Download presentation
Presentation is loading. Please wait.

1
THE URBAN INSTITUTE Examining Long-Term Care Episodes and Care History for Medicare Beneficiaries: A Longitudinal Analysis of Elderly Individuals with Congestive Heart Failure Stephanie Maxwell & Timothy Waidmann APHA Annual Meeting Boston, MA November 6, 2006

2
Background Congestive heart failure (CHF) is the leading medical condition among the elderly. Significant policy concern regarding CHF hospitalization rates CHF is a common target of disease management programs. Few large-scale studies have explored the CHF patients’ use of long-term care (LTC) services and Medicare services combined
 services and Medicare services combined.")
3
Overview of Study Design Longitudinal (36-month) analyses National cohort of elderly who were first hospitalized for CHF in 1999. Identify patterns over three years of Medicare service use and spending, enrollment in Medicaid, and nursing home entry. Estimate hazard models of risks of re-hospitalization, nursing home admission and death, controlling for health status.

4
Data Sources (mainly 1999-2002 files) 100% Medicare claims files (all service types) 100% Medicare enrollment files 100% MDS patient assessment records Area Resource File and Interstudy HMO Files
 100% Medicare claims files (all service types) 100% Medicare enrollment files 100% MDS patient assessment records Area Resource File and Interstudy HMO Files")
5
Defining the Cohort in the Claims Data Final cohort = 296,462 elderly Cohort consists of elderly hospitalized, in 1999, for their first hospitalization for CHF. The principal diagnosis field of acute hospital records was searched for a set of diagnosis codes indicating CHF as the primary reason for hospitalization. Scanned a 5-year “look-back” period of hospital claims (1994-1998 claims) to screen out individuals whose first CHF admission occurred before 1999. To assure a comparable “look-back period”, we included only those age- eligible for Medicare in January 1994 in the cohort.
 to screen out individuals whose first CHF admission occurred before To assure a comparable look-back period , we included only those age- eligible for Medicare in January 1994 in the cohort..")
6
Statistical Methods Bivariate analyses -- of outcomes stratified by patient and area characteristics Survival models -- to estimate the effects of covariates on the instantaneous risk of an outcome, through measuring the elapsed time before an outcome is observed. Two-part use and spending models – estimated models for the first six months following CHF hospitalization and also for the three years following CHF hospitalization.

7
Outcomes Measures of Hazard Models Survival Subsequent CHF hospitalization Subsequent non-CHF hospitalization Medicaid enrollment Nursing home entry

8
Outcomes Measures of Two-Part Use and Spending Models CHF hospitalizations Other hospitalizations SNF stays Home health use Hospital outpatient use Physician services use

9
Person-Level Independent Variables Demographics (age group, race, sex) Charlson comorbidity score Length of stay of the index CHF hospitalization Nursing home use prior to index CHF hospitalization Utilization and spending variables between the index CHF hospitalization and outcome: Quarterly physician spending Quarterly hospital outpatient spending Quarterly acute hospital spending (except in models of death and non-CHF hospitalizations) CHF hospitalizations (except when used as an outcome) Oher hospitalizations (except when use as an outcome) SNF stays Medicare home health use Nursing home use (except when used as an outcome)
 Charlson comorbidity score Length of stay of the index CHF hospitalization Nursing home use prior to index CHF hospitalization Utilization and spending variables between the index CHF hospitalization and outcome: Quarterly physician spending Quarterly hospital outpatient spending Quarterly acute hospital spending (except in models of death and non-CHF hospitalizations) CHF hospitalizations (except when used as an outcome) Oher hospitalizations (except when use as an outcome) SNF stays Medicare home health use Nursing home use (except when used as an outcome)")
10
County-Level Independent Variables Urban influence HMO penetration Median county income Supply rates per 1000 elderly: –All physicians –Cardiologists –Short-term hospital beds –Long-term hospital beds –SNF beds –Nursing home beds Presence of a facility in the county: –Short-term hospital –Nursing home –Rural health clinic –Federally qualified health clinic Population mortality rates for 10 selected medical conditions

11
Summary of Findings Over 3 years following index hospitalization for CHF: 36% had additional CHF hospitalizations 68% had hospitalizations for other conditions 42% had SNF stays 15% entered a nursing home (non-Medicare) 7% enrolled in Medicaid 56% died 11% had NH use prior to their index CHF hospitalization Average 3-year spending = $35,000 –Non-CHF hospitalizations was largest source of spending
 7% enrolled in Medicaid 56% died 11% had NH use prior to their index CHF hospitalization Average 3-year spending = $35,000 –Non-CHF hospitalizations was largest source of spending")
12
Findings – Death SNF use is the dominant risk Age -- 5 additional years 13% to 30% higher risk Charlson -- additional comorbidity 10% higher risk Index LOS -- additional day 2% higher risk SNF use 200% higher risk Physician spending per quarter ($thousands) 15 to 40% higher risk NF use 15% to 47% higher risk
 15 to 40% higher risk NF use 15% to 47% higher risk")
14
Findings – CHF Hospitalizations Approximately 15% increased risk associated with: 5-year age increase Additional comorbidity Race: Black Physician spending per quarter ($thousands) Home health use Whites have higher death risks and blacks have higher rehospitalization risks. This is consistent with each other in suggesting that whites are more severely ill once hospitalized.

