Download presentation
Presentation is loading. Please wait.

1
VCU Death and Complications Conference

2
Introduction Complication Procedure Primary Diagnosis
Post operative bleeding, reoperation Procedure Deceased donor kidney transplant Primary Diagnosis Hypertension Give a synopsis of each case to start the presentation.

3
Clinical History HPI: 44 yo f with renal failure due to severe HTN since childhood. She has had 3 previous kidney transplants. PMH/PSH: 1989, 1999, 2007 kidney transplant 1999 AV and MV mechanical St. Jude valves, on Coumadin 2007 Left transplant nephrectomy 2008 Right femoral AVG Hyperparathyroidism, OSA, infectious endocarditis 1989 CKT 1999 LRKT from sister 1999 AV and MV mechanical valve replacement due to endocarditis from line infection 2007 midline LRKT, left nephrectomy transplant kidney 2008 R femoral AVG 1989 status post cadaveric kidney transplant which failed due to chronic allograft nephropathy 1999 status post living-related kidney transplant from her sister which failed due to chronic nephropathy. 2007 status post living-related kidney transplant from her daughter failed due to acute humoral rejection status post IV IF and plasmapheresis x3 months without improvement in her renal function. -calcitriol (calcitriol 0.25 mcg oral capsule)(Hx): 1CAP, daily -calcium acetate (PhosLo Gelcap 667 mg oral capsule)(Hx): 3CAP, three times a day -calcium carbonate (Tums)(Hx): , three times a day -ergocalciferol (Vitamin D)(Hx): -multivitamin (Nephrocaps oral capsule)(Hx): 1CAP, daily -warfarin (Coumadin)(Hx):
(Hx): 1CAP, daily. -calcium acetate (PhosLo Gelcap 667 mg oral capsule)(Hx): 3CAP, three times a day. -calcium carbonate (Tums)(Hx): , three times a day. -ergocalciferol (Vitamin D)(Hx): -multivitamin (Nephrocaps oral capsule)(Hx): 1CAP, daily. -warfarin (Coumadin)(Hx):")
4
Hospital Course INR 2.4 on admission INR 4.8 on POD #2
2mg Vitamin K INR 1.5 Heparin gtt with goal ptt 60-70 POD#4, Coumadin restarted POD#6: 2g drop in Hgb, hypotension, tenderness over incision, left flank pain, INR 2.3, PTT 79 US: large collection of blood in left retroperitoneum, obscuring and compressing transplant kidney; flow present in renal vein and artery

5
Hospital Course Return to OR for exploration POD#8, Hgb drop 8.9 7.1
~250 mL of blood surrounding the transplant kidney. Good flow in artery and vein, kidney slightly mottled, but viable. No active bleeding. Biopsy: mild tubulitis, not clearly rejection POD#8, Hgb drop 8.9 7.1 CT scan: large collection of blood in retroperitoneum, no mass effect on kidney; hematocrit effect with layering 2 U PRBC, 2 U FFP Large left-sided retroperitoneal hemorrhage extending from the inferior spleen to the superior aspect of the transplant kidney. It does not appear to exert mass effect on the transplant kidney. The JP drain courses along the posterior inferior aspect of the hematoma, and may not be adequately draining the hematoma. Hematocrit effect from blood in different stages within this hematoma implies relative acuity. Active extravasation cannot be assessed due to lack of IV contrast medium. 2. Mesenteric stranding in trace amount of fluid around left lower quadrant. Transplant kidney in the left lower quadrant. No hydronephrosis.

6
transplant kidney, JP drain
superior to transplant kidney just inferior to spleen

7
Hospital Course POD#11 2g hgb drop, hypotension, INR 1.5, PTT 30’s Repeat US with large collection of blood around transplant kidney (400mL) Second return to OR 1L blood evacuated, no focal areas of active bleeding POD#14 Current Hgb stable 9.1, 8.9, hemodynamically stable, INR 1.4

8
Analysis of Complication
Was the complication potentially avoidable? Yes, could have held anticoagulation or could have avoided surgery Would avoiding the complication change the outcome for the patient? Most likely, yes. No transfusions, no reoperation, no compression of transplant kidney. What factors contributed the complication? Anticoagulation, surgical dissection

