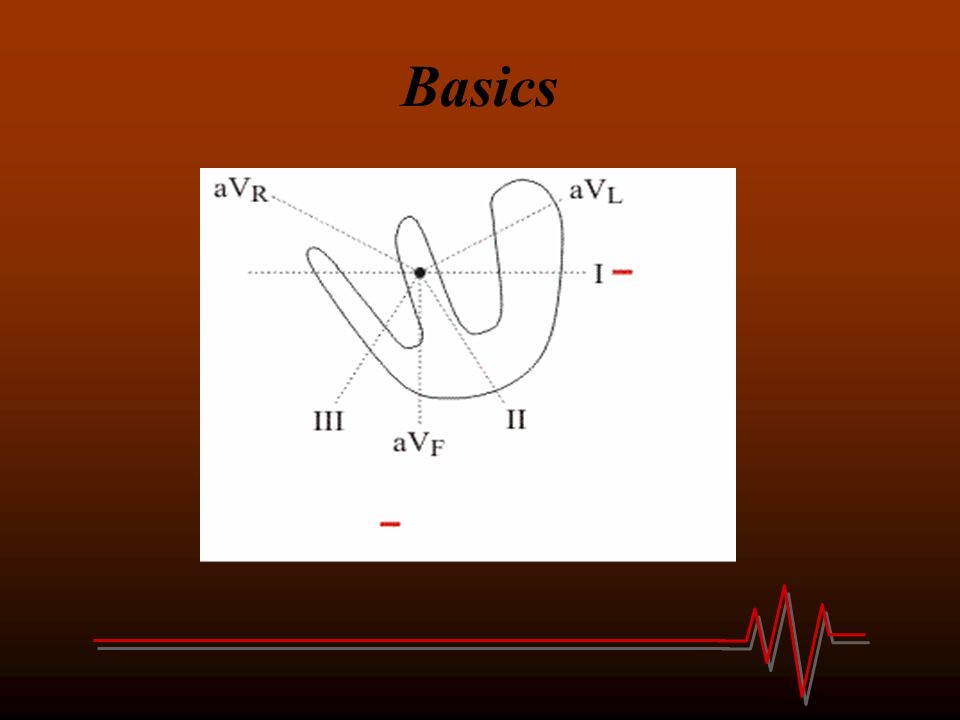
Basics Axis –More than just “thumb up/thumb down” and leads I and aVF –Refers to direction of electrical stimulus/depolarization. –Related to ventricular depolarization Mean QRS vector = general direction of ventricular depolarization Usually pointed downward and slightly to left since the “vectors” representing depolarization of left ventricle are larger due to thicker wall and septum (septum usually depolarizes from left to right.)
.")
7
Basics

9
Mean QRS vector

10
Basics Remember these diagrams

11
Basics Axis –Therefore if heart is displaced to right then Mean QRS vector will be displaced as well –A hypertrophied ventricle has greater electrical activity therefore mean vector will be displaced to that side –In infarction, dead myocardium cannot conduct therefore mean QRS vector tends to point away from infarcted area.

12
Basics Axis –Calculation:

13
Basics Axis –Examine lead I If positive QRS then vector located in left half If negative QRS then vector located in right half –Examine lead aVF If positive QRS then vector points downward If negative QRS then vector points upward –This will give you the general quadrant ie. Why the thumb rule works….

14
Basic Axis –Then find most isoelectric lead and mean vector will be at about 90 degrees towards the already specified quadrant –Plot it out….it helps. –Why is axis important…. It can help with diagnosis – extreme RAD Vtach, hyperK…. –RAD RVH, PE, VSD… –LAD inf MI, hyperK, poor LV function, dilated LV, LAFB, LVH.

15
Basics Intervals/Segments –PR interval Start of P wave to start of QRS Normal: 0.12 - 0.2 sec –Remember each small square is 0.04 sec –QRS interval Start of QRS to end of QRS Normal: < 0.12 –QT interval Start of Q wave (or R wave if not Q) to termination of T wave. Quick and dirty: usually prolonged if greater than half the R-R interval QTc:

16
Basics Bundle Branch Block –More than the “bunny ears” –Leads V1 and V6 (chest leads) –Determine which direction the “last” half of the QRS is pointing, it will point to the ventricle that is depolarizing last, which will be the side of the bundle branch block. –Dr. Weeks to explain better than me….

17
Basics A little more on P waves –Ensure going in right direction –Tall P wave lead II right atrial abnormality (look for RAD, RVH) –Wide P wave lead II +/- negative portion V1 left atrial abnormality (look for MR, MS, AS, HCM)
 –Wide P wave lead II +/- negative portion V1 left atrial abnormality (look for MR, MS, AS, HCM)")
18
Basics –Hypertrophy Increase in the thickness of the wall of that chamber. Right Ventricular Hypertrophy –R wave of V1 gets progessively smaller Left Ventricular Hypertrophy –S wave in V1 plus R wave in V5 > 35 mm –T wave inversion can also occur –Also if > 10mm in I or aVL then LVH

19
Basics Infarction –Ischemia, injury, infarction –T wave inversion ischemia –ST segment elevation/depression injury Elevation = > 1 mm in 2 or more contigous leads Depression = > 0.5 mm in 2 or more contigous leads

20
Basics I LateralaVRV1 SeptalV4 Anterior II InferioraVL LateralV2 SeptalV5 Lateral III InferioraVF Inferior V3 AnteriorV6 Lateral

21
Basics Lots to remember and lots of variation but remember the basics and then work from there….

Similar presentations
















>")


