Download presentation
Presentation is loading. Please wait.

1
Supervisor: Vs 余垣斌 Presenter: CR 周益聖

2
INTRODUCTION

3
VTE vs. Warfarin 2-3 per 1000 in the general population Recurrence after discontinuation of anticoagulant – 1% per year for transient risk factor – 10% per year for unprovoked VTE Warfarin (INR 2.0-3.0) for the long-term treatment of VTE – Major bleeding 2% per year – VTE risk reduction > 90% Low-intensity warfarin regimen (INR 1.5-2.0) for extended treatment – Major bleeding 0.9% per year – VTE risk reduction around 75-80% Becker, N Engl J Med 2012Linkins, Ann Intern Med. 2003Ridker, N Engl J Med 2003
 for the long-term treatment of VTE – Major bleeding 2% per year – VTE risk reduction > 90% Low-intensity warfarin regimen (INR ) for extended treatment – Major bleeding 0.9% per year – VTE risk reduction around 75-80% Becker, N Engl J Med 2012Linkins, Ann Intern Med. 2003Ridker, N Engl J Med")
4
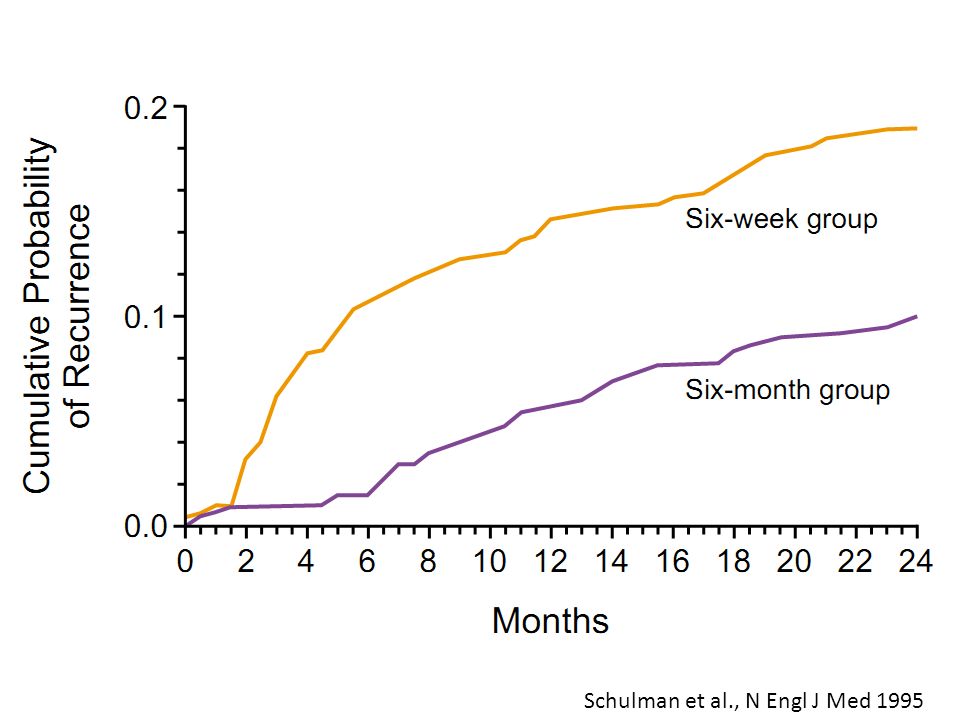
Schulman et al., N Engl J Med 1995 The Duration of Anticoagulation I Trial

