Download presentation
Presentation is loading. Please wait.

1
MLAB 2401: Clinical Chemistry Keri Brophy-Martinez
Thyroid Gland

2
Anatomy Largest endocrine gland
Located in the lower part of the neck, wrapped around trachea and larynx Composed of two cell types Follicular Make and secrete thyroxine (T4) and triodothyronine (T3) Clear Secrete calcitonin
 and triodothyronine (T3) Clear. Secrete calcitonin.")
3
Thyroid Hormone Synthesis
Thyroid hormone is made up of iodine, primarily, so we must get iodine into the cell for thyroid function Daily intake of iodine should be 150 µg If < 50 µg/day: thyroid can not make thyroid hormone and leads to a deficiency Sources of Iodide seafood, dairy products, vitamins and iodine-enriched breads

4
Synthesis of Thyroid Hormones

5
Thyroid Hormones Triiodothyronine (T3) Thyroxine (T4) Calcitonin
Lowers plasma calcium Assists in calcium homeostasis Reverse T3 (rT3) Produced by the liver Inactive form of T3
 Produced by the liver. Inactive form of T3.")
6
Protein Binding of Thyroid Hormones
Once released into circulation, only small amounts of T4 and T3 are unbound and available for hormone activity Binding Proteins Thyroxine-binding globulin (TBG) Thyroxine-binding prealbumin (TBPA) albumin
 Thyroxine-binding prealbumin (TBPA) albumin.")
7
Thyroid Hormone Regulation
Regulation occurs via a feedback system between the thyroid gland, hypothalamus and anterior pituitary gland Hypothalamus produces TRH TRH asks the anterior pituitary to make and release TSH Free T3 and T4 hormones have a negative feedback effect to block TRH

8
Actions of Thyroid Hormone
Tissue growth Brain maturation Increased heat production Increased oxygen comsumption

9
Disorders of the Thyroid Gland

10
Terms Euthyroid Goiter Normal thyroid gland function
Condition where the thyroid gland grows larger than normal

11
Hypothyroidism Symptoms Lab features
Obesity, dry skin, dry lusterless hair, sluggishness of body functions and goiter Lab features Low free T4 level Normal to high TSH

12
Hypothyroidism Types Dysfunction Condition Primary Thyroid gland
Hashimoto’s thyroiditis Treatment for toxic goiter Excessive iodine intake Subacute thyroiditis Secondary Pituitary gland Hypopituitarism Tertiary Hypothalamus Hypothalamic

13
Thyrotoxicosis Causes Excessive thyroid hormone ingestion
Leakage of stored thyroid hormone from thyroid follicles Excessive production of thyroid hormone (hyperthyroidism)
")
14
Thyrotoxicosis Signs Symptoms Tachycardia Tremor
Warm, moist, flushed skin Goiter Muscle wasting and weakness Anxiety, nervousness Palpitations Weight loss Heat intolerance Prominence of eyes

15
Graves’ Disease Autoimmune Disease Familial Women more affected
Antibodies activate TSH receptor Familial Women more affected Lab Features High free T4 and/or T3 level TSH undetectable

16
Hyperthyroidism

17
Subacute Thyroiditis Condition where there is inflammation of the thyroid gland, leakage of stored thyroid hormone and repair of the gland Most common form is postpartum thyroiditis

18
Nonthyroidal Illness Abnormalities in thyroid function tests of hospitalized patients (especially critically ill patients) Characterized by low total T4, free T4, & TSH Less T4 is converted to active T3, leading to decreased levels of T3 and higher levels of reverse T3. Central hypothyroidism & thyroid hormone-binding changes are associated with severe illness. Changes may be appropriate adaptations to illness.

19
Thyroid Nodules Common 5–9% prove to be thyroid cancer.
Clinically apparent nodules are present in 6.4% of adult women & 1.5% of adult men. Thyroid ultrasound finds unsuspected nodules in 20–45% of women & 17–25% of men. 5–9% prove to be thyroid cancer. Fine-needle aspiration, with cytologic examination of aspirate, is used to determine need for surgical removal.

