Download presentation
Presentation is loading. Please wait.

1
Bovine Abomasal Surgery
By Eoin Ryan MVB

2
Introduction Abomasal Surgery Post-op Medical Management LDA RDA
RTA/RVA Post-op Medical Management

3
Surgical Approaches to the Bovine Abdomen
Left flank: caesarean sections, access to rumen, LDA Right flank: thorough exploration of the abdomen possible (SI & LI), LDA, RDA &RDA and torsion Right paramedian: caesarean sections to remove emphysematous calves, LDA & RDA Midline: rarely used Flank approach far and away the most common, incise through all layers, grid incision or modified grid Method of closure varies (external rectus sheath apposition critical in the paramedian approach)
, LDA, RDA &RDA and torsion. Right paramedian: caesarean sections to remove emphysematous calves, LDA & RDA. Midline: rarely used. Flank approach far and away the most common, incise through all layers, grid incision or modified grid. Method of closure varies (external rectus sheath apposition critical in the paramedian approach)")
6
Flank Anaesthesia Line block Inverted “L”
Paravertebral: blocks T13, L1 & L2 cranial to L1, L2 & L3 Care: Do not overdo the volume, preparations with adrenaline may cause ischemia

10
Abomasal Surgery LDA – Left Displaced Abomasum
RDA – Right Displaced Abomasum RVA – Right Volvulus of the Abomasum

11
Risk Factors for Abomasal Problems
High concentrate diet Insufficient crude fibre & roughage Hypocalcaemia – clinical or subclinical Stress / Concurrent disease (50 – 60% cows) eg ketosis, fatty liver, metritis, RFM Twins / large calf More common in both young and old cows Higher yielders Most common in the first 6 weeks post-calving May occur up to 6 weeks before calving
 eg ketosis, fatty liver, metritis, RFM. Twins / large calf. More common in both young and old cows. Higher yielders. Most common in the first 6 weeks post-calving. May occur up to 6 weeks before calving.")
12
Diagnosis History & Signalment Clinical Exam
Dairy cow recently calved, back in the milk and not eating concentrates (selective inappetance – ketosis) Clinical Exam Abdominal percussion Rumeno-reticular motility Rectal examination Heart rate (very important in differentiating dilation from volvulus) Skin tent / sunken eyes
 Clinical Exam. Abdominal percussion. Rumeno-reticular motility. Rectal examination. Heart rate (very important in differentiating dilation from volvulus) Skin tent / sunken eyes.")
13
Abnormal “Pings” Left flank dorsally, under last ribs:
DDx: LDA 99% of the time Much less likely: rumen gas cap; pneumoperitoneum, abscess on Left body wall Right flank craniodorsally under rib cage: RDA/RVA (RVA “pings” can extend cranially as far as the 9th intercostal space) Caecal torsion/volvulus Right paralumbar fossa: Caecal dilation/volvulus Right sided abomasal volvulus
 Caecal torsion/volvulus. Right paralumbar fossa: Caecal dilation/volvulus. Right sided abomasal volvulus.")
14
Thorough Percussion: Detection of pings

