Download presentation
Presentation is loading. Please wait.

1
Neonatal Sepsis Maria Angelica M. Geronimo

2
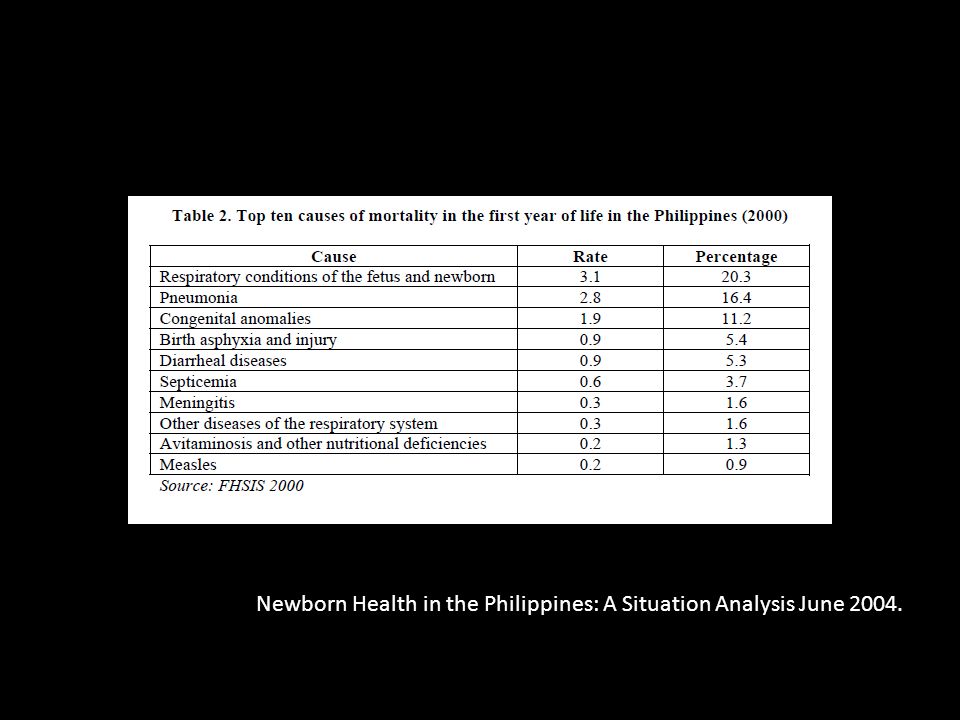
Epidemiology Newborn Health in the Philippines: A Situation Analysis June 2004.

4
Neonatal Sepsis Clinical syndrome of bacteremia with systemic signs and symptoms of infection in the first 4 weeks of life 1-4/1000 live births Term male infants 2x higher than female Pre Term have 3-10x higher incidence of infection than term Low Birth Weight

5
Sepsis Systemic inflammatory response syndrome resulting from a suspected or proven infection Nelson Textbook of Pediatrics 18 th edition

6
Clinical Spectrum Systemic Infection Localized infection Severe sepsis Death Multiple organ dysfunction syndrome Septic shock Nelson Textbook of Pediatrics 18 th edition

7
SIRS 2 out of 4 criteria, 1 of which must be abnormal temperature or abnormal leukocyte count 1. Core temperature >38.5°C or <36°C 2. Tachycardia Nelson Textbook of Pediatrics 18 th edition

8
SIRS 3. Respiratory rate >2 SD above normal for age or acute need for mechanical ventilation not related to neuromuscular disease or general anesthesia 4. Leukocyte count elevated or depressed for age (not secondary to chemotherapy) or >10% immature neutrophils Nelson Textbook of Pediatrics 18 th edition
 or >10% immature neutrophils Nelson Textbook of Pediatrics 18 th edition.")
9
Severe Sepsis Sepsis plus 1 of the following 1. Cardiovascular organ dysfunction – Despite >40 mL/kg of isotonic intravenous fluid in 1 hr – Hypotension <5th percentile for age, systolic blood pressure <2 SD below normal for age – Need for vasoactive drug to maintain blood pressure – 2 of the following: Unexplained metabolic acidosis or oliguria – Prolonged capillary refill 5 sec – Core to peripheral temperature gap >3°C Nelson Textbook of Pediatrics 18 th edition