16
Findings – Other Hospitalizations Compared to CHF hospitalization, key differences are regarding race and home health use Blacks 10% to 20% higher risk for CHF hospitalizations But blacks 5% to 10% lower risk for other hospitalizations Home health use 15% higher risk for CHF hospitalizations But home health use 20% lower risk for other hospitalizations

18
Findings – Nursing Home Entry SNF use and prior NH use are dominant risks SNF use several hundred percent higher risk Prior NH use 100% higher risk Additional CHF hospitalizations 20% higher risk Other hospitalizations 5% to 20% higher risk

20
Findings – Medicaid Enrollment SNF use and NH use are the dominant risks (200% to 300% higher risk) Three factors each increasing risk by ~ 6% to 24%: Prior NH use Hospitalizations Home health use Race: black 40% to 100% higher risk
 Three factors each increasing risk by ~ 6% to 24%: Prior NH use Hospitalizations Home health use Race: black 40% to 100% higher risk")
22
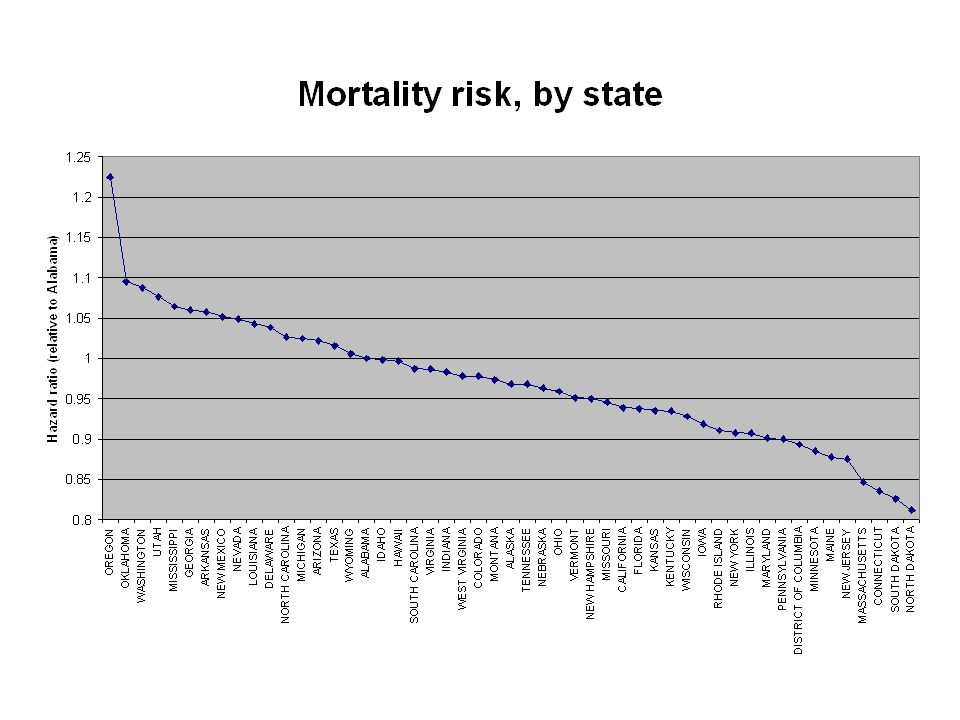
Methodological Contributions to the CHF Literature Large-scale, national study of CHF population with a long follow- up (36 months). Survival analysis jointly accounts for utilization and mortality risk. This is important when studying elderly or high-mortality conditions. Logistic regression may give misleading impressions. Controlled for health status using comorbidity index and prior nursing home use. Controlled for area variation using state and 6-level urban influence variable. In terms of urban influence, risks hinged on large metro county residence. An urban/rural flag would incorrectly attribute practice patterns typical in large center cities to the surrounding metro areas and to smaller cities.

23
Conclusions Higher CHF rehospitalization among African Americans. Target for disease management programs? Bivariate findings suggest decreasing intensity of care with age. Multivariate models do not. Importance of more than CHF hospitalization in cohort. Geographic variation in utilization and health.

24
Main Study Limitation: Missing Data on Social Support, Income, Functional Status This study had mixed findings regarding the effect (sign) of home health use on outcomes. Our findings on home health use in relation to SNF use may point to influential characteristics not available in our data: social support, individual income, and ADL information on community residents. The importance of these factors in understanding LTC use is well-established in the literature. This study’s findings suggest that these factors may be important in understanding medical use as well, when examining a chronic and ultimately debilitating disease like CHF.

25
Principal Investigators: Stephanie Maxwell, PhD and Timothy Waidmann, PhD smaxwell@ui.urban.org twaidman@ui.urban.org 202-261-5825 202-261-5718 Health Policy Center The Urban Institute 2100 M Street, NW Washington, DC 20037 fax: 202-223-1149 Funder: Centers for Medicare and Medicaid Services THE URBAN INSTITUTE

Similar presentations




 Lee Feb. 9 th, 2007.>")






 Data: A Researcher’s Perspective Judith H. Lichtman, PhD MPH Associate.>")











