Download presentation
Presentation is loading. Please wait.

1
Echocardiography in ICU Michel Slama AmiensFrance LEVEL 1 basic LEVEL 2: advanced

2
How to use echocardiography in ICU patients Two clinical situations Unexplained shock Unexplained respiratory failure

3
How to use echocardiography in ICU patients Two clinical situations Unexplained shock Unexplained respiratory failure

4
Step 1: rule out péricardial tamponnade Step 1: rule out péricardial tamponnade

5
LEVEL 1 goal directed

6
Step 2 : evaluation of fluid responsiveness

7
Mean 211 / 195 52 % CHEST 2002, 121:2000-8 R / NRR (%) Calvin (Surgery 81) 20 / 871 % Calvin (Surgery 81) 20 / 871 % Schneider (Am Heart J 88) 13 / 572 % Schneider (Am Heart J 88) 13 / 572 % Reuse (Chest 90) 26 / 1563 % Reuse (Chest 90) 26 / 1563 % Magder (J Crit Care 92) 17 / 1652 % Magder (J Crit Care 92) 17 / 1652 % Diebel (Arch Surgery 92) 13 / 959 % Diebel (Arch Surgery 92) 13 / 959 % Diebel (J Trauma 94) 26 / 3940 % Diebel (J Trauma 94) 26 / 3940 % Wagner (Chest 98) 20 / 1656 % Wagner (Chest 98) 20 / 1656 % Tavernier (Anesthesio 98) 21 / 1460 % Tavernier (Anesthesio 98) 21 / 1460 % Magder (J Crit Care 99) 13 / 1645 % Magder (J Crit Care 99) 13 / 1645 % Tousignant (A Analg 00) 16 / 2440 % Tousignant (A Analg 00) 16 / 2440 % Michard (AJRCCM 00) 16 / 2440 % Michard (AJRCCM 00) 16 / 2440 % Feissel (Chest 01) 10 / 953 % Feissel (Chest 01) 10 / 953 %
 Calvin (Surgery 81) 20 / 871 % Calvin (Surgery 81) 20 / 871 % Schneider (Am Heart J 88) 13 / 572 % Schneider (Am Heart J 88) 13 / 572 % Reuse (Chest 90) 26 / 1563 % Reuse (Chest 90) 26 / 1563 % Magder (J Crit Care 92) 17 / 1652 % Magder (J Crit Care 92) 17 / 1652 % Diebel (Arch Surgery 92) 13 / 959 % Diebel (Arch Surgery 92) 13 / 959 % Diebel (J Trauma 94) 26 / 3940 % Diebel (J Trauma 94) 26 / 3940 % Wagner (Chest 98) 20 / 1656 % Wagner (Chest 98) 20 / 1656 % Tavernier (Anesthesio 98) 21 / 1460 % Tavernier (Anesthesio 98) 21 / 1460 % Magder (J Crit Care 99) 13 / 1645 % Magder (J Crit Care 99) 13 / 1645 % Tousignant (A Analg 00) 16 / 2440 % Tousignant (A Analg 00) 16 / 2440 % Michard (AJRCCM 00) 16 / 2440 % Michard (AJRCCM 00) 16 / 2440 % Feissel (Chest 01) 10 / 953 % Feissel (Chest 01) 10 / 953 %")
8
CVP out…. D Osman Crit care med 2007

9
CVP out…. PAOP out… D Osman Crit care med 2007

10
LEVEL 1

11
TTE : IVC LEVEL 1

12
IVC diameter = 22 % Cardiac output will increase by 18 % after fluid infusion expiration inspiration Feissel Intensive Care Med 2004 “The respiratory variation in inferior vena cava diameter as a guide to fluid therapy” LEVEL 1

13
TTE or TEE : aortic Pulsed Doppler flow Delta peak > 12% Delta VTI > 20% LEVEL 2

14
12%

15
∆Vpeak(%) Before fluid infusion 4 8 12 16 20 24 28 32 36 reponders non reponders Respiratory changes in aortic blood velocity as an indicator of fluid responsiveness in ventilated patients with septic shock. Feissel M, Michard F, Mangin I, Ruyer O, Faller JP, Teboul JL. Chest 2001; 119:867-873

16
-15 0 15 30 45 60 75 5101520253035 r 2 = 0.83 p < 0.001 Respiratory changes in aortic blood velocity as an indicator of fluid responsiveness in ventilated patients with septic shock. Feissel M, Michard F, Mangin I, Ruyer O, Faller JP, Teboul JL. Chest 2001; 119:867-873 Vpeak ( %) before fluid infusion Increase in CO after Fluid infusion (%)
 before fluid infusion Increase in CO after Fluid infusion (%).")
17
Step 3 : evaluation of LV systolic function