10
Severe Sepsis 2. Acute respiratory distress syndrome (ARDS) Pa O 2/FiO 2 ratio ≤300 mm Hg Bilateral infiltrates on chest radiograph No evidence of left heart failure OR Sepsis plus 2 or more organ dysfunctions (respiratory, renal, neurologic, hematologic, or hepatic) Nelson Textbook of Pediatrics 18 th edition
 Pa O 2/FiO 2 ratio ≤300 mm Hg Bilateral infiltrates on chest radiograph No evidence of left heart failure OR Sepsis plus 2 or more organ dysfunctions (respiratory, renal, neurologic, hematologic, or hepatic) Nelson Textbook of Pediatrics 18 th edition.")
11
Septic Shock Sepsis plus cardiovascular organ dysfunction as defined above Nelson Textbook of Pediatrics 18 th edition

12
Multiple Organ Dysfunction Syndrome Presence of altered organ function such that homeostasis cannot be maintained without medical intervention Nelson Textbook of Pediatrics 18 th edition

13
Epidemiology Nelson Textbook of Pediatrics 18 th edition

14
Etiology AGEPATHOGENS NeonatesGroup B streptococcus Escherichia coli Listeria monocytogenes Enteroviruses Herpes simplex virus ChildrenStreptococcus pneumoniae Neisseria meningitidis Staphylococcus aureus (methicillin-sensitive or resistant) Nelson Textbook of Pediatrics 18 th edition
 Nelson Textbook of Pediatrics 18 th edition")
15
Predominant Pathogens for Sepsis Nelson Textbook of Pediatrics 18 th edition

16
Clinical Manifestation Hypo/hyperthermia Tachycardia Tachypnea Delayed capillary refill, Diminished peripheral and central pulses Cool extremities Decreased urine output. Alterations in mental status Nelson Textbook of Pediatrics 18 th edition

17
WHO study (2003) Predict Severe Bacterial Illness in Infants 1.Feeding ability reduced 2.No spontaneous movement 3.Temperature >38° C 4.Prolonged capillary refill time 5.Lower chest wall indrawing 6.Respiratory rate > 60/minute 7. Grunting 8.Cyanosis 9.Convulsions

18
Diagnosis Isolation – Blood – CSF – Urine – Pleural fluid – Pus

19
Diagnosis CBC and differential count ANC < 1800/ cmm – indicator of infection Neutropenia Immature neutrophils (Band+myelocytes+metamy elocytes) to total neutrophils ratio (I/T) > 0.20 Platelet count <100,000/cmm Toxic granules on peripheral smear and gastric aspirate - > 5 leukocytes/hpf Micro ESR – elevated with sepsis and fall of > 15 mm during the 1 st hour indicates infection C-reactive protein
 to total neutrophils ratio (I/T) > 0.20 Platelet count <100,000/cmm Toxic granules on peripheral smear and gastric aspirate - > 5 leukocytes/hpf Micro ESR – elevated with sepsis and fall of > 15 mm during the 1 st hour indicates infection C-reactive protein")
20
Diagnosis Sepsis screen 2 or more – Leukopenia (TLC < 5000/cmm) – Neutropenia (ANC <1800/cmm) – Immature neutrophil to total neutrophil (I/T) ratio (>0.2) – Micro ESR (<15mm 1 st hour) – CRP + CXR Lumbar puncture – late onset of sepsis – symptomatic early onset of sepsis
 – Neutropenia (ANC <1800/cmm) – Immature neutrophil to total neutrophil (I/T) ratio (>0.2) – Micro ESR (<15mm 1 st hour) – CRP + CXR Lumbar puncture – late onset of sepsis – symptomatic early onset of sepsis")
21
Management High index of suspicion Antibiotics Supportive care

22
Antibiotic Therapy AGEANTIBIOTIC Neonate Ampicillin plus aminoglycoside or cefotaxime + vancomycin if nosocomial infection +acyclovir if HSV Child Cefotaxime or ceftriaxone + vancomycin for meningitis or in areas of high staphylococcal or pneumococcal resistance to methicillin or cefotaxime, respectively Nelson Textbook of Pediatrics 18 th edition

23
Antibiotic Therapy Septicemia or Pneumonia AntibioticDosageFrequencyRouteDuration <7 days of age >7days of age Ampicillin50 mkdoseQ12Q8IV, IM7-10 days Cloxacillin50 mkdoseQ12Q8IV7-10 days Gentamicin2.5 mkdoseQ12Q8IV,IM7-10 days Amikacin7.5 mkdoseq12Q8IV, IM7-10 days