9
Discussion points Mechanical valves Anticoagulation
Management of post operative bleeding Perinephric hematoma, transplant kidney

10
Mechanical valve thrombosis
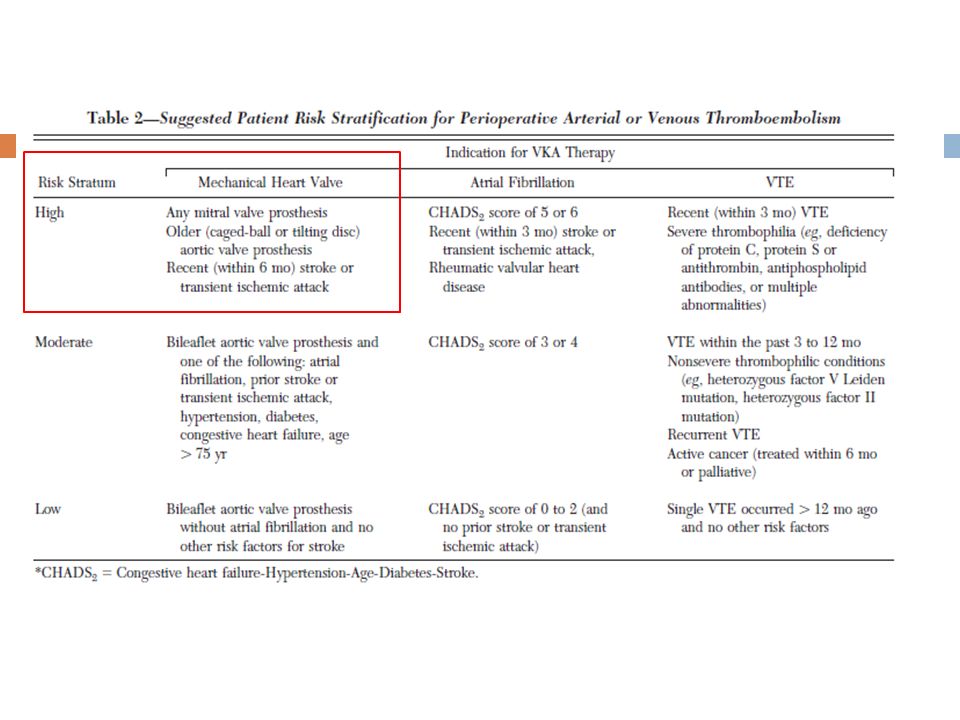
Highest risk of stroke/embolism/valve thrombosis Mitral position Caged-ball valve Two or more prosthetic valves Overall risk of valve thrombosis per year % on coumadin 2.2% on ASA 9-22% no anticoagulation (lower in some studies) % calculated absolute risk for 6-8 day post op warfarin interruption oral anticoagulant therapy: a practical guide for clinicians Perioperative anticoagulation management in patients who are receiving James D. Douketis* Department of Medicine, McMaster University, Hamilton, Ontario, Canada St. Joseph’s Hospital, Room F-538, 50 Charlton Avenue East, Hamilton, Ontario, Canada, L8N 4A6 Thrombosis research 2009 Prosthetic mitral valves are more thrombogenic than aortic prostheses because of greater vascular stasis around the mitral valve [35]. Providing reliable estimates of the absolute risk of thromboembolic events in such patients during temporary interruption of warfarin therapy is problematic because most data are based on studies performed 15–25 years ago and mainly involve patients with first-generation prosthetic heart valves. Nonetheless, it is estimated that the incidence of a thromboembolic event in patients with a prosthetic heart valve who are not receiving anticoagulant therapy is between 9% and 22% per year [36,37]. If one interpolates this risk to a 6–8 day perioperative period, when warfarin therapy is interrupted, this corresponds to an absolute risk of thromboembolism of 0.17–0.42%. Few studies have investigated the perioperative risk of thromboembolism so as to corroborate these risk estimates (Table 1). In four studies involving 271 patients with mostly first-generation prosthetic heart valves who underwent 300 procedures, 4 (1.3%) patients had a perioperative thromboembolic event despite bridging anticoagulant therapy [7–10]. In a retrospective study of 235 patients with newer prosthetic valve types (191 bileaflet, 51 tilting disc), of whom 164 had bridging anticoagulant therapy with full-dose UFH or LMWH, a higher rate of thromboembolism was reported [11]. In this study, 4 of 177 (2.3%) patients with a aortic valve prosthesis, 9 of 51 (18%) patients with a mitral valve prosthesis, and 3 of 7 (43%) patients with two prosthetic valves had a thromboembolic event. However, limitations of this study included inadequate information about clinical follow-up and the adequacy of perioperative anticoagulation. Two small, but well-designed, prospective cohort studies of bridging anticoagulant therapy with full-dose LMWH reported one thromboembolic event in 24 (4.2%) patients [5,6]. Overall, the discrepant findings from these studies underscore the need for large, well-designed, prospective studies to provide reliable estimates of the risk of thromboembolism in patients with a mechanical heart valve who have interruption of warfarin and receive bridging anticoagulant therapy. Based on the available evidence, a classification scheme that stratifies patients with a mechanical heart valve according to the thromboembolic risk, and a suggested anticoagulation management strategy for each risk category, is provided in Table 2. Douketis, James D. Perioperative anticoagulation management in patients who are receiving oral anticoagulant therapy: a practical guide for clinicians., Thrombosis research 2009