5
Schulman et al., N Engl J Med 1995

8
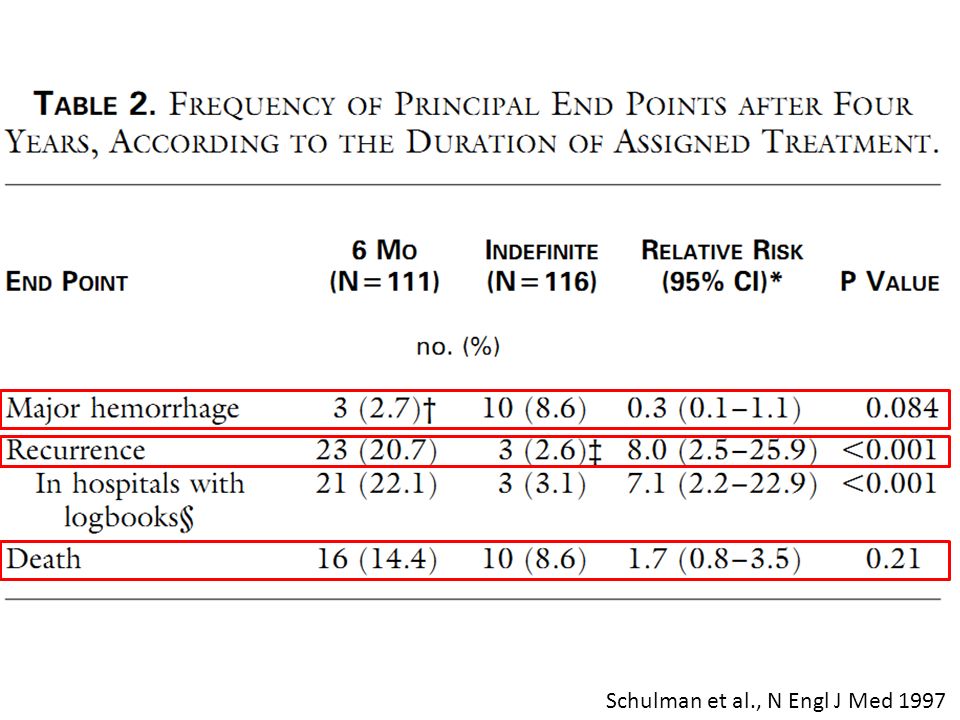
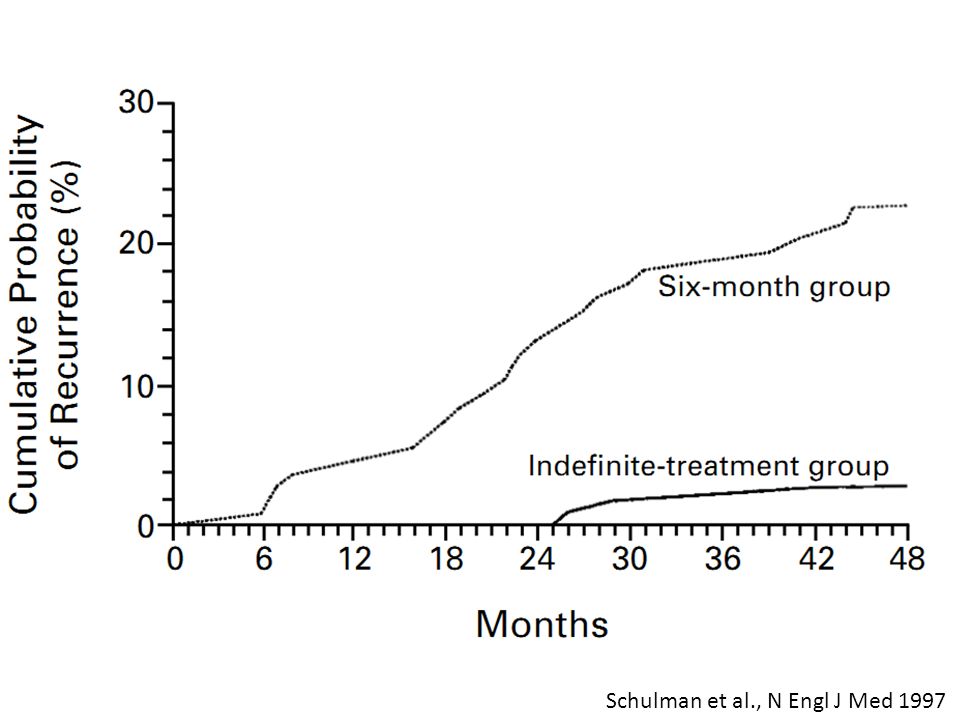
The Duration of Anticoagulation II Trial 6mos vs. indefinitely The Duration of Anticoagulation II Trial 6mos vs. indefinitely Schulman et al., N Engl J Med 1997

