Download presentation
Presentation is loading. Please wait.

2
THERAPEUTIC MODALITIES LOCAL TREATMENTS SURGERY RADIATION THERAPY SYSTEMIC TREATMENTS CHEMOTHERAPY BIOLOGIC THERAPY

3
DRUG SELECTION SINGLE DRUG COMBINATION THERAPY ADJUVANT CHEMOTHERAPY

4
OUTLINE I.The Cell Cycle II.Categories of Drugs III.Biologic Characteristics of Cancer Cells IV.Mechanisms of Drug Resistance V.Clinical Uses of Cytotoxic Agents VI.Timing and Response to Chemotherapy VII.Chemotherapeutic Agents

5
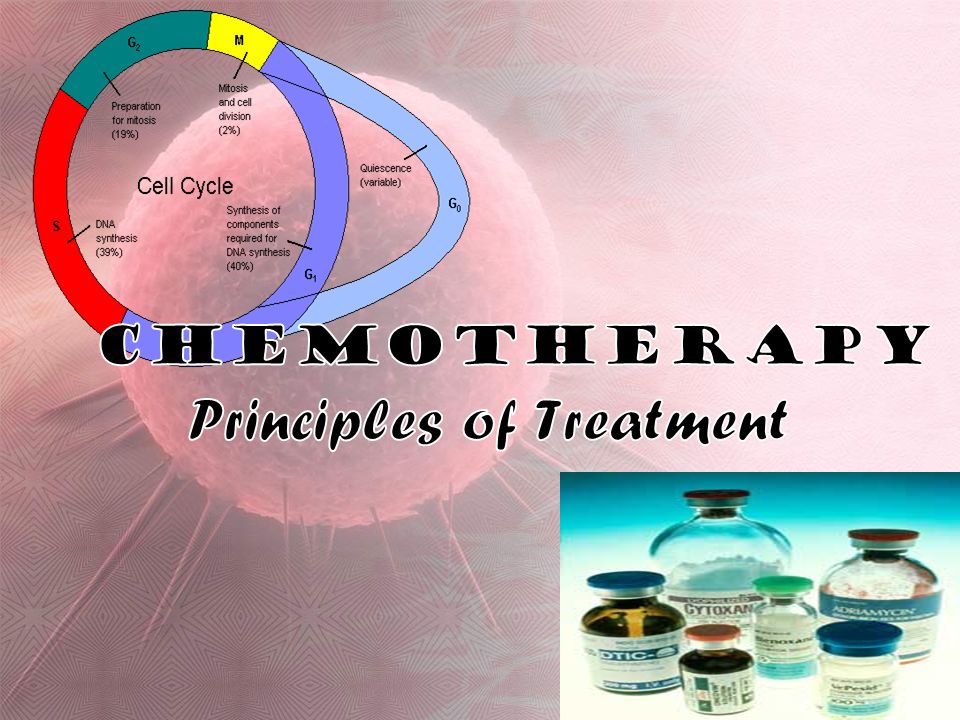
CELL CYCLE

6
PHASES STATEPHASEDESCRIPTION Quiescent/ senescent Gap 0 (G 0 )Resting phase; the cell left the cycle; Stopped dividing. InterphaseGap 1 (G 1 )Cells increase in size G 1 checkpointG 1 checkpoint control mechanism ensures everything ready for DNA synthesis.DNA Synthesis (S)DNA replicationDNA replication occurs. Gap 2 (G 2 )The cell continues to grow. G 2 checkpointG 2 checkpoint control mechanism ensures everything ready to enter the M phase and divide. Cell DivisionMitosis (M)Cell growth stops, cellular energy focused on the orderly division into two daughter cells. Metaphase CheckpointMetaphase Checkpoint ensures the cell ready to complete cell division.
Cells increase in size G 1 checkpointG 1 checkpoint control mechanism ensures everything ready for DNA synthesis.DNA Synthesis (S)DNA replicationDNA replication occurs. Gap 2 (G 2 )The cell continues to grow. G 2 checkpointG 2 checkpoint control mechanism ensures everything ready to enter the M phase and divide. Cell DivisionMitosis (M)Cell growth stops, cellular energy focused on the orderly division into two daughter cells. Metaphase CheckpointMetaphase Checkpoint ensures the cell ready to complete cell division..")
7
Categories of Drugs 1. Phase nonspecific a. Cycle-nonspecific drugs - nondividing cells (steroid hormones, antitumor antibiotics except bleomycin). b. Cycle-specific, phase-nonspecific drugs – effective if cells proceed through the cycle can inflict injury at any point in the cycle (alkylating agents).
. b. Cycle-specific, phase-nonspecific drugs – effective if cells proceed through the cycle can inflict injury at any point in the cycle (alkylating agents)..")
8
Phase Nonspecific Drugs Pharmacokinetics Linear dose–response curve: the greater the amount of drug administered, the greater the fraction of cells killed. Log-cellnumber(response) dose
 dose.")
9
Categories of Drugs 2.Phase specific Cycle-specific, phase-specific drugs are effective only if present during a particular phase of the cell cycle.