 % calculated absolute risk for 6-8 day post op warfarin interruption. oral anticoagulant therapy: a practical guide for clinicians. Perioperative anticoagulation management in patients who are receiving. James D. Douketis* Department of Medicine, McMaster University, Hamilton, Ontario, Canada. St. Joseph’s Hospital, Room F-538, 50 Charlton Avenue East, Hamilton, Ontario, Canada, L8N 4A6. Thrombosis research Prosthetic mitral valves are more thrombogenic. than aortic prostheses because of greater vascular. stasis around the mitral valve [35]. Providing reliable estimates of the absolute risk of. thromboembolic events in such patients during temporary. interruption of warfarin therapy is problematic because most. data are based on studies performed 15–25 years ago and. mainly involve patients with first-generation prosthetic heart. valves. Nonetheless, it is estimated that the incidence of a. thromboembolic event in patients with a prosthetic heart. valve who are not receiving anticoagulant therapy is. between 9% and 22% per year [36,37]. If one interpolates. this risk to a 6–8 day perioperative period, when warfarin. therapy is interrupted, this corresponds to an absolute risk of. thromboembolism of 0.17–0.42%. Few studies have investigated. the perioperative risk of thromboembolism so as to. corroborate these risk estimates (Table 1). In four studies. involving 271 patients with mostly first-generation prosthetic. heart valves who underwent 300 procedures, 4 (1.3%) patients had a perioperative thromboembolic event despite. bridging anticoagulant therapy [7–10]. In a retrospective. study of 235 patients with newer prosthetic valve types (191. bileaflet, 51 tilting disc), of whom 164 had bridging anticoagulant. therapy with full-dose UFH or LMWH, a higher. rate of thromboembolism was reported [11]. In this study, 4. of 177 (2.3%) patients with a aortic valve prosthesis, 9 of 51. (18%) patients with a mitral valve prosthesis, and 3 of 7. (43%) patients with two prosthetic valves had a thromboembolic. event. However, limitations of this study included. inadequate information about clinical follow-up and the. adequacy of perioperative anticoagulation. Two small, but. well-designed, prospective cohort studies of bridging anticoagulant. therapy with full-dose LMWH reported one. thromboembolic event in 24 (4.2%) patients [5,6]. Overall, the discrepant findings from these studies underscore the. need for large, well-designed, prospective studies to provide. reliable estimates of the risk of thromboembolism in patients. with a mechanical heart valve who have interruption of. warfarin and receive bridging anticoagulant therapy. Based. on the available evidence, a classification scheme that. stratifies patients with a mechanical heart valve according. to the thromboembolic risk, and a suggested anticoagulation. management strategy for each risk category, is provided in. Table 2. Douketis, James D. Perioperative anticoagulation management in patients who are receiving oral anticoagulant therapy: a practical guide for clinicians., Thrombosis research")
11
Chest 2008;133;299S-339S Recommendations: Coumadin discontinued 5 days prior to surgery, with reversal of INR to 1.5 or less FFP and low dose vitamin K for emergency reversal Good intraoperative hemostasis Coumadin restarted hours after surgery Anticipated partial effect within 48 hours In high risk cases, heparin bridge recommended several strategies with hours, therapeutic vs. low dose depending on bleeding risk In the postoperative period, the use of therapeuticdose LMWH administered can vary. The 3 principal management approaches that have been studied are: (1) to administer therapeutic-dose LMWH within a fixed time period after a procedure (within initial 24 h); (2) to administer therapeutic-dose LMWH within a varied time period after a procedure (24 to 72 h), with the initiation depending on the procedurerelated bleeding risk and the adequacy of postoperative hemostasis; and (3) to replace therapeutic-dose LMWH with low-dose LMWH in select patients who are undergoing a procedure associated with a high bleeding risk.
 to administer therapeutic-dose LMWH within a. fixed time period after a procedure (within initial. 24 h); (2) to administer therapeutic-dose LMWH. within a varied time period after a procedure (24 to. 72 h), with the initiation depending on the procedurerelated. bleeding risk and the adequacy of postoperative. hemostasis; and (3) to replace therapeutic-dose. LMWH with low-dose LMWH in select patients. who are undergoing a procedure associated with a. high bleeding risk.")