15
Left Displaced Abomasum

16
Right Displaced Abomasum: two common sites

18
Diagnostic Tests Haematology - not a lot to be seen usually
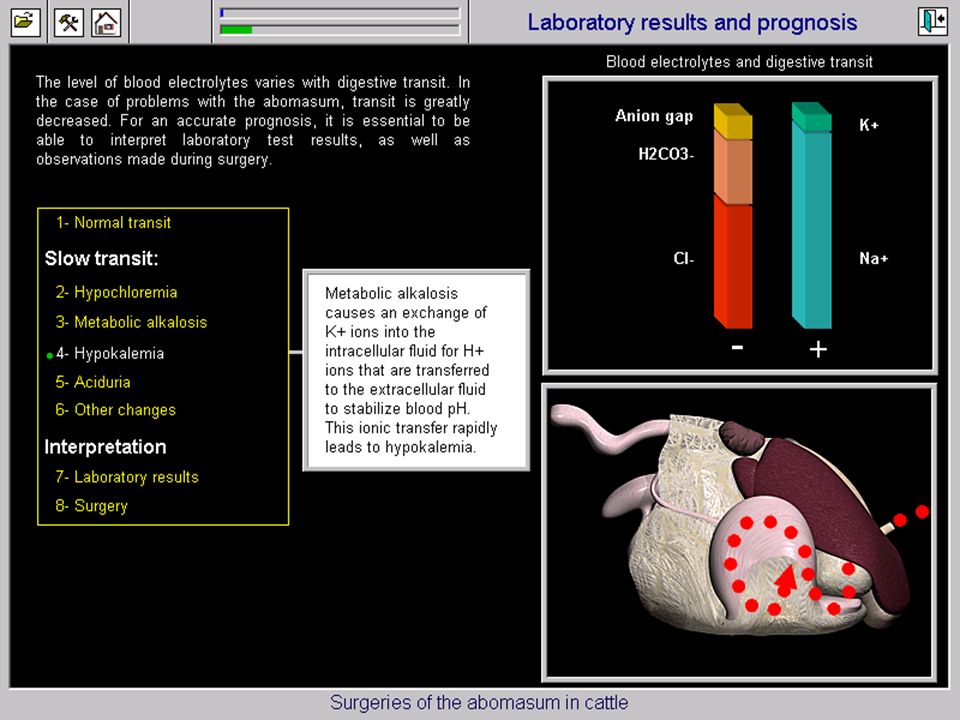
Serum biochemistry hypochloraemia (proximal GI obstruction) hypokalaemia (proximal GI obstruction) metabolic alkalosis (proximal GI obstruction) ketosis - -hydroxybutyrate (LDA / RDA) hypocalaemia (abomasal /caecal displacement) Liptac test Using auscultation and percussion, identify the area of “pings” “Pings” = gas; below this should be abomasal fluid Insert a 9cm 18G spinal needle 2 inches below the bottom of the “pings” and aspirate fluid If pH < 5 = abomasal fluid
 hypokalaemia (proximal GI obstruction) metabolic alkalosis (proximal GI obstruction) ketosis - -hydroxybutyrate (LDA / RDA) hypocalaemia (abomasal /caecal displacement) Liptac test. Using auscultation and percussion, identify the area of pings Pings = gas; below this should be abomasal fluid. Insert a 9cm 18G spinal needle 2 inches below the bottom of the pings and aspirate fluid. If pH < 5 = abomasal fluid.")
24
Prognosis for Return to Function
Medical therapy alone – only 5-15% Closed surgical procedures – 77-91% Conventional open surgeries – %

25
Intervention V Culling
Cost-benefit analysis (Abonyi, 1988) “with the policy of early surgical intervention the surplus value of additional meat and milk production and breeding performance, discounting the value of meat had the animals been immediately destroyed or culled, out weighed the total costs of intervention by a factor of 5.76”
 with the policy of early surgical intervention the surplus value of additional meat and milk production and breeding performance, discounting the value of meat had the animals been immediately destroyed or culled, out weighed the total costs of intervention by a factor of 5.76")
26
Abomasal Repositioning and Stabilisation
Closed techniques: rolling (high % of recurrence) percutaneous toggling Open techniques: Right flank omentopexy Left flank abomasopexy Right paramedian abomasopexy
 percutaneous toggling. Open techniques: Right flank omentopexy. Left flank abomasopexy. Right paramedian abomasopexy.")
27
CONSERVATIVE TREATMENT
Rolling Cast to right lateral recumbency Then dorsal recumbency, rock gently & ping Sharp rotation onto left side ; then onto sternal recumbency and allow to stand High % recurrence Occasionally can result in RDA or RVA NB – LDA only ; Rolling is contraindicated with RDA due to risk of inducing RVA