10
Cell Cycle & Phase Specific Drugs G0 phase: glucocorticoids for mature lymphocytes G1 phase: L-Asparaginase S phase: procarbazine and antimetabolites G2 phase: bleomycin and plant alkaloids M phase: plant alkaloids

11
Phase Specific Drugs Pharmacokinetics Phase-specific drugs reach a limit in cell-killing ability, but its effect is a function of both time and concentration. (maintaining a drug conc’n over a period of time, more cells enter specific lethal phase of the cycle and killed. Log-cell number dosage

13
Biologic Characteristics of Cancer Cells and Possible use of Chemotherapy Biologic characteristics of cancer cells can be exploited to make them susceptible to drugs. Although malignant cellular proliferation occur in absence of normal growth controls, cancer cells depend on same mechanisms for cell division found in normal cells. Damage to those mechanisms leads to cell death in both normal and malignant tissues.

14
Biologic Characteristics of Cancer Cells and Possible use of Chemotherapy Exploitation of apoptosis in cancer (Radiation and most cytotoxic agents kill cancer cells by damaging cell and inducing apoptosis.) Exploitation of proliferation control factors in cancer. (Biologic response modifiers stimulate selected immune cells, which then demonstrate anticancer activity [interferons, ILs, and GFs.] Exploitation of maturation abnormalities. Maturation factors ( Transretinoic acid, Vit. D, Cytosine arabinoside )/ Eradication of stem cells leaving behind a pop’n of maturing cells.
/ Eradication of stem cells leaving behind a pop’n of maturing cells..")
15
Biologic Characteristics of Cancer Cells and Possible use of Chemotherapy Angiogenesis inhibition: exploitation of dependence of cancer cells to induce the formation of their own blood supply to proliferate. Angiogenesis inhibition is being actively pursued as a tool for cancer treatment.

16
Mechanisms of drug resistance Tumor cell heterogeneity Spontaneous genetic mutations/ drug-resistant Goldie-Coldman hypothesis indicates that probability of a tumor population containing resistant cells is a fxn of total # of cells present. Single-drug resistance (Catabolic enzymes, transport proteins. Multidrug resistance. (P-170 and the mdr-1 gene, loss of apoptosis)
.")
17
Indications for use of Chemotherapy To cure certain malignancies To palliate symptoms in pxs with disseminated cancer when potential benefits of treatment exceed side effects To treat asymptomatic pxs in ff circumstances: a. When cancer is aggressive and treatable (e.g., acute leukemia, small cell lung cancer) b. When treatment proven to decrease rate of relapse and increase disease-free interval or increase absolute survival (colon CA, stages I or II breast CA, Osteogenic sarcoma)
 b. When treatment proven to decrease rate of relapse and increase disease-free interval or increase absolute survival (colon CA, stages I or II breast CA, Osteogenic sarcoma).")
18
Contraindications for use of Chemotherapy 1. Inadequate facilities to evaluate px’s response to therapy & to monitor & manage toxic rxns 2. When px not likely to survive longer even if tumor shrinkage could be accomplished 3. When the px not likely to survive long enough to obtain benefits (severely debilitated patients) 4. When patient is asymptomatic with slow- growing, incurable tumors, in which case chemotherapy should be postponed until symptoms require palliation
 4. When patient is asymptomatic with slow- growing, incurable tumors, in which case chemotherapy should be postponed until symptoms require palliation.")
19
Timing of Chemotherapy A) Induction chemotherapy (initial therapy to achieve significant cytoreduction (complete remission) of disease. B)Consolidation/Intensification chemotherapy (postremission, same drugs used in induction (consolidation) or non-cross resistant drugs (intensification) are repeated. (to prolong remission and overall survival eg. in ALL, AML). C)Adjuvant chemotherapy After local treatment (surgical or radiation), adjuvant used to prevent local or distant relapse.
Consolidation/Intensification chemotherapy (postremission, same drugs used in induction (consolidation) or non-cross resistant drugs (intensification) are repeated. (to prolong remission and overall survival eg. in ALL, AML). C)Adjuvant chemotherapy After local treatment (surgical or radiation), adjuvant used to prevent local or distant relapse..")
20
Timing of Chemotherapy D) Neoadjuvant chemotherapy. Before local therapy, neoadjuvant chemotherapy is given in hopes of reducing extent of local treatment or increasing its effectiveness. E) Maintenance chemotherapy. Prolonged, low- dose outpatient chemotherapy intended to prolong duration of remission and achieve cure in patients in remission. F) Salvage chemotherapy After failure of other treatments (surgery, radiation, or prior chemo), used to control disease or provide palliation.
 Maintenance chemotherapy. Prolonged, low- dose outpatient chemotherapy intended to prolong duration of remission and achieve cure in patients in remission. F) Salvage chemotherapy After failure of other treatments (surgery, radiation, or prior chemo), used to control disease or provide palliation..")
21
Response to Chemotherapy Induction Therapy: Complete response (CR) - disappearance of dx on imaging for at least 1 mo. eg in AML, CR defined as <5% blasts in BM, no circulating blasts in blood & no extramedullary dx by day 14 after induction. Partial response (PR) - decrease of 50% or more in sum of products of biperpendicular diameters; no new sites of dx at least 1 month. Stable disease in pxs with <50% response without actual progression of disease. Progression 25% inc in sum of products of biperpendicular diameters of known lesions or any new sites of disease.
 - decrease of 50% or more in sum of products of biperpendicular diameters; no new sites of dx at least 1 month. Stable disease in pxs with <50% response without actual progression of disease. Progression 25% inc in sum of products of biperpendicular diameters of known lesions or any new sites of disease..")
22
Response to Chemotherapy Adjuvant chemotherapy: Relapse-free survival measures time from start of tx to regrowth of tumor to detectable levels. Salvage chemotherapy: Progression-free survival remains major end point in patients with advanced disease and equivalent of relapse-free survival in adjuvant setting.