18
LV function Ejection fraction Cardiac output Left ventricular filling pressure

19
Shortening Fraction of LV Area Ejection Fraction Systolic Function LEVEL 1

20
NB Shiller, Heart, 1996;75:17-26 Estimated and measured EF LEVEL 1

21
TTE : Ejection fraction Septic shock J1 Septic shock J7

22
Pouleur, Am J Cardiol, 1983;52:813-21 Influence of afterload on EF HT, AS Septic Shock

23
How to perform echocardiographic examination in shocked patient? Cardiac output TTE: LEVEL 2

24
How to perform echocardiographic examination in shocked patient? Cardiac output TTE: LEVEL 2

25
E/E’ ratio predicts PAOP LEVEL 2

26
Combes A Int Care Med 2004 E/Ea ICU, mechanical ventilation LEVEL 2: advanced

27
Step 4 : assessment of right ventricular function

28
No dilatation: RVDA/LVDA< 0.6 Moderate Dilation: RVDA/LVDA 0.6 - 1 Severe dilation: RVDA/LVDA > 1 Jardin Chest 1997 DILATION VD LEVEL 1

29
RV function TAPSETDI LEVEL 2

30
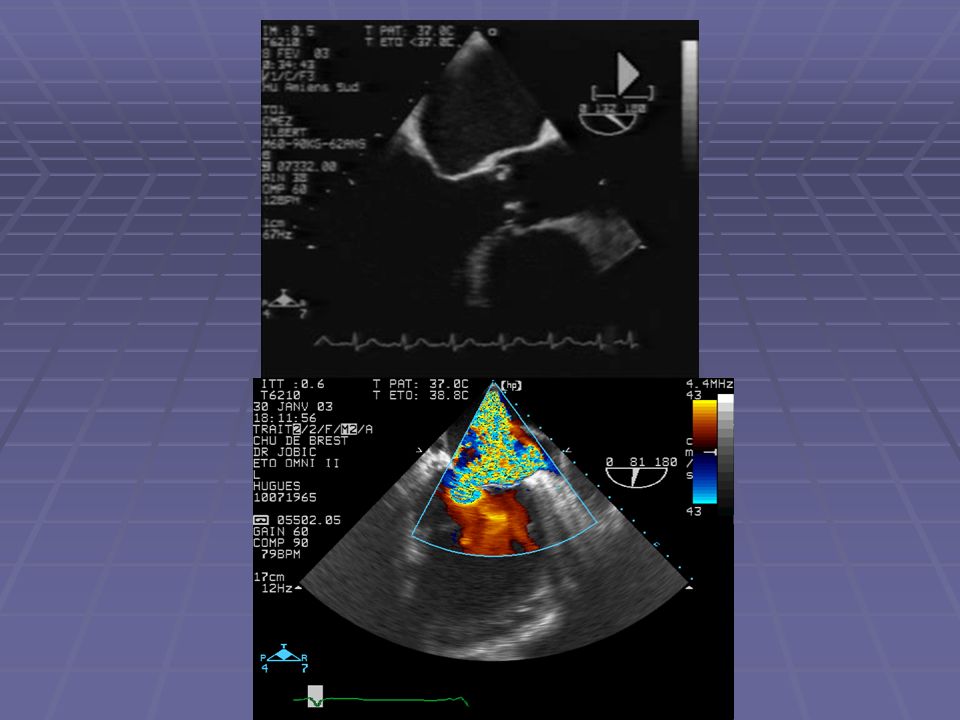
Evaluation of pulmonary arterial pressures Tricuspid regurgitation Pulmonary regurgitation LEVEL 2

31
Septic Shock

32
Cardiac failure? No Acute circulatory failure Yes No Consider circulatory assistance Yes LVRV Fluid responsiveness? Fluid loading Vasopressors InotropesVasopressors* Figure 5.1-2 * LEVEL 1

