Download presentation
Presentation is loading. Please wait.

1
Bronchial asthma By: Nur Izzatul Ashikin Harun Moderator: Dr Nik Azman Nik Adib

2
Outline Definition Diagnosis Management and prevention 1 Develop patient-doctor relationship 2 Identify and reduce exposure to risk factor 3 Assess, treat and monitor asthma 4 Management of exacerbation Management of life threatening asthma

3
Introduction Asthma is a serious public health problem throughout the world When uncontrolled, asthma can place several limits on daily life and is sometimes fatal Early diagnosis of asthma and implementation of appropriate therapy significantly reduce the socioeconomic burden of asthma and enhance patients’ quality of life

4
Updated 2012

5
Objective To increase awareness on asthma among health professionals, public health authorities, and the genaral public To improve prevention and management of asthma through a concerted worldwide effort

6
GINA Offers a framework to achieve and maintain asthma control for most patient that can be adapted to local health care systems and resources

7
Definition Chronic inflammatory disorder of the airways associated with airway hyperreposive that leads to widespread but variable airflow obstruction that is often reversible either spontaneously or with treatment. causes recurrent episodes of wheezing, breathlessness, chest tightness and cough, particularly at night and in the early morning.

8
Diagnosis HISTORY Wheezing - high-pitched whistling sounds when breathing out (A normal chest examination does not exclude asthma). History of any of the following: cough, worse particularly at night/early morning recurrent wheeze recurrent difficulty in breathing recurrent chest tightness Note: Eczema, hay fever, or a family history of asthma or atopic diseases is often associated with asthma.

9
Precipitating factor: Symptoms occurs or worsen in presence of: Exercise respiratory tract infection animals smoke (tobacco, wood) pollen changes in temperature aerosol chemicals drugs (aspirin, beta blockers) dust mites (in mattress, pillows, upholstered furniture, carpets) strong emotional expression (laughing or crying hard)
 pollen changes in temperature aerosol chemicals drugs (aspirin, beta blockers) dust mites (in mattress, pillows, upholstered furniture, carpets) strong emotional expression (laughing or crying hard)")
10
Symptoms respond to anti-asthmatic therapy Patient’s cold ‘go to the chest’ or take more than 10 days to clear up

11
Lung Function Test 1.Spirometry -For confirmation of diagnosis -Measure the severity of air flow limitation and its reversibility -Increase in FEV1 of ≥12% and ≥ 200ml after administration of a bronchodilator indicates reversible airflow limitation consistent with asthma 2.PEF -For diagnosis and monitoring -PEF measurement ideally compared to the patient’s own previous best measurement -An improvement of 60L/min, or ≥20% of the pre- bronchodilator PEF after inhalation of a bronchodilator -Diurnal variation in PEF more than 20% (with twice daily readings, more than 10%)
")
12
Pefr chart

13
Other test: Measurement of airway responsiveness to metacholamine and histamine Indirect challenge test i.e. inhaled mannitol Exercise challenge test Skin test

14
Management and prevention 4 components to achieve and maintain control: 1.Develop patient-doctor relationship 2.Identify and reduce exposure to risk factor 3.Assess, treat and monitor asthma 4.Management of exacerbation

15
1. Develop patient-doctor relationship Development of partnership between patient and health care team Avoid exposure to risk factor Take medication correctly Understand different between controller/reliever Monitor symptoms, if relevant PEF Recognize symptoms that asthma is worsening and take action Seek medical advice as appropriate

16
2. Identify and reduce exposure to risk factor Domestic mites – mattress encasing Furred animal – remove from house Outdoor allergen – close door and window Indoor air pollutant – avoid passive and active smoking Occupational exposure Food allergy Avoid drugs – aspirin, NSAIDs, B blocker Obesity – weight reduction