23
CANCER CHEMOTHERAPY DRUG CLASSSIFICATION

24
Classification of Chemotherapy Drugs CELL-CYCLE SPECIFIC DRUGS Antimetabolites Mitotic Inhibitors (Vinca Alkaloids, Epipodophyllotoxins, Taxanes) Camptothecins CELL-CYCLE NONSPECIFIC DRUGS Alkylating agents Antitumor antibiotics Hormones Hormone Antagonists Miscellaneous Agents
 Camptothecins CELL-CYCLE NONSPECIFIC DRUGS Alkylating agents Antitumor antibiotics Hormones Hormone Antagonists Miscellaneous Agents")
25
Cell Cycle-Specific Agents Administered in divided doses or as a continuous infusion which facilitates lysis of cells in certain phases of the cycle. Reduce growth fraction (# of cells present in the cycle) of the tumor.
 of the tumor..")
26
Antimetabolites Structural analogues of normal molecules essential for cell growth and replication. inhibit enzymes necessary for synthesis. major effect - interfering with building blocks of DNA synthesis activity greatest in S phase of cell cycle most effective when cell proliferation is rapid. Nonlinear dose-response curve (except FU). eg ( Capecitabine, 5-FU, Cytosine arabinoside, Gemcitabine, Deoxycoformycin, 6-Mercaptopurine, Floxuridine, Methotrexate, Fludarabine, Thioguanine
. eg ( Capecitabine, 5-FU, Cytosine arabinoside, Gemcitabine, Deoxycoformycin, 6-Mercaptopurine, Floxuridine, Methotrexate, Fludarabine, Thioguanine.")
27
Methotrexate (amethopterin, MTX) I: A wide variety of conditions MOA: Folic acid antimetabolite. blocks dihydrofolate reductase, preventing formation of reduced tetrahydrofolic acid; block formation of thymidylate from deoxyuridylate & prevents synthesis of DNA; also inhibits RNA and protein synthesis prevents cells from entering S phase. Metab: min metabolized; excreted in urine unchanged (90%) Toxicity (reversed with Leucovorin 1:1) Dose limiting. Myelosuppression, stomatitis, renal dysfxn High-dose regimens. N/V, RT necrosis, cortical blindness Dose: 2.5-mg tablets and 20 to 1000-mg vials. Modification. must not be given to px w/ CrCl <60mL/min
 Toxicity (reversed with Leucovorin 1:1) Dose limiting. Myelosuppression, stomatitis, renal dysfxn High-dose regimens. N/V, RT necrosis, cortical blindness Dose: 2.5-mg tablets and 20 to 1000-mg vials. Modification. must not be given to px w/ CrCl <60mL/min.")
28
Mercaptopurine (6-MP, Purinethol) I: ALL (maintenance therapy) MOA: Purine antimetabolite. Undergoes extensive metabolic changes; complex Inhibits de novo purine synthesis, purine interconversion Competes with ribotides for enzymes responsible for conversion of inosinic acid to adenine and xanthine ribotides. Metab: slowly degraded in liver, largely by xanthine oxidase. Toxicity Dose limiting. Myelosuppression Common. N/V, anorexia (25%); reversible cholestasis Dose: Supplied as 50-mg tablets, 70 to 100mg/m2 Modification. Reduced by 50-75% for pxs w/ hepatic dysfxn.
; reversible cholestasis Dose: Supplied as 50-mg tablets, 70 to 100mg/m2 Modification. Reduced by 50-75% for pxs w/ hepatic dysfxn..")
29
Fluorouracil (5-FU, Adrucil) I: A wide variety of carcinomas MOA: Pyrimidine Antimetabolite Interferes with DNA synthesis by blocking thymidylate synthetase, (conversion of deoxyuridylic acid to thymidylic a) Incorporated into several RNA species, interfere with RNA fxn and protein synthesis. S-phase specific but acts in other cell cycle phases Unique in having a log linear cell-killing action. Metab: hepatic; 90% excreted in urine, bile & breath (CO2). Toxicity: Dose limiting Myelosuppression, mucositis/diarrhea Common: Nasal discharge; eye irritation and lacrimation Dose: 500-mg vials Modification: w/held if px has diarrhea, infection, leukopenia,
. Toxicity: Dose limiting Myelosuppression, mucositis/diarrhea Common: Nasal discharge; eye irritation and lacrimation Dose: 500-mg vials Modification: w/held if px has diarrhea, infection, leukopenia,.")
30
Leucovorin (citrovorum factor, folinic acid, 5-formyl tetra-hydrofolate) I: Combined w/ 5-FU in tx of colorectal & other adenoCAs; rescue agent for antifol toxicity (MTX) MOA: a tetrahydrofolic acid derivative that acts as a cofactor for carbon transfer rxns in synthesis of purines & pyrimidines Inhibits effects of MTX & other DHFR antagonists. Metabolism. Excreted in the urine as metabolites Toxicity. Potentiates toxic effects of fluoropyrimidine therapy Dose: 50-, 100-, and 350-mg vials for IV use and as a 60-mg bottle for oral use