13
Anticoagulation held, mean of 15 +/- 4 days 24 Mechanical valves
28 patients with prosthetic heart valves hospitalized for major bleeding Anticoagulation held, mean of 15 +/- 4 days 24 Mechanical valves 20 patients with St. Jude valves 12 mitral valves (11 St Jude) 12 aortic valves (5 St Jude) 4 both aortic and mitral (all St. Jude) Thromboembolic events: zero at 6 month follow up One patient sudden death at 4 months, no post Major bleeding defined as requiring hospitalization, reversal of warfarin with vitamin K, FFP Included GI bleed, retroperitoneal hemorrhage, ICH, SDH Mean of 15 +/- 4 days off anticoagulation 5 pts were reversed with Vit K 7 pts were reversed with FFP Coumadin restarted in 22 of 24 pts prior to DC, had discharge No thromboembolic events 3 pts lost to FU 1 sudden home, no post 1 on ASA, no coumadin Twenty-eight patients with prosthetic heart valves receiving warfarin were hospitalized for major hemorrhage from 1990 to The mean 6 SD age was years (15 men and 13 women). Twenty patients had St. Jude valves, 4 patients had Carpentier-Edwards bioprosthetic valves, 2 patients had Starr Edwards valves, and 2 patients had Bjork-Shiley valves. Valves were in the mitral position in 12 patients, the aortic position in 12 patients, and both mitral and aortic positions in 4 patients. The average interval from valve surgery to index bleeding was 7 years. Twenty-five patients had GI or retroperitoneal hemorrhage, 2 patients had an intracranial hemorrhage, and 1 patient had a subdural hematoma. Interventions: Vitamin K was administered to five patients and fresh frozen plasma was given to seven patients to reverse anticoagulation. The mean duration of anticoagulation withholding was days.
 12 aortic valves (5 St Jude) 4 both aortic and mitral (all St. Jude) Thromboembolic events: zero at 6 month follow up. One patient sudden death at 4 months, no post. Major bleeding defined as requiring hospitalization, reversal of warfarin with vitamin K, FFP. Included GI bleed, retroperitoneal hemorrhage, ICH, SDH. Mean of 15 +/- 4 days off anticoagulation. 5 pts were reversed with Vit K. 7 pts were reversed with FFP. Coumadin restarted in 22 of 24 pts prior to DC, had discharge. No thromboembolic events. 3 pts lost to FU. 1 sudden home, no post. 1 on ASA, no coumadin. Twenty-eight patients with prosthetic heart valves receiving warfarin were hospitalized. for major hemorrhage from 1990 to The mean 6 SD age was years (15 men and 13. women). Twenty patients had St. Jude valves, 4 patients had Carpentier-Edwards bioprosthetic. valves, 2 patients had Starr Edwards valves, and 2 patients had Bjork-Shiley valves. Valves were. in the mitral position in 12 patients, the aortic position in 12 patients, and both mitral and aortic. positions in 4 patients. The average interval from valve surgery to index bleeding was 7 years. Twenty-five patients had GI or retroperitoneal hemorrhage, 2 patients had an intracranial. hemorrhage, and 1 patient had a subdural hematoma. Interventions: Vitamin K was administered to five patients and fresh frozen plasma was given to. seven patients to reverse anticoagulation. The mean duration of anticoagulation withholding was days.")
14
Page kidney Described by Irvine Page in 1939
Compression of animal kidneys with cellophane Seen with subcapsular/perinepheric hematoma, uroma Renal hypoperfusion Microvascular ischemia Hypertension due to activation of renin angiotensin system AKI, renal failure Evaluate by US, duplex US, CT scan Reversible by evacuation of hematoma, decapsulation, nephrectomy Acute Renal Failure and Severe Hypertension from a Page Kidney Post-Transplant Biopsy Division of Nephrology, Feinberg School of Medicine, Northwestern University, Chicago TheScientificWorldJOURNAL August 3, 2010

