Download presentation
Presentation is loading. Please wait.

1
Documentation By Peter Latham FY2 A&E

2
What we’re going to discuss The basics Clinical Summary, ward rounds, TTOs Post Death Certification TTO Talking and documenting conversations with other specialties

3
Don’t be this Guy

4
Why be a Master of Documentation? Massive help to other specialties reviewing the patient, or on call doctors.

5
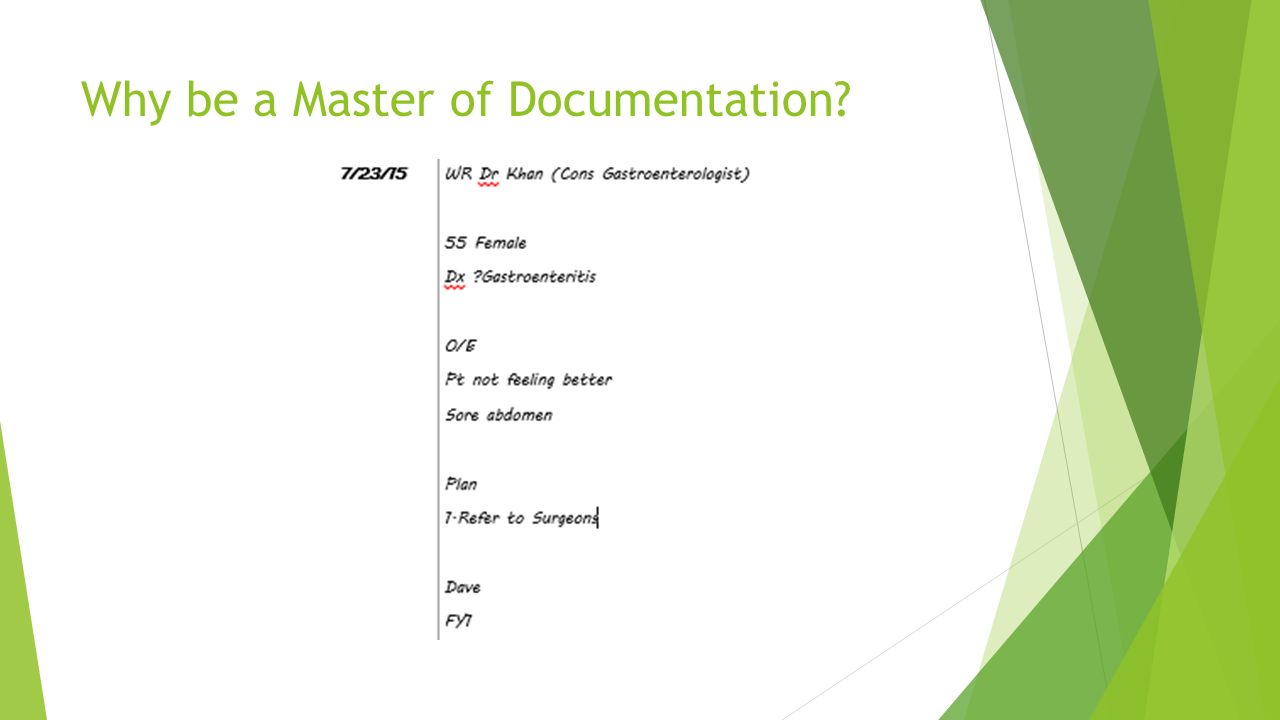
Why be a Master of Documentation?

7
Massive help to other specialties reviewing the patient, or on call doctors. An accurate recording of the patient story Map their journey through the hospital Help identify where things began to improve or decline Legally – it can save your bacon!!