28
Transportation Helps expel gas from abomasum
Transient reduction or loss of “ping” Often returns rapidly (within 6 to 8 hours) Does not necessarily restore normal position or function If risk factors for initial displacement still there - i.e. metritis; ketosis; hypocalcaemia; high concentrate diet – high likelihood of recurrance
 Does not necessarily restore normal position or function. If risk factors for initial displacement still there - i.e. metritis; ketosis; hypocalcaemia; high concentrate diet – high likelihood of recurrance.")
29
Surgical Treatments for LDA
Right Flank Omentopexy Pyloropexy Left flank Abomasopexy Right Paramedian abomasopexy Toggle pin fixation

30
PRE-OP MED MANAGEMENT Electrolyte imbalances :
Abomasal conditions – hypochloraemic, hypokalaemic, metabolic alkalosis Fluid therapy : LDA/RDA – usually do not require fluids pre-op RVA – severe dehydration/shock Hypertonic saline 7.2% (216g in 3L pumped in over mins) Follow with isotonic10L 0.9% NaCl iv (90g salt in 10L water) at rate of 4-6L/hr Add KCl at 0.2% = 20g/10L ; NB No HCO3¯
 Follow with isotonic10L 0.9% NaCl iv (90g salt in 10L water) at rate of 4-6L/hr. Add KCl at 0.2% = 20g/10L ; NB No HCO3¯")
31
PRE-OP MED MANAGEMENT 400ml 40% Ca borogluconate s/c NSAIDs
Antimicrobials