15
Learning points Mechanical valve type and location important for risk of thrombosis and need for anticoagulation. Anticoagulation may be held for life threatening bleed, but must be continually re-evaluated. Perinepheric hematoma that is compressing or obstructing transplant kidney should be evacuated to prevent ischemia and graft failure. 4. Assessment of postoperative bleeding risk The assessment of postoperative bleeding risk is based on the following considerations: (1) the adequacy of postoperative hemostasis; (2) the risk of bleeding and clinical consequences of bleeding associated with surgery or an invasive procedure. Patients with unexpected postoperative bleeding Major bleeding, defined as bleeding associated with transfusion of >2 U of packed red blood cells, reoperation, or bleeding into the intracranial, intrathoracic or retroperitoneal cavity [71], can be separated into surgical and nonsurgical bleeding. Surgical bleeding at the wound site is the most common source of bleeding [72–74] and usually results from delayed wound healing or intraoperative blood vessel injury. Bleeding can also occur from stress-induced peptic ulceration or a hemorrhagic stroke. The anticoagulant management in such patients depends on the cause and location of bleeding although, in general, anticoagulants should be withheld until the bleeding source has been identified and treated. If the cause of bleeding is reversible, as with the repair of a severed blood vessel that inadvertently occurred during surgery, anticoagulant therapy can be resumed probably within 24 h. In patients with gastrointestinal bleeding, anticoagulants can be withheld for as little as 2 days in patients with a self-limiting Mallory– Weiss tear, to as long as 21 days in patients with a large gastric ulcer [75,76]. In patients with intracranial bleeding, resumption of anticoagulants can occur within 1–4 weeks, depending on the extent of bleeding and radiologic evidence of healing [77–79].
 the adequacy of postoperative. hemostasis; (2) the risk of bleeding and clinical. consequences of bleeding associated with surgery or an. invasive procedure Patients with unexpected postoperative bleeding. Major bleeding, defined as bleeding associated with. transfusion of >2 U of packed red blood cells, reoperation, or bleeding into the intracranial, intrathoracic or retroperitoneal. cavity [71], can be separated into surgical and. nonsurgical bleeding. Surgical bleeding at the wound site. is the most common source of bleeding [72–74] and usually. results from delayed wound healing or intraoperative blood. vessel injury. Bleeding can also occur from stress-induced. peptic ulceration or a hemorrhagic stroke. The anticoagulant. management in such patients depends on the cause and. location of bleeding although, in general, anticoagulants. should be withheld until the bleeding source has been. identified and treated. If the cause of bleeding is reversible, as with the repair of a severed blood vessel that inadvertently. occurred during surgery, anticoagulant therapy can be. resumed probably within 24 h. In patients with gastrointestinal. bleeding, anticoagulants can be withheld for as. little as 2 days in patients with a self-limiting Mallory– Weiss tear, to as long as 21 days in patients with a large. gastric ulcer [75,76]. In patients with intracranial bleeding, resumption of anticoagulants can occur within 1–4 weeks, depending on the extent of bleeding and radiologic evidence. of healing [77–79].")
Similar presentations