8
Pitfalls of Poor Documentation Lack of Preparation Teamwork – rarely will you be the only junior on the wardround Pre-wardround prep – blood stickers, look up NEWs, print scan reports Surgeons Medical wardrounds start later and have a more gentle pace Surgical wardrounds are 100mph Don’t feel bad asking to repeat things, asking them to hold on, did they find anything on examination, repeat the plan, show them the drug Kardex

9
Targets to think about during the Wardround Positive Outcomes Leaving before 6pm Having a lunch break Having a coffee break Not looking incompetent Gaining some form of respect from the nursing staff Being able to sit down at some point

10
Targets to think about during the Wardround Things that stand in the way of this: Cannulas – ask if we still need IVI, can we switch Abx to oral, are we happy with that UO, NEWS – is that BP OK for the patient, are we concerned about that HR Meds R/V – show them the Kardex, Bloods – do we need to do any more bloods on this pt, are you happy with that trend Referrals – what exactly do we want from the radiologist, surgeons, Med Reg? Family Questions – whats our Imp, ?home tomorrow

11
Basics

12
FY 2 Latham ED SHO Signed 7420531

13
Talking to other Specialities When asked to discuss with another team think about the following things: What clinical question are we asking them? Do we want advice? Do we want them to see the patient? Do we want them to take over the question? Stick to the SBAR system, have all the information you need by the phone. Document the key elements of what was discussed Make sure you get their name and a contact number

14
TTOs Think about it as if you were on the phone, speaking to the GP, telling them all the important events Also think about the next time the patient presents to A&E, what important things need to be documented for the admitting Doctor Tell a succinct patient story

15
TTOs Diagnosis – Type I Respiratory Failure Secondary to Community Acquired Pneumonia Mrs Blogs presented to ED with SOB and a productive cough. She was found to hypotensive, tachycardic and drowsy. An ABG revealed a Type I Respiratory Failure and CxR showed Left lower lobe consolidation. She required Iv Abx and NIV. Sputum Cultures grew S.Pneumoniae. With Abx and chest physio her symptoms improved and she is now medically stable for discharge. Other things to mention – DNARs, thickened fluids, changes to social, recommendations given to patient (DVLA etc)
.")
16
TTOs Investigations Bloods – WCC 22, CRP 208, U&E – NAD CxR – Left lower lobe pneumonia ECG – Left Axis Deviation, SR BCM – S.Pneumoniae (sensitive – Penicillin) CT Thorax – try and fit whole report
 CT Thorax – try and fit whole report")
17
TTOs Procedures Chest Drain – what did it grow Operation – exactly what and was it complicated Endoscopy? Bronchoscopy

18
TTOs Follow-up - what have you organised – CxR on arrival, Echo - what needs organising at booking centre (Check) GP Advise - very busy people - document medication changes, - Recheck bloods - Refer to clinics that you cant - Not just monitor symptoms, unsure patient remains well etc
 GP Advise - very busy people - document medication changes, - Recheck bloods - Refer to clinics that you cant - Not just monitor symptoms, unsure patient remains well etc")
19
TTOs – The Bad Diagnosis – chest infection Pt admitd with cough. Received Abx. Bloods improved, now stable Pmhx Smoker Investigations Bloods

20
TTOs GP Refer to Resp Clinic Get Pt to stop smoking Repeat Bloods next week Meds Co-amox Clarithro GP to review

21
Deaths Sadly you will see a lot of deaths as a junior doctor – it’s a reality of the job Some jobs you will forever find yourself filling out Death Certificated ALWAYS, ALWAYS, ALWAYS, ask the consultant SPECIFICALLY what they want as 1a, b, c. I recommend asking them as soon as you find out about the death, and double check whilst in the bereavement office Do they need to be referred to the coroner Always double check with the bereavement staff what is acceptable and what is not.

22
Death - TTO Diagnosis – 1a Type I Respiratory Failure Secondary 1b Community Acquired Pneumonia 1c – Mrs Blogs presented to ED with SOB and a productive cough. She was found to hypotensive, tachycardic and drowsy. An ABG revealed a Type I Respiratory Failure and CxR showed Left lower lobe consolidation. She required Iv Abx and NIV. Sputum Cultures grew S.Pneumoniae. Despite these treatments Mrs Blogs deteriorated and sadly passed away on 23/7/2015 at 16.15.

23
My General Tips Always, always work together When you’ve finished your work, help out someone else Leave on time, TOGETHER ALWAYS ask for help if you need it. Never be ashamed Never, ever, pass up an opportunity to poop, pee, eat or drink – you may not get that opportunity again!! Everyone has the same goal, be respectful, be helpful and it’s nice to be nice.

Similar presentations