17
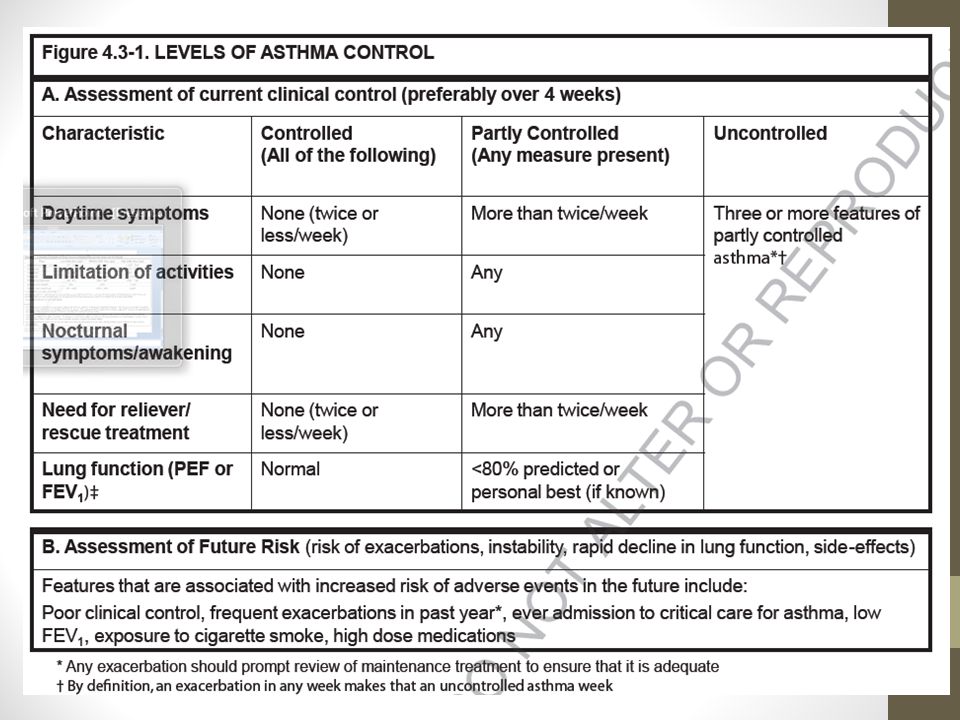
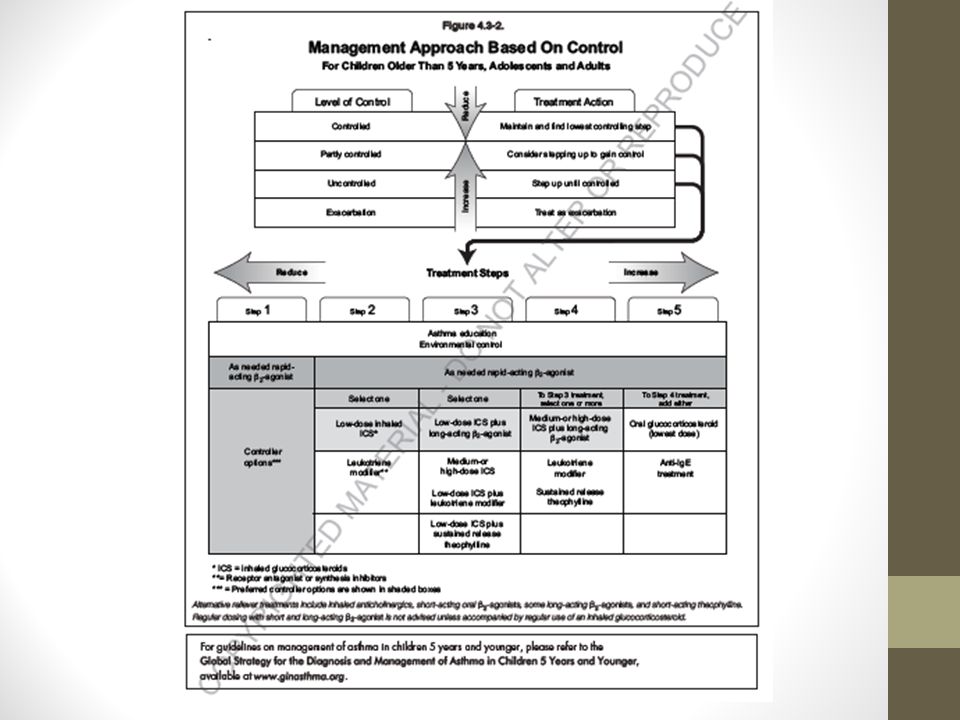
3. Assess, treat and monitor asthma Asthma is controlled when: Patient can prevent most attack Avoid troublesome symptoms day and night Keep physically active Good control is important reduce risk of exacerbation

20
Difficult to treat Patient who do not reach an acceptable level of control at step 4 Symptoms not control in spite of reliever + ≥2 controllers Consider: Diagnosis, Compliance, Smoking, Comorbidities Focus on achieving the best level of control

21
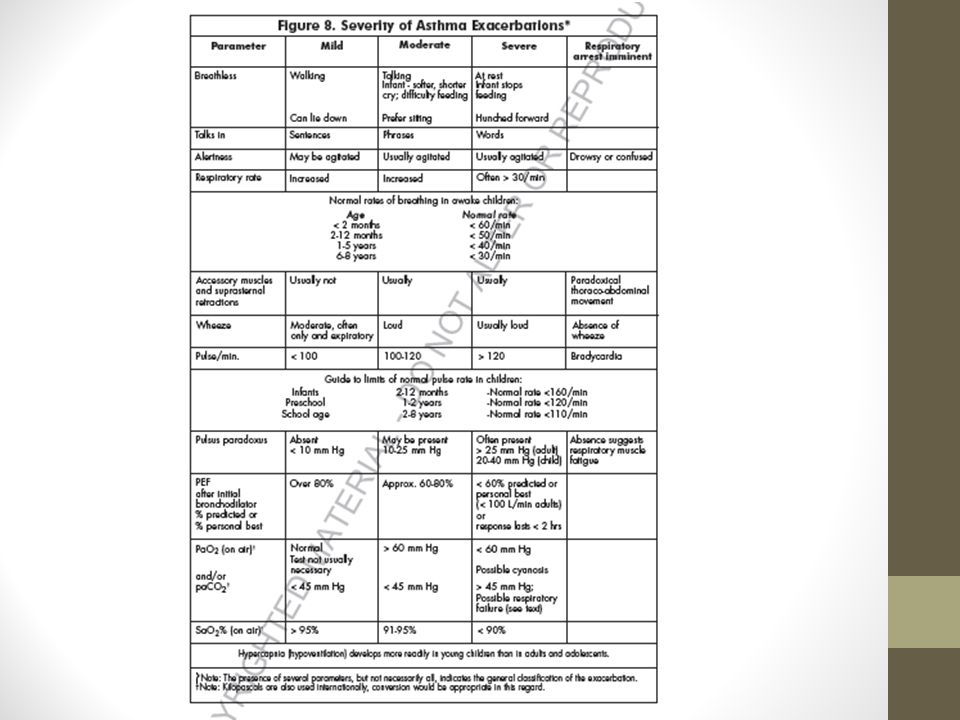
4. Management of asthma exacerbation Exacerbation? Episodes of progressive increase in SOB, cough, wheezing, chest tightness Characterized by reduced in expiratory airflow, as measured by FEV1 and PEF