31
Mitotic Inhibitors Mitotic inhibitors interfere with formation of mitotic spindle, causing metaphase arrest. M-phase active, but they may also have activity in G2 and S. Include the vinca alkaloids, the epipodophyllo- toxins, and the taxanes.

32
Vinca Alkaloids A.k.a plant alkaloids - extracts of periwinkle plant. bind to microtubular proteins, essential in forming mitotic spindle of the dividing cells. This binding arrests mitosis, which eventually causes cell death. act mainly in M phase; however, high doses can also disrupt RNA and protein synthesis. Vinblastine, Vincristine, Vindesine, Vinorelbine

33
Vinblastine (Velban) I: Lymphomas, testicular carcinoma MOA: Binds to microtubular proteins. Inhibits RNA synthesis by affecting DNA-dependent RNA polymerases. Cell cycle–phase specific; arrests cells at the G2-phase and M-phase interface. Metab: mainly hepatic, minimal renal Toxicity: Dose-limiting Neutropenia Common Cramps or severe jaw, back pain Dose: 10-mg vials Dose modification. Decrease dose by 50% for patients with serum bilirubin greater than 3.0 mg/dL.

34
Vincristine (Oncovin/Vincasar/leurocristine) I: A wide variety of malignancies MOA: Same as vinblastine Metabolism. Same as vinblastine Toxicity Dose-limiting. Severe paresthesias, ataxia, Foot drop (slapping gait), muscle wasting, cranial nerve palsies, paralytic ileus, obstipation, abdominal pain, cortical blindness, seizures Common. Tissue necrosis, alopecia (20% to 40%) Dose: 1 mg/mL vials Modification. Hepatic dysfunction; same as for vinblastine
, muscle wasting, cranial nerve palsies, paralytic ileus, obstipation, abdominal pain, cortical blindness, seizures Common. Tissue necrosis, alopecia (20% to 40%) Dose: 1 mg/mL vials Modification. Hepatic dysfunction; same as for vinblastine.")
35
Epipodophyllotoxins isolated from the mandrake plant (May crab apple). act in the premitotic phase, G2 and S, and interfere with topoisomerase II enzyme reaction. Inhibition of topoisomerase interferes with transcription and replication by causing DNA damage, inhibition of DNA replication, failure to repair strand breaks, and then, cell death. Etoposide, Teniposide

36
Etoposide (VP-16, VePesid) I: Testicular CA, Lung CA, lymphoma, & other malignancies MOA: An epipodophyllotoxin; a topoisomerase II inhibitor cell cycle–phase specific at G2, late S, and M phases. Metab: Highly bound to plasma proteins; metabolized by the liver. Excreted in urine (40%) intact & degraded drug; excretion of remaining 60% is uncertain. Toxicity Dose-limiting: Neutropenia Common. N/V (w/ oral dosing); mild alopecia ; hypotension if rapidly infused Dose: 50 mg/m2 PO daily for 21 days/ 50 to 120 mg/m2 IV daily for 3 to 5 days DI. CCBs, methotrexate may increase cytotoxicity
 intact & degraded drug; excretion of remaining 60% is uncertain. Toxicity Dose-limiting: Neutropenia Common. N/V (w/ oral dosing); mild alopecia ; hypotension if rapidly infused Dose: 50 mg/m2 PO daily for 21 days/ 50 to 120 mg/m2 IV daily for 3 to 5 days DI. CCBs, methotrexate may increase cytotoxicity.")
37
Taxanes Taxanes cause mitotic arrest by forming abnormal spindle fibers and mitotic asters. Taxanes not only bind to microtubules but also promote microtubule assembly and resistance to depolymerization, resulting in production of nonfunctional microtubules. Docetaxel, Paclitaxel