20
Assessment of the Thyroid

21
Historical Procedures
Basal Metabolic Rate Measured rate of oxygen consumption over a 15 minute period Required careful patient preparation and precision of testing Radioactive iodine uptake test Measured the ability of the thyroid to take up and trap iodine Rate of absorption is determined by measuring increased radioactivity in the thyroid gland

22
Historical Procedures
Protein bound iodine (PBI) Used to estimate the amount of thyroid T3 and T4 by measuring the amount of iodine contained in a protein precipitate of serum
 Used to estimate the amount of thyroid T3 and T4 by measuring the amount of iodine contained in a protein precipitate of serum.")
23
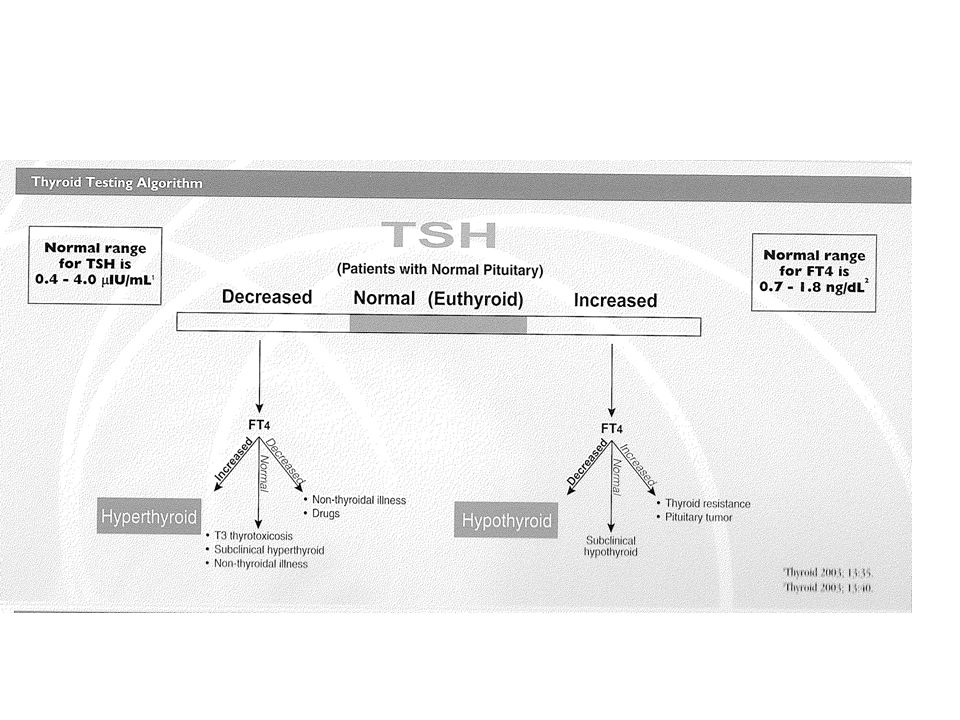
Common Thyroid Function Tests
TSH Total T3 and total T4 Free T3 and Free T4 T3 Uptake (for binding proteins) Free thyroxine index( estimate of Free T4) Serological testing for antibodies to thyroid disease
 Free thyroxine index( estimate of Free T4) Serological testing for antibodies to thyroid disease.")
25
Thyroid Testing Methods
Competitive binding techniques RIA ELISA FIA

26
Thyroid Antibodies Thyroglobulin antibodies
Anti-thyroglobulin antibodies are mostly IgG and do not fix complement Titerable using an indirect hemagglutination assay Found in Hashimoto’s thyroiditis Grave’s disease Subacute thyroiditis Thyroid cancer

27
Thyroid Antibodies Microsomal antibodies
Complement fixing IgG directed against a microsomal antigen within follicular cells Found in Hashimoto’s disease Thyrotoxicosis Primary myxedema

Similar presentations





 Triiodothyronine (T3) T4 and T3 regulate body metabolism.>")
 Triiodothyronine (T3) Calcitonin Energy & Growth Control.>")




 Destruction of thyroid tissue –Radioactive Iodine –Hashimoto’s –Surgical.>")


. Its size depends on: 1. age … age size. 2. sex … female > male. 3.>")



BB>")
. It has two lobes that are joined together.>")