33
Cardiogenic shock with pulmonary edema

34
Yes Acute circulatory failure & pulmonary venous congestion (elevated LV filling pressures) No LV systolic dysfunction? LV volume overload Extensive (anterior) AMI Mechanical complications Small AMI on previously compromised LV function Cardiogenic shock Acute myocardial infarction (AMI)? NoYes Non ischemic cardiomyopathy Fulminant myocarditis Myocardial contusion, intoxication by cardiac depressant drugs… Acute (severe) valvular regurgitation Valvular prosthesis dysfunction Volume overload (renal failure) LEVEL 1
 AMI Mechanical complications Small AMI on previously compromised LV function Cardiogenic shock Acute myocardial infarction (AMI). NoYes Non ischemic cardiomyopathy Fulminant myocarditis Myocardial contusion, intoxication by cardiac depressant drugs… Acute (severe) valvular regurgitation Valvular prosthesis dysfunction Volume overload (renal failure) LEVEL 1.")
35
Yes Acute circulatory failure & pulmonary venous congestion (elevated LV filling pressures) No LV systolic dysfunction? LV volume overload Extensive (anterior) AMI Mechanical complications Small AMI on previously compromised LV function Cardiogenic shock Acute myocardial infarction (AMI)? NoYes Non ischemic cardiomyopathy Fulminant myocarditis Myocardial contusion, intoxication by cardiac depressant drugs… Acute (severe) valvular regurgitation Valvular prosthesis dysfunction Volume overload (renal failure) Figure 5.1-3 LEVEL 1
 AMI Mechanical complications Small AMI on previously compromised LV function Cardiogenic shock Acute myocardial infarction (AMI). NoYes Non ischemic cardiomyopathy Fulminant myocarditis Myocardial contusion, intoxication by cardiac depressant drugs… Acute (severe) valvular regurgitation Valvular prosthesis dysfunction Volume overload (renal failure) Figure LEVEL 1.")
36
Yes Acute circulatory failure & pulmonary venous congestion (elevated LV filling pressures) No LV systolic dysfunction? LV volume overload Extensive (anterior) AMI Mechanical complications Small AMI on previously compromised LV function Cardiogenic shock Acute myocardial infarction (AMI)? NoYes Non ischemic cardiomyopathy Fulminant myocarditis Myocardial contusion, intoxication by cardiac depressant drugs… Acute (severe) valvular regurgitation Valvular prosthesis dysfunction Volume overload (renal failure) Figure 5.1-3 LEVEL 1
 AMI Mechanical complications Small AMI on previously compromised LV function Cardiogenic shock Acute myocardial infarction (AMI). NoYes Non ischemic cardiomyopathy Fulminant myocarditis Myocardial contusion, intoxication by cardiac depressant drugs… Acute (severe) valvular regurgitation Valvular prosthesis dysfunction Volume overload (renal failure) Figure LEVEL 1.")
37
Acute circulatory failure & systemic venous congestion (elevated RV filling pressures) RV dysfunction / dilatation Cardiac tamponade Relevant pulmonary hypertension? Yes*No Acute RV infarctionMassive pulmonary embolism ARDS Biventricular dysfunction (end-stage cardiomyopathy)** Figure 5.1-4 LEVEL 1
** Figure LEVEL 1.")
38
Acute circulatory failure & systemic venous congestion (elevated RV filling pressures) RV dysfunction / dilatation Cardiac tamponade Relevant pulmonary hypertension? Yes*No Acute RV infarctionMassive pulmonary embolism ARDS Biventricular dysfunction (end-stage cardiomyopathy)** Figure 5.1-4 LEVEL 1
** Figure LEVEL 1.")
39
How to use echocardiography in ICU patients Two clinical situations Unexplained shock Unexplained respiratory failure

40
Respiratory failure Two differents clinical situations : Respiratory distress with pulmonary edema : problem is to distinghish hemodynamic pulmonary edema and ARDS or bilateral pneumonia Severe hypoxemia without pulmonary edema: COPD, PE or intra cardiac or pulmonary shunt « White chest X-ray » « Black chest X-ray »

41
Pulmonary edema? Question 1: is the pulmonary wedge pressure high? Question 2: which is the cause of this pulmonary edema?

42
Pulmonary edema? Question 1: is the pulmonary wedge pressure high?

43
PAOP is pressure into a large pulmonary vein PAOP Pulmonary artery Pulmonary Vein capillairiEscapillairiEsPAOP

44
Non invasive PAOP?

45
Mitral flow Parameters that evaluate LV relaxation preload independent E/Ea ratio LEVEL 2: advanced

46
Combes A Int Care Med 2004 E/Ea ICU, mechanical ventilation LEVEL 2: advanced

47
Pulmonary edema? Question 2: which is the cause of this pulmonary edema?

48
Evaluation of systolic function

49
Cause of pulmonary edema Left ventricular systolic function NormalDecreased Diastolic dysfunction Valvular regurgitation or stenosis

50
Pulmonary edema Left ventricular volume (ml) End diastolic left ventricular pressure (mmHg)
 End diastolic left ventricular pressure (mmHg)")
52
Cause of pulmonary edema Left ventricular systolic function NormalDecreased Diastolic dysfunction Valvular regurgitation or stenosis Ischemic or non ischemic cardiomyopathy

55
Pulmonary edema and normal PAOP : ARDS bilateral pneumoniae

56
Respiratory failure Two differents clinical situation : Respiratory distress syndrom with pulmonary edema : problem is to distinghish between hemodynamic pulmonary edema and ARDS Severe hypoxemia without pulmonary edema: COPD (other) or PE or intra cardiac or pulmonary shunt
 or PE or intra cardiac or pulmonary shunt")
57
Pulmonary embolism Echocardiography : ACP with RV dilation, paradoxical septum mouvement and PAH. Venous Doppler CT Scan

58
Intra pulmonary shunt and Patent foramen ovale

60
Respiratory failure with pulmonary edema PAOP ElevatedNormal LV systolic dysfunctionNormal systolic functionARDS, pneumonia Valvular pathology Diastolic dysfunction Ischemic CM Non ischemic CM

61
Respiratory failure without pulmonary edema Contrast PositiveNegative PFOIntra pulmonary shuntPulmonary cause (COPD)
")
62
Case presentation

Similar presentations






 Occurs when the right ventricle fails as an effective forward pump, causing back-pressure of blood into the systemic.>")