33
Right Flank Omentopexy
NB. Position for incision site critical Bottom of incision should be as close as possible to normal position of pylorus Bottom of incision should be level with point where the ribs stop coursing caudally and begin to turn cranially The incision should be no more then 2 inches caudal to the last rib The length of incision is 6-8 inches (arm width) Most common cause of surgical failure folowing omentopexy = tension due to incision placed too high and caudal
 Most common cause of surgical failure folowing omentopexy = tension due to incision placed too high and caudal.")
35
Right Flank Omentopexy
Ventral deviation of duodenum and mesoduodenum Direct palpation of viscus to left of rumen Gas decompression using 14G needle and 40 cm tubing (water bowl) Push deflated abomasum under the rumen and apply gentle traction to the omentum Identify omentum close to pylorus, “sow’s ear” not a consistent finding and may be too friable anyway Incorporate 8-10cm length of omentum into the peritoneal/transversus first layer of abdominal wall closure
 Push deflated abomasum under the rumen and apply gentle traction to the omentum. Identify omentum close to pylorus, sow’s ear not a consistent finding and may be too friable anyway. Incorporate 8-10cm length of omentum into the peritoneal/transversus first layer of abdominal wall closure.")
42
4 Cardinal Points to the Omentopexy
(1) Proper Placement of Incision Site The incision should not be too high or too far caudal (bottom of incision level with point where ribs stop coursing caudally and start to turn cranially) – otherwise tension may cause omentum to tear leading to failure If the incision is made too far ventrally the intestines will prolapse making surgery and closure in particular difficult
 Proper Placement of Incision Site. The incision should not be too high or too far caudal (bottom of incision level with point where ribs stop coursing caudally and start to turn cranially) – otherwise tension may cause omentum to tear leading to failure. If the incision is made too far ventrally the intestines will prolapse making surgery and closure in particular difficult.")
45
4 Cardinal Points to the Omentopexy
(2) Require a thick strong piece of omentum close to the pylorus Classically the sow’s ear is used if strong enough (located 2-3 inches from pylorus and triangular in shape – frequently too small or not present) Omentum should be within 4 inches of the pylorus and strong enough to hold 2 mattress stay sutures If >4 inches from pylorus – risk of torsion around pexy
 Require a thick strong piece of omentum close to the pylorus. Classically the sow’s ear is used if strong enough (located 2-3 inches from pylorus and triangular in shape – frequently too small or not present) Omentum should be within 4 inches of the pylorus and strong enough to hold 2 mattress stay sutures. If >4 inches from pylorus – risk of torsion around pexy.")
48
4 Cardinal Points to the Omentopexy
(3) Surgical pexy must be performed that will last a minimum of 3 weeks so that a good adhesion will form Suture material must be strong (6-8 metric catgut or polyglyclic acid – Safil/Vicryl) The peritoneum must be included If omentum is friable (chronic DA in a cow in very low BCS) then a pyloropexy may also be performed (stitches placed partial thickness through pylorus as well as omentum)
 Surgical pexy must be performed that will last a minimum of 3 weeks so that a good adhesion will form. Suture material must be strong (6-8 metric catgut or polyglyclic acid – Safil/Vicryl) The peritoneum must be included. If omentum is friable (chronic DA in a cow in very low BCS) then a pyloropexy may also be performed (stitches placed partial thickness through pylorus as well as omentum)")
49
4 Cardinal Points to the Omentopexy
(4) Spread the weight-bearing load when suturing 2 horizontal mattress sutures are placed at the bottom of the incision to take the main weight of the pylorus and abomasum (should be little pull on pexy if incision is low enough) Sutures pass through internal AO, transversus Ab, peritoneum, omentum and back through the same layers Sutures in cranial edge of the incision only
 Spread the weight-bearing load when suturing. 2 horizontal mattress sutures are placed at the bottom of the incision to take the main weight of the pylorus and abomasum (should be little pull on pexy if incision is low enough) Sutures pass through internal AO, transversus Ab, peritoneum, omentum and back through the same layers. Sutures in cranial edge of the incision only.")
50
4 Cardinal Points to the Omentopexy
(4) Spread the weight-bearing load when suturing A bite of omentum is taken as part of the simple continuous closure until half way up the closure when starting from the bottom – this spreads the weightbearing load giving the pexy greater holding power
 Spread the weight-bearing load when suturing. A bite of omentum is taken as part of the simple continuous closure until half way up the closure when starting from the bottom – this spreads the weightbearing load giving the pexy greater holding power.")
58
Left Flank Abomasopexy
Advantage of identification of ulcers or adhesions Disadvantage – requires 2 operators for proper suture placement Continuous suture with long ends placed in abomasum (not into lumen) 5-7 cms from junction with the omentum 2nd operator tells principal surgeon where to place external sutures Cranial piece through first 6” caudal to xiphoid and 2” to right of midline, 2nd needle placed 4” caudally Care not to incarcerate anything Suture left in for 4-6 weeks
 5-7 cms from junction with the omentum. 2nd operator tells principal surgeon where to place external sutures. Cranial piece through first 6 caudal to xiphoid and 2 to right of midline, 2nd needle placed 4 caudally. Care not to incarcerate anything. Suture left in for 4-6 weeks.")
63
Right Paramedian Abomasopexy
The cow is sedated and rolled into dorsal recumbency The abomasum (unless adhesed) will float to the midline Tends to evacuate itself Incision Site: halfway between midline and milk vein, 2” cranial to the umbilicus and running forward 8” Incorporate omentum in the 1st layer of abdominal closure (internal rectus sheath and peritoneum) Vital to appose the external rectus sheath well
 will float to the midline. Tends to evacuate itself. Incision Site: halfway between midline and milk vein, 2 cranial to the umbilicus and running forward 8 Incorporate omentum in the 1st layer of abdominal closure (internal rectus sheath and peritoneum) Vital to appose the external rectus sheath well.")
64
Disadvantages of Right Paramedian Abomasopexy
Need help for casting and restraint Dangers of hypoxaemia and aspiration of ruminal reflux Large blood vessels – increased haemorrhage Risk of abomasal fistulation and/or peritonitis

69
Abomasal Fistulae Umbilical hernia or infection Perforating ulcers
Complication of abomasopexy Treatment: surgical correction