38
Paclitaxel (Taxol) I: Breast, ovarian CA, AIDS-assoc Kaposi’s sarcoma, others MOA: Taxane ; bind to microtubules and promote microtubule assembly & resistance to depolymerization, resulting in production of nonfunctional microtubules. Metab: Nearly totally protein bound & distributed well to body fluids (effusions) w/ a plasma half-life of about 5 hours Toxicity Dose-limiting: Neutropenia, prev. treated w/ cisplatin Hypersensitivity, Peripheral neuropathy. Common: Alopecia, thrombocytopenia; transient arthralgias & myalgias w/in 3 days of tx (ameliorated by NSAIDs), brady Dose: 30-, 100-, and 300-mg vials/ 135 to 175mg/m2 Dose modification. Hematologic
 w/ a plasma half-life of about 5 hours Toxicity Dose-limiting: Neutropenia, prev. treated w/ cisplatin Hypersensitivity, Peripheral neuropathy. Common: Alopecia, thrombocytopenia; transient arthralgias & myalgias w/in 3 days of tx (ameliorated by NSAIDs), brady Dose: 30-, 100-, and 300-mg vials/ 135 to 175mg/m2 Dose modification. Hematologic.")
39
Camptothecins Name derived from the Chinese tree Camptotheca acuminata new subcategory of cell cycle–specific drugs. act in S phase and inhibit topoisomerase I, a nuclear enzyme necessary for maintaining DNA structure, resulting in single-stranded DNA breaks and subsequently cell death. Irinotecan, Topotecan

40
Irinotecan (Camptosar, CPT-11) I: Colorectal CA refractory to 5-FU–based chemotherapy MOA: water-soluble analogue of camptothecin, relatively inactive prodrug, converted to active agent Inhibits topoisomerase I cell cycle– phase specific. Metab. Metabolized in liver. Renal clearance. Toxicity Dose-limiting. Profuse diarrhea Common. Neutropenia; mild N/V, abdominal cramps; flushing during administration; alopecia Dose: 100-mg vials/ 125mg/m2 Dose modification. Use with caution for hepatic insufficiency.

41
Cycle-Nonspecific Drugs Effective through all phases of cell cycle Directly affect DNA molecule and display no specificity for cells that are dividing. More toxic than cycle–specific drugs (does not differentiate between normal & malignant cells. Given in bolus doses because they cause death independently of the proliferative state of cell. Reduce the number of cells that make up a tumor, which is known as the tumor burden.

42
Alkylating Agents target DNA, cytotoxic, mutagenic & carcinogenic. All produce alkylation through the formation of intermediates. Impair cell fxn by transferring alkyl groups to amino, carboxyl, sulfhydryl, or phosphate groups of important mol. nucleic acids & proteins alkylated. (N-7) position of guanine in DNA & RNA - most actively alkylated site; O-6 grp of guanine alkylated by nitrosoureas. Alkylation of guanine results in abnormal nucleotide sequences, miscoding of messenger RNA, cross-linked DNA strands that cannot replicate, breakage of strands, and other damage to transcription & translation of genetic mat’l. Primary mode of action: cross-linking of DNA strands.
 position of guanine in DNA & RNA - most actively alkylated site; O-6 grp of guanine alkylated by nitrosoureas. Alkylation of guanine results in abnormal nucleotide sequences, miscoding of messenger RNA, cross-linked DNA strands that cannot replicate, breakage of strands, and other damage to transcription & translation of genetic mat’l. Primary mode of action: cross-linking of DNA strands..")
43
Alkylating Agents Mustard gas derivatives: Mechlorethamine, Cyclophosphamide, Chlorambucil, Melphalan,& Ifosfamide. Ethylenimines: Thiotepa & Hexamethylmelamine. Alkylsulfonates: Busulfan. Hydrazines and Triazines: Altretamine, Procarbazine, Dacarbazine and Temozolomide. Nitrosureas: Carmustine, Lomustine and Streptozocin (unique, can cross BBB). Metal salts: Carboplatin, Cisplatin, and Oxaliplatin.
. Metal salts: Carboplatin, Cisplatin, and Oxaliplatin..")
44
Cyclophosphamide (Cytoxan) I: Used in a wide variety of conditions MOA: Alkylation, also inhibits DNA synthesis Metab: requires activation by liver microsomal oxidase system to form an aldehyde that decomposes in plasma and peripheral tissues to yield acrolein & an alkylating metabolite (phosphoramide mustard); excreted in urine. Toxicity: Dose limiting: Myelosuppression, hemorrhagic Cystitis Common. Alopecia, stomatitis, aspermia, amenorrhea; headache (fast onset, short duration), N/V. Dose: 25 or 50mg tabs; vials contain 100 to 1000 mg Dose modification. Hematologic; may be required for hepatic functional impairment
, N/V. Dose: 25 or 50mg tabs; vials contain 100 to 1000 mg Dose modification. Hematologic; may be required for hepatic functional impairment.")
45
Busulfan (Myleran) I: CML, bone marrow transplantation (high doses) MOA: Alkylation Metabolism: Acts directly; catabolized to inactive products excreted in the urine. Toxicity Dose limiting. Reversible and irreversible myelosuppression with slow recovery; blood cell counts fall for about 2 weeks after discontinuation of drug. Common. GI upset (mild), sterility Dose: 2-mg tablets/ 2-8mg/day PO Dose modification. Hematologic
, sterility Dose: 2-mg tablets/ 2-8mg/day PO Dose modification. Hematologic.")
46
Procarbazine (Matulane, Natulan, N- methylhydrazine) I: Hodgkin & Non-Hodgkin Lymphoma, Myeloma, Brain Ca MOA: DNA alkylation and depolymerization; Methylation of nucleic acids; Inhibition of DNA, RNA, and protein synthesis Metab: Metabolic activation required. Readily enters CSF. Degraded in liver to inactive cmpds, excreted in urine Toxicity: Dose limiting. Myelosuppression, which may not begin until several weeks after starting treatment Common. N/V, which decreases w/ continued use; myalgia, arthralgia; sensitizes tissues to radiation Dose: 50-mg capsules Modification Reduce dose in pxs w/ hepatic, renal, or bone marrow dysfunction.