11
Kearon et al., N Engl J Med 1999

13
Schulman et al., N Engl J Med 1997

14
ACCP guideline (9 th edition) Antithrombotic Therapy for VTE VKA for 3 months – Proximal or isolated distal VTE provoked by surgery or non surgical risk factor – First Unprovoked distal VTE – PE provoked by surgery or non surgical risk factor Extended VKA except high bleeding risk – First Unprovoked proximal VTE – Second unprovoked VTE – First unprovoked DVT in cancer pt’ – First or second unprovoked PE Extended VKA no matter low or high bleeding risk – PE in active cancer VKA for 3 months – Proximal or isolated distal VTE provoked by surgery or non surgical risk factor – First Unprovoked distal VTE – PE provoked by surgery or non surgical risk factor Extended VKA except high bleeding risk – First Unprovoked proximal VTE – Second unprovoked VTE – First unprovoked DVT in cancer pt’ – First or second unprovoked PE Extended VKA no matter low or high bleeding risk – PE in active cancer Kearon et al., CHEST 2012; 141:Suppl(2):e419S-e4194S
 Antithrombotic Therapy for VTE VKA for 3 months – Proximal or isolated distal VTE provoked by surgery or non surgical risk factor – First Unprovoked distal VTE – PE provoked by surgery or non surgical risk factor Extended VKA except high bleeding risk – First Unprovoked proximal VTE – Second unprovoked VTE – First unprovoked DVT in cancer pt’ – First or second unprovoked PE Extended VKA no matter low or high bleeding risk – PE in active cancer VKA for 3 months – Proximal or isolated distal VTE provoked by surgery or non surgical risk factor – First Unprovoked distal VTE – PE provoked by surgery or non surgical risk factor Extended VKA except high bleeding risk – First Unprovoked proximal VTE – Second unprovoked VTE – First unprovoked DVT in cancer pt’ – First or second unprovoked PE Extended VKA no matter low or high bleeding risk – PE in active cancer Kearon et al., CHEST 2012; 141:Suppl(2):e419S-e4194S")
15
Pathogenesis of VTE Becker, N Engl J Med 2012

16
WARFASA The Warfarin and Aspirin Study Becattini et al., N Engl J Med 2012

17
Aim Assess the clinical benefit of aspirin for the prevention of recurrence after a course of treatment with vitamin K antagonists in patients with unprovoked venous thromboembolism

18
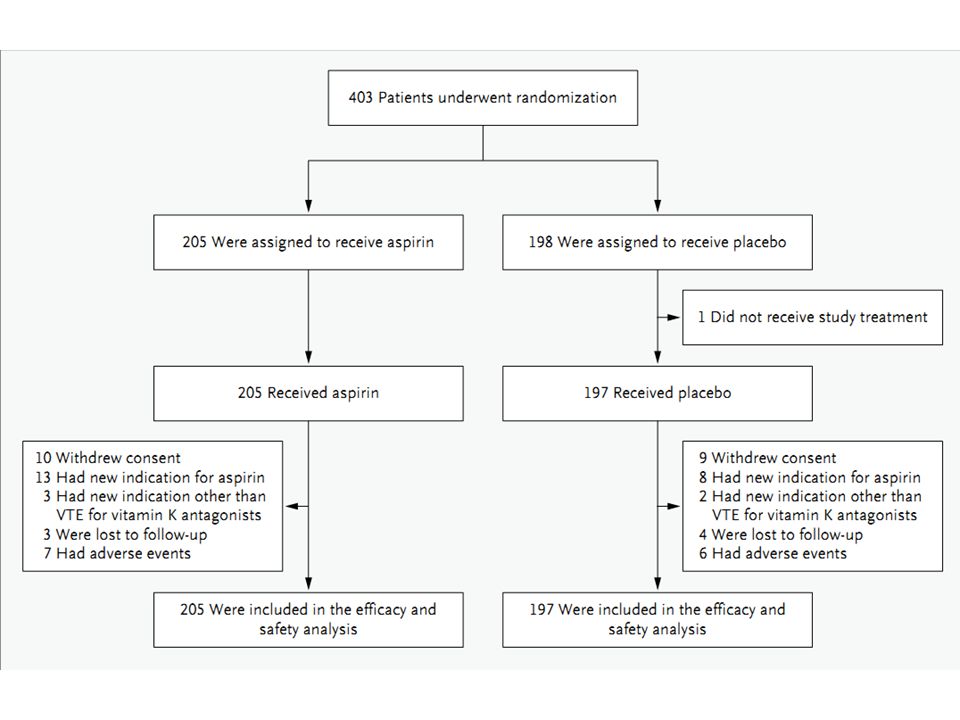
WARFASA Design Unprovoked VTE s/p Vitamin K antagonist RANDOMIZATIONRANDOMIZATION 1:1 n=205 n=197 Aspirin 100mg PO QD for 2 years Placebo for 2 years n=403 Assumption: 40% relative risk reduction with aspirin and expected event rate of 8.0% per year (Result:8.6%) 70 events provide a power of 80% Two sided α of 0.05
 70 events provide a power of 80% Two sided α of 0.05")
19
WARFASA Design Multicenter, Investigator-initiated, Double-blind Primary endpoint – recurrence of VTE Secondary endpoint – nonfatal myocardial infarction – unstable angina – Stroke – transient ischemic attack – acute ischemia of the lower limbs – death from any cause Principal safety outcome – major bleeding ( fatal, major organ, Hb↓ > 2g/dl, PRBC >2U)
")
20
Inclusion criteria older than 18 years of age treated for 6 to 18 months with vitamin K antagonists unprovoked proximal deep-vein thrombosis (DVT), pulmonary embolism (PE), or both – in the absence of any known risk factor
, pulmonary embolism (PE), or both – in the absence of any known risk factor")
21
Exclusion criteria Known cancer Known major thrombophilia – antiphospholipid antibodies – lupus anticoagulant – homozygous factor V Leiden – Prothrombin G21210A – deficiency of antithrombin, protein C or S – atrial fibrillation – prosthetic heart valve Atherosclerosis requiring treatment with aspirin or other anti-platelet agents Active bleeding or high risk for bleeding or a bleeding episode which occurred during the 6-18 months of anticoagulation Pregnancy or breast-feeding Women with venous thromboembolism associated with the use of estro- progestin therapy