71
Toggle Pin Fixation Closed Laparoscopic

72
Closed Toggle-Pin Fixation
The cow is cast (+/- sedation) into dorsal recumbency The abomasum should rise allowing the surgeon to detect “pings” on the ventral abdomen The cow is rocked until the abomasum is returned to the right of midline The trochar is introduced into the area of “pings” 4 inches from midline and 4 inches caudal to the sternum
 into dorsal recumbency. The abomasum should rise allowing the surgeon to detect pings on the ventral abdomen. The cow is rocked until the abomasum is returned to the right of midline. The trochar is introduced into the area of pings 4 inches from midline and 4 inches caudal to the sternum.")
73
Closed Toggle-Pin Fixation
The first toggle is then inserted quickly so that all the gas does not escape The second toggle is placed 3 inches caudally to the first and the two ends tied The suture should be left in place for 4 to 6 weeks Disadvantages: blind surgery so there can be incarceration of bowel; incorrect realignment of abomasum; fistula formation

80
Laparoscopic Toggle-Pin Fixation
Advantages: can see where toggles are placed and ensure correct alignment and placement of the abomasum Disadvantages: initial capital expenditure (€5,000 approx.) to purchase equipment Still requires casting of the cow and the help needed for this
 to purchase equipment. Still requires casting of the cow and the help needed for this.")
81
Omentopexy V Toggle-Pin
Cost-benefit analysis (Bartlett, 1995) Costs considered : cost of treatment ; milk loss ; livestock loss (replacement cost & slaughter value based on % treated animals lost to herd within 120 days) Cost by Toggle-pin was 65% of cost by omentopexy Milk loss – 10% more for Toggle-pin
 Costs considered : cost of treatment ; milk loss ; livestock loss (replacement cost & slaughter value based on % treated animals lost to herd within 120 days) Cost by Toggle-pin was 65% of cost by omentopexy. Milk loss – 10% more for Toggle-pin.")
82
Omentopexy V Toggle-Pin
Best access to entire abdomen with right open surgery Toggle-pin contra-indicated with RDA and RVA Toggle-pin : risks of entrapment of bowel + penetration of another viscus + improper relocation + fistulation Right Flank Omentopexy Preferable in valuable animal

83
Right Displacement of the Abomasum (RDA)
Right Dilation of the Abomasum RVA/RTA Right Volvulus/Torsion of the Abomasum

84
Right Displaced Abomasum
Diagnosis: Dilation: similar to LDA history in dilation cases, “pings” under last 2 ribs on right flank, can’t palpate it on rectal examination, no signs of severe systemic changes Treatment: Right flank omentopexy Incision as for LDA Deflate with 14G needle – abomasum drops down below incision site Locate pylorus; duodenum should be visible also Perform omentopexy as for LDA

87
Right Torsion/Volvulus of the Abomasum
Depending on longevity of condition, cows show varying degrees of systemic involvement – sunken eyes, skin tent, distended abdomen, fluid on ballottement, large area of “pings” on right flank, occasionally palpable per rectum in advanced cases (poor prognosis) Severe hypokalaemia
 Severe hypokalaemia.")
89
Right Torsion/Volvulus of the Abomasum
Main surgical difference between RVA and RDA = RDA is gas-filled whereas RVA is mainly fluid-filled especially in advanced cases Right flank laparotomy Deflation with 14G needle Usually must release fluid to untorse A purse-string suture is placed in the abomasal wall (partial thickness)
")
92
Right Torsion/Volvulus of the Abomasum
An assistant places a double-throw and holds the two ends ready to tighten the purse-string when necessary The surgeon makes a shallow incision in the centre of the purse-string through the serosa, muscularis but not the mucosa A large stomach tube is pushed through the mucosa and the purse-string tightened simultaneously to prevent leakage

95
Right Torsion/Volvulus of the Abomasum
The fluid is siphoned off and its volume is measured to determine prognosis (>25 litres gives a bad prognosis due to overstretching of abomasal muscle and possible vagal nerve damage leading to ileus post-op) The incision is over-sowed and cleaned
 The incision is over-sowed and cleaned.")
98
Right Torsion/Volvulus of the Abomasum
The torsion/volvulus is invariably anti- clockwise and from lateral to medial The surgeon must place their arm ventrally and toss the abomasum in a clockwise direction and from medial to lateral If untwisted correctly the pylorus can be drawn up to the incision without excessive tension and the duodenum seen coursing caudally