47
Streptozocin (streptozotocin, Zanosar) I: Islet cell CA (w/ FU), carcinoid syndrome MOA: Alkylation; Inhibits DNA synthesis & DNA repair enzyme, guanine-O6-methyl transferase; affects pyrimidine nucleotide metab, inhibits enzymes in gluconeogenesis Metab: extensively metabolized, a short plasma half-life; Crosses BBB; Excreted in urine. Toxicity Dose limiting: Nephrotoxicity Common: N/V, myelosuppression, hypoglycemia, vein irritation Dose: 1-g vials/ 1.0 g/m2 IV weekly, or 0.5 g/m2 IV daily Modification. Proteinuria or elevated serum creatinine levels

48
Cisplatin (cis-diaminedichloroplatinum [CDDP], Platinol) I: A wide variety of malignancies MOA: heavy metal alkylator of DNA; Covalently bonds to proteins, RNA, & esp DNA, forming DNA cross-linking & intrastrand N-7 adducts. Metab: Widely distributed in body, except for CNS. Long half-life in plasma (3 days); drug (30%) & metabolites excreted in urine; biliary excretion <10% Toxicity Dose limiting: Cumulative renal insufficiency/ Peripheral sensory neuropathy, Ototoxicity with tinnitus Common: Severe N/V, hypokalemia, hypomagnesemia & mild myelosuppressiona. Dose: 10- and 50-mg vials/ 40 to 120mg Mod: Renal fxn must return to normal before cisplatin given
![Cisplatin (cis-diaminedichloroplatinum [CDDP], Platinol) I: A wide variety of malignancies MOA: heavy metal alkylator of DNA; Covalently bonds to proteins, RNA, & esp DNA, forming DNA cross-linking & intrastrand N-7 adducts.](http://images.slideplayer.com/25/8167374/slides/slide_48.jpg "Metab: Widely distributed in body, except for CNS. Long half-life in plasma (3 days); drug (30%) & metabolites excreted in urine; biliary excretion <10% Toxicity Dose limiting: Cumulative renal insufficiency/ Peripheral sensory neuropathy, Ototoxicity with tinnitus Common: Severe N/V, hypokalemia, hypomagnesemia & mild myelosuppressiona. Dose: 10- and 50-mg vials/ 40 to 120mg Mod: Renal fxn must return to normal before cisplatin given.")
49
Antitumor Antibiotics Isolated from fermented broths ofStreptomyces Focal point of cytotoxicity is the DNA. Interfere w/ DNA-directed RNA synthesis by intercalating between base pairs of DNA and generating toxic oxygen-free radicals, causing single- or double-stranded DNA breaks. cycle–nonspecific, useful in slow-growing tumors with low growth fractions. Anthracyclines: Doxorubicin, Daunorubicin, Epirubicin, Mitoxantrone, and Idarubicin. Chromomycins: Dactinomycin and Plicamycin. Miscellaneous: Mitomycin and Bleomycin.

50
Actinomycin D (dactinomycin, Cosmegen) I: Trophoblastic neoplasms, sarcomas, testicular CA, Wilms’ MOA: Intercalates between DNA base pairs & prevents synthesis of mRNA; inhibits topoisomerase II Metab: Unknown; extensively bound to tissues, resulting in long half-life in plasma & tissue, Excreted in bile and urine Toxicity Dose limiting. Myelosuppression Common. N/V (worsening after successive daily doses); alopecia, acne, erythema, desquamation,hyperpigmentation; radiation-recall rxn; a vesicant that causes necrosis Dose: 0.5-mg vials/ 0.25 to 0.60 mg/m2 IV daily for 5 days Modification. Reduce by 50% in of renal or hepatic dysfxn.
; alopecia, acne, erythema, desquamation,hyperpigmentation; radiation-recall rxn; a vesicant that causes necrosis Dose: 0.5-mg vials/ 0.25 to 0.60 mg/m2 IV daily for 5 days Modification. Reduce by 50% in of renal or hepatic dysfxn..")
51
Bleomycin (Blenoxane) I: Lymphoma, SCC, testicular Ca, malignant effusions others MOA: Binds to DNA, inhibiting synthesis of DNA, RNA and Proteins; Causes DNA strand cleavage by free radicals and inhibits DNA repair by marked inhibition of DNA ligase. G2-phase specific; also active in late G1, S, and M phases Metab: tissue-bound, extensive degradation by hydrolysis in nearly all tissues. Drug & metab products excreted in urine. Toxicity Dose-limiting: Mild -severe shaking chills & febrile rxns, Bleomycin pneumonitis w/ dyspnea, dry cough Common Sensitizes tumor & tissues to radiation, anorexia hyperpigmentation of skin stretch areas, mucositisa. Dose: 15-unit (mg) vials Modification. COPD, erythroderma
 vials Modification. COPD, erythroderma.")
52
Doxorubicin ( Adriamycin/Rubex/hydroxydaunorubicin) I: Effective in a large variety of tumors MOA: Anthracycline; Intercalates b/w DNA base pairs, forms free radicals, alters cell membranes, induces topoisomerase II–dependent DNA damage, inhibits preribosomal DNA and RNA. Cycle–phase nonspecific. Metab: 70% bound to plasma proteins; metabolized by liver excreted in the bile Toxicity Dose-limiting: Myelosuppression, Cardiomyopathy Common: Alopecia, N/V; stomatitis, ulceration & necrosis. Dose: 10, 20, 50, 100 & 150mg vials/ 50-75 mg/m2 IV bolus Modification. congestive heart failure,