24
Antibiotic Therapy Meningitis AntibioticDosageFrequencyRouteDuration <7 days of age >7days of age Ampicillin and Gentamicin 100 mkdose 2.5mkdose Q12Q8IV 21 days Cefotaxime and Gentamicin 50 mkdose 2.5 mkdose Q12Q8IV 21 days

25
SEPSIS PROTOCOL M. Jeeva Sankar, Ramesh Agarwal, Ashok K Deorari, Vinod K Paul Division of Neonatology, Department of Pediatrics All India Institute of Medical Sciences Ansari Nagar, New Delhi –110029

26
SEPSIS PROTOCOL M. Jeeva Sankar, Ramesh Agarwal, Ashok K Deorari, Vinod K Paul Division of Neonatology, Department of Pediatrics All India Institute of Medical Sciences Ansari Nagar, New Delhi –110029

27
WHO Guidelines Chorioamnionitis – Elevated maternal temperature – Uterine tenderness – Foul smelling vaginal discharge – Maternal leucocytosis WBC>18 – Fetal tachycardia

28
WHO Guidelines Term and near term baby or birth wt. Of 2 kg or more with maternal history of chorioamnionitis and or fever with or without rupture of membranes – Blood CS (+) or baby develops signs and symptoms antibiotic for 10 days – Blood CS (-) and baby is asymptomatic after 5 days discontinue antibiotics – Blood CS not done and baby is asymptomatic after 5 days discontinue antibiotics
 or baby develops signs and symptoms antibiotic for 10 days – Blood CS (-) and baby is asymptomatic after 5 days discontinue antibiotics – Blood CS not done and baby is asymptomatic after 5 days discontinue antibiotics.")
29
WHO Guidelines Observe the baby for 24 hours after discontinuing antibiotics – Baby remains well, feeds well and there are no problems Discharge the baby – Explain to the mother the signs of sepsis or ask to return with the baby if signs of sepsis develops

30
WHO Guidelines Term and near term baby or birth wt. of 2 kg or more with maternal history ruptured bag of water with or without chorioamnionitis, fever – Blood sample for Culture and sensitivity do not start antibiotics – Observe the baby for signs of sepsis every 4 hours for 48 hours

31
WHO Guidelines – Blood CS (-) and baby is well after 48 hours observation discharge the baby – Explain to the mother the signs of sepsis or ask to return with the baby if signs of sepsis develops – Blood CS (+) is positive or baby develop signs of sepsis (during the 48 hours observation) treat for sepsis and start antibiotics – Blood CS is not possible observe the baby for additional 3 days remains well discharge baby
 and baby is well after 48 hours observation discharge the baby – Explain to the mother the signs of sepsis or ask to return with the baby if signs of sepsis develops – Blood CS (+) is positive or baby develop signs of sepsis (during the 48 hours observation) treat for sepsis and start antibiotics – Blood CS is not possible observe the baby for additional 3 days remains well discharge baby")
32
WHO Guidelines Gestational age less than 35 weeks of birth weight less than 2 kg with maternal history of either or both of the following: – Maternal fever / chorioamnionitis – PROM more than 18 hours

33
WHO Guidelines – Blood CS (+) or if baby develops signs and symptoms continue 10 days treatment with antibiotics – Blood CS (-) and baby is asymptomatic after 5 days of treatment discontinue antibiotics – Blood culture is not possible but baby remains asymptomatic after 5 days of treatment discontinue antibiotics
 or if baby develops signs and symptoms continue 10 days treatment with antibiotics – Blood CS (-) and baby is asymptomatic after 5 days of treatment discontinue antibiotics – Blood culture is not possible but baby remains asymptomatic after 5 days of treatment discontinue antibiotics")
34
WHO Guidelines Observe the baby for 24 hours after discontinuing antibiotics – Baby remains well, feeds well and there are no problems Discharge the baby – Explain to the mother the signs of sepsis or ask to return with the baby if signs of sepsis develops

35
Prevention Good antenatal care All mothers should be immunized against tetanus Babies should be fed early and exclusively with breast milk Cord should be kept clean and dry Immunization with the conjugate H. influenzae type b and S. pneumoniae vaccines is recommended for all infants

36
Prevention Hand Washing Nursery environment should be clean and dry with 24 hour water and electricity Adequate ventilation Nursery temperature maintained between 30 – 32 C Avoid overcrowding Mask and gloves Every baby must have separate thermometer and stethoscope

37
Thank You!

Similar presentations

>")

