103
Right Torsion/Volvulus of the Abomasum
Omentopexy is performed as before Post-op medical management is extremely important Intravenous fluids (hypertonic/isotonic) Oral fluids - stomach tube 20L water containing 200 to 250g coffee (caffeine stimulates abomasal motility and emptying) 100g KCl (1 tub of Lo Salt) propylene glycol “Stimulex” powders
 Oral fluids - stomach tube 20L water containing. 200 to 250g coffee (caffeine stimulates abomasal motility and emptying) 100g KCl (1 tub of Lo Salt) propylene glycol. Stimulex powders.")
104
Post-Op Medical Management
Routine Post-op Treatment for LDA / RDA 400ml 40% Ca borogluconate s/c off concentrates for 48 hours antibiotics for 5 days NSAIDs In severe cases a lidocaine drip is recommended to combat ileus -

107
Post-Op Medical Considerations
RVA – as well as the hypochloraemia and metabolic alkalosis, there is a much more severe hypokalaemia which leads to muscle weakness, dullness and reduced smooth muscle contractility Potassium cannot be supplemented iv at > 0.2% solution Therefore, the best way to raise a severely low blood potassium is via oral supplementation

108
POST-OP MED MANAGEMENT
10 – 20L of isotonic saline with 0.2% KCl iv over 2-3 hours is ideal (2g KCl/L) K+ can be given PO at a dose of 0.5-1g/kg Can give 0.5g/kg KCl up to a maximum of 1g/kg KCl in a 24 hour period For RVA give 150 to 300g KCl depending on severity and amount of fluid drained from abomasum
 K+ can be given PO at a dose of 0.5-1g/kg. Can give 0.5g/kg KCl up to a maximum of 1g/kg KCl in a 24 hour period. For RVA give 150 to 300g KCl depending on severity and amount of fluid drained from abomasum.")
109
Post-Op Ileus Ileus = abnormal lack of motility of the gastrointestinal tract Post-op ileus occurs after almost every surgery, especially surgeries involving the GIT It is a major problem post-RVA Combat ileus : caffeine ; Ca borogluconate ; laxatives ; probiotics Treatment of choice for severe paralytic ileus = Intravenous Lidocaine Therapy lidocaine dose = 50ml/litre at slow to medium flow rate - usually give a total of 10L daily (500ml lidocaine in 10 litres saline)
")
110
Prognosis with RVA ↓ with heart rate >100 bpm
↓ with severity of systemic signs pre-op NB : very poor if > 20L fluid in abomasum ↓ with concurrent abomasal ulcer Must pick up and perform surgery in first 12 hrs for reasonable prognosis

111
Abomasal Surgery - Conclusions
Early surgical intervention is warranted in >90% of cases of abomasal displacement It is important to be confident and skilled in performing surgical procedures Pre and post-op medical management is vital in returning cows to productivity as quick as possible

112
Pedigree Jersey V Holstein
Jersey cows are much more delicate Jersey cows are more prone to hypocalcaemia (clinical and subclinical) Jersey cows are equally as susceptible to developing LDA’s, RDA’s, RVA’s and caecal dilation/torsion In my experience it is best to operate ASAP rather than treat medically If left they very quickly become weak and recumbent making surgery difficult/impossible
 Jersey cows are equally as susceptible to developing LDA’s, RDA’s, RVA’s and caecal dilation/torsion. In my experience it is best to operate ASAP rather than treat medically. If left they very quickly become weak and recumbent making surgery difficult/impossible.")
113
Acknowledgements John Berkery and Donal Lynch and the XL VETS team
The sponsors Intervet-Schering Plough Animal Health for facilitating the talk Thank you for listening

Similar presentations






























































,>")