53
Hormones & Hormone Antagonists diverse group of drugs beneficial in cancer therapy. Some alter cellular environment & affect permeability of cell membrane that will affect cell growth. inhibit tumor proliferation by blocking/ antagonizing naturally occurring substance that stimulates tumor growth. Androgens: testosterone proprionate, methyltestosterone, fluoxymesterone Antiandrogens: flutamide Antiestrogens: tamoxifen Aromatase inhibitors: aminoglutethimide Estrogens: diethylstilbestrol, estradiol Glucocorticoids: prednisone, hydrocortisone, dexamethasone Gonadotropin inhibitors: leuprolide, goserelin Progestins: megestrol acetate

54
Hormones & Hormone Antagonists Androgens I: Breast Ca, short-range anabolic, erythropoiesis stimulant Toxicity & SE vary; Virilization, fluid retention & hepatotoxic, characterized by abnormal LFTs or cholestasis reversible, Antiandrogens (bicalutamide, flutamide, nilutamide) I: Prostate Ca in combination with medical therapy MOA: Nonsteroidal antiandrogens bind to cytosol androgen receptors & competitively inhibit uptake or binding Toxicity Common Impotence, gynecomastia, hypogonadism Antiestrogens (tamoxifen, toremifene) I: Breast carcinoma MOA: Nonsteroidal agents that bind to estrogen receptors, exert antiestrogenic, estrogenic, or both activities 3
 I: Prostate Ca in combination with medical therapy MOA: Nonsteroidal antiandrogens bind to cytosol androgen receptors & competitively inhibit uptake or binding Toxicity Common Impotence, gynecomastia, hypogonadism Antiestrogens (tamoxifen, toremifene) I: Breast carcinoma MOA: Nonsteroidal agents that bind to estrogen receptors, exert antiestrogenic, estrogenic, or both activities 3")
55
Miscellaneous BIOLOGICAL RESPONSE MODIFIERS –Interferon-alfa, Interleukin-2 TYROSINE KINASE INHIBITORS –Imatinib (Glivec): CML MONOCLONAL ANTIBODIES –Versus GROWTH FACTOR RECEPTORS Rituximab (NHL,CLL), Trastuzumab (metastatic breast CA) –Versus ANGIOGENIC FACTORS Bevacizumab (coloretal CA, renal cell CA)
: CML MONOCLONAL ANTIBODIES –Versus GROWTH FACTOR RECEPTORS Rituximab (NHL,CLL), Trastuzumab (metastatic breast CA) –Versus ANGIOGENIC FACTORS Bevacizumab (coloretal CA, renal cell CA)")
56
Interferon-a (IFN-a) Sources: Lymphocytes, macrophages, and other cells Properties: Antitumor activity, Antiproliferative activity, Inhibition of angiogenesis, Reg’n of differentiation,Interaction w/ growth factors, oncogenes, other cytokine, enhancement of tumor-associated antigens; NK cell activation, CTL activation, induction of (MHC) class I, Antiviral activity I: CML, hairy cell leukemia, myeloproliferative disorders, cutaneous T-cell lymphomas D: recombinant forms (IFN-a2a (Roferon-A): 3, 6, 18, & 36million U/mL vials/ IFN-a2b (Intron-A): 3, 5, 18, & 50million U/mL vials
 Sources: Lymphocytes, macrophages, and other cells Properties: Antitumor activity, Antiproliferative activity, Inhibition of angiogenesis, Reg’n of differentiation,Interaction w/ growth factors, oncogenes, other cytokine, enhancement of tumor-associated antigens; NK cell activation, CTL activation, induction of (MHC) class I, Antiviral activity I: CML, hairy cell leukemia, myeloproliferative disorders, cutaneous T-cell lymphomas D: recombinant forms (IFN-a2a (Roferon-A): 3, 6, 18, & 36million U/mL vials/ IFN-a2b (Intron-A): 3, 5, 18, & 50million U/mL vials")
57
Rituximab (Rituxan) I: Relapsed or refractory low-grade or follicular CD20-(+), B- cell non-Hodgkin lymphoma MOA: antibody is a genetically engineered chimeric murine/ human monoclonal antibody directed against CD20 antigen found on the surface of normal and malignant B lymphocytes. In vitro, Fab domain of rituximab binds to CD20 antigen on B lymphocytes, and Fc domain recruits immune effector functions to mediate B-cell lysis. Metab: detectable in serum 3 to 6 months; admin results in a rapid and sustained depletion of circulating and tissue- based B cells. B-cell levels return to normal by 12 months after completion of treatment. Toxicity: Dose-limiting. Hypersensitivity rxns, arrhythmias Common: infusion-related symptom complex responds to slowing infusion rate and consists of fever or chills (50%);
;.")
58
SAMPLE REGIMENS