23
Result

25
Recurrent VTE Deep-vein thrombosis – 44 patients (ipsilateral in 51% of cases) Pulmonary embolism – 27 patients (fatal in 2 patients) Prior PE is at higher risk for recurrent PE compared to prior DVT – 12.7% vs. 3.2% – HR:5.52 – 95% confidence interval : 2.29 to 13.30 – P<0.001

26
Intention to treat analysis 6.6% for aspirin vs. 11.2% for placebo per year – HR: 0.58 – 95%CI:0.36-0.93 – P=0.02

27
Post Hoc analysis Prior PE – 6.7% for aspirin vs. 13.5% for placebo per year – HR: 0.38 – 95%CI:0.17-0.88 – P=0.02 Prior DVT – 6.5% for aspirin vs. 10.2% for placebo per year – HR: 0.65 – 95%CI:0.65-1.20 – P=0.17

28
Risk factors for recurrent VTE Age>65 years – HR: 2.26 – 95%CI:1.16-4.41 – P=0.02 Male – HR: 2.02 – 95%CI:1.16-3.49 – P=0.01 No association between anticoagulant > 6 months vs. longer

30
Hemorrhagic complications Major bleeding – 1 bowel angiodysplasia in ASA vs. 1 gastric ulcer in placebo (0.3% per patient-year ) Non major bleeding – 1 gingival bleeding and 2 cutaneous hematoma in ASA – 2 musculoskeletal bleeding and 1 hemorrhagic gastritis in placebo
 Non major bleeding – 1 gingival bleeding and 2 cutaneous hematoma in ASA – 2 musculoskeletal bleeding and 1 hemorrhagic gastritis in placebo.")
31
Secondary outcome Death – 6 in ASA (1.4% per year ) vs. 5 in placebo (1.3% per year ) Sudden death – 1 in each due to PE Arterial events – 8 in ASA (1.9% per year ) vs. 5 in placebo (1.3% per year )
 Sudden death – 1 in each due to PE Arterial events – 8 in ASA (1.9% per year ) vs. 5 in placebo (1.3% per year ).")
32
AE Gastric pain – 1 in ASA and 2 in placebo 1 cutaneous reaction in ASA Renal failure in ASA Antiplatelet – 5 in ASA and 3 in placebo Anticoagulant – 3 in ASA and 2 in placebo

33
Discussion Aspirin therapy, begun after 6 to 18 months of oral anticoagulant treatment, reduces the rate of recurrence by about 40% – no apparent increase in the risk of major bleeding Aspirin is a potential alternative to extended oral anticoagulant treatment for the long-term secondary prevention of venous thromboembolism

34
Limitation Patients excluded – clinically significant thrombophilia – a bleeding event during the period of anticoagulant treatment Reduction in the risk of recurrence is lower with aspirin than with these new oral agents (80% for dabigatran and rivaroxaban) or low dose warfarin (60%) Underpowered for showing effect of aspirin on the incidence of IHD or CVA The results may not apply to whom require aspirin for the prevention of arterial events
 or low dose warfarin (60%) Underpowered for showing effect of aspirin on the incidence of IHD or CVA The results may not apply to whom require aspirin for the prevention of arterial events")
35
Strengths Randomized, placebo controlled, double blinded Treatment for 2 years ITT analysis = On treatment analysis

36
Conclusion Aspirin reduced the risk of recurrence when given to patients with unprovoked venous thromboembolism who had discontinued anticoagulant treatment With no apparent increase in the risk of major bleeding

37
Thanks for your attention!

Similar presentations