59
HODGKIN LYMPHOMA ABVD: Adriamycin (doxorubicin), bleomycin, vinblastine, dacarbazinedoxorubicinbleomycin vinblastinedacarbazine BEACOPP: Bleomycin, etoposide, Adriamycin (doxorubicin), cyclophosphamide, Oncovin (vincristine), procarbazine, prednisoneBleomycinetoposidedoxorubicincyclophosphamidevincristineprocarbazineprednisone MOPP: MechlorethamineMOPP: Mechlorethamine, Oncovin (vincristine), procarbazine, prednisonevincristine procarbazineprednisone ChlVPP/EVA Chlorambucil,vincristine (Oncovin), procarbazine, prednisone, etoposide, vinblastine, Adriamycin (doxorubicin)ChlorambucilOncovinprocarbazineprednisone etoposidevinblastinedoxorubicin
, bleomycin, vinblastine, dacarbazinedoxorubicinbleomycin vinblastinedacarbazine BEACOPP: Bleomycin, etoposide, Adriamycin (doxorubicin), cyclophosphamide, Oncovin (vincristine), procarbazine, prednisoneBleomycinetoposidedoxorubicincyclophosphamidevincristineprocarbazineprednisone MOPP: MechlorethamineMOPP: Mechlorethamine, Oncovin (vincristine), procarbazine, prednisonevincristine procarbazineprednisone ChlVPP/EVA Chlorambucil,vincristine (Oncovin), procarbazine, prednisone, etoposide, vinblastine, Adriamycin (doxorubicin)ChlorambucilOncovinprocarbazineprednisone etoposidevinblastinedoxorubicin")
60
BREAST CA AC: Adriamycin (doxorubicin), cyclophosphamidedoxorubicincyclophosphamide CA: Cyclophosphamide, Adriamycin (doxorubicin) (same as AC)Cyclophosphamidedoxorubicin CAF: Cyclophosphamide, Adriamycin (doxorubicin), fluorouracil (5-FU)Cyclophosphamidedoxorubicinfluorouracil CMF: Cyclophosphamide, methotrexate, fluorouracil (5-FU)CMF: Cyclophosphamidemethotrexate fluorouracil EC: Epirubicin, cyclophosphamideEpirubicincyclophosphamide FEC: Fluorouracil (5-FU), epirubicin, cyclophosphamideFluorouracilepirubicin cyclophosphamide
, cyclophosphamidedoxorubicincyclophosphamide CA: Cyclophosphamide, Adriamycin (doxorubicin) (same as AC)Cyclophosphamidedoxorubicin CAF: Cyclophosphamide, Adriamycin (doxorubicin), fluorouracil (5-FU)Cyclophosphamidedoxorubicinfluorouracil CMF: Cyclophosphamide, methotrexate, fluorouracil (5-FU)CMF: Cyclophosphamidemethotrexate fluorouracil EC: Epirubicin, cyclophosphamideEpirubicincyclophosphamide FEC: Fluorouracil (5-FU), epirubicin, cyclophosphamideFluorouracilepirubicin cyclophosphamide")
61
COLORECTAL CA FOLFOX: Fluorouracil (5-FU), leucovorin (folinic acid), oxaliplatinFluorouracilfolinic acidoxaliplatin FOLFIRI: Fluorouracil (5-FU), leucovorin (folinic acid), irinotecanFluorouracilfolinic acidirinotecan FL: Fluorouracil (5-FU), leucovorin (folinic acid)FL: Fluorouracilfolinic acid
, leucovorin (folinic acid), oxaliplatinFluorouracilfolinic acidoxaliplatin FOLFIRI: Fluorouracil (5-FU), leucovorin (folinic acid), irinotecanFluorouracilfolinic acidirinotecan FL: Fluorouracil (5-FU), leucovorin (folinic acid)FL: Fluorouracilfolinic acid")
62
LUNG CANCER CAV: Cyclophosphamide, Adriamycin (doxorubicin), vincristineCAV: Cyclophosphamidedoxorubicinvincristine
, vincristineCAV: Cyclophosphamidedoxorubicinvincristine")
63
THANK YOU!

Similar presentations




 Carcinoembryonic.>")
. C C ancers most commonly occur in: breast (♀) ->")







 2010,3.>")