23
High risk for asthma-related death History of near-fatal requiring intubation / mechanical ventilation Had history of emergency visit or hospitalization for asthma in the past year Not currently using inhaled corticosteroid Currently using / have recently stopped using oral glucocorticosteroid Over-dependent on rapid-acting inhaled beta2- agonist, esp those who use >1 canister monthly History of psychiatric disease / psychosocial problem History of non-compliance to asthma medication

25
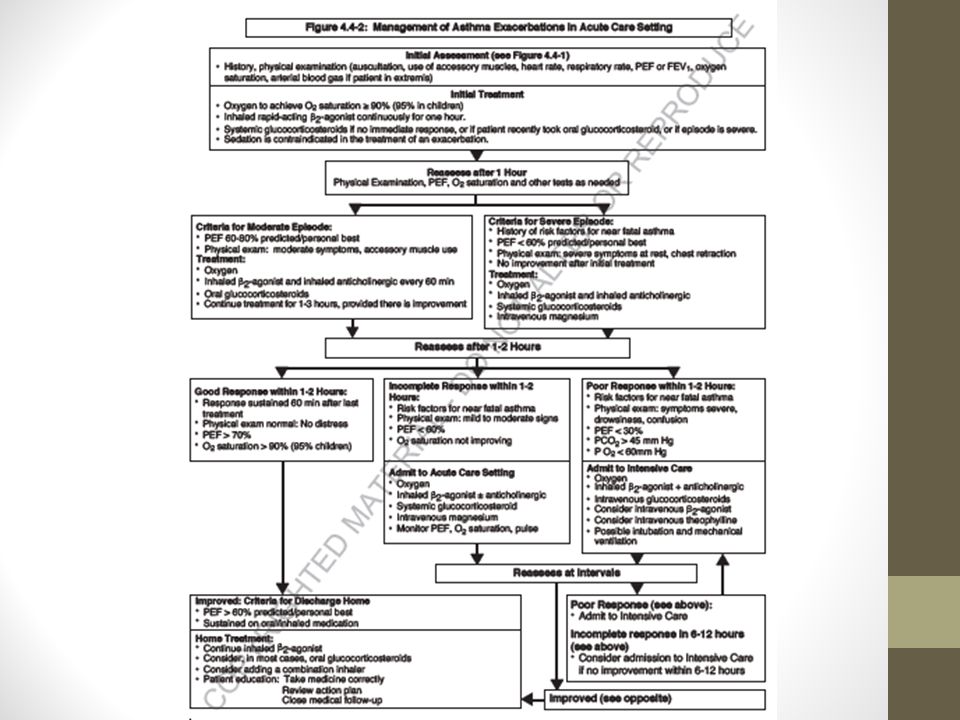
TREATMENT OF EXACERBATION MANAGEMENT IN COMMUNITY SETTING MANAGEMENT IN ACUTE CARE

26
BronchodilatorOral glucocorticosteroid -Administration of rapid acting inhaled B2 agonist -Mild attack - 2-4puffs every 3-4hr -Moderate attack – 6-10puffs every 1- 2hr -Oral prednisolone (0.5-1mg/kg) to treat exacerbation MANAGEMENT IN COMMUNITY SETTNG
 to treat exacerbation MANAGEMENT IN COMMUNITY SETTNG")
27
-Oxygen therapy -Aim SPO2 >95% -SPO2<92% good predictor of the need for hospital admission -ABG: paO2 45mmHg) indicates respiratory failure MANAGEMENT IN ACUTE CARE
 indicates respiratory failure MANAGEMENT IN ACUTE CARE")
28
Rapid acting inhaled B2 agonist Administer at regular intervals by MDI or spacer device Intermittent vs continuous neb no significant difference in bronchodilator effect / hospital admission Reasonable aproach initial use of continuous therapy, followed by intermittent on demand therapy

29
Additional bronchodilator Ipratropium bromide Anti-cholinergic Combination of nebulized B2 agonist with anti-cholinergic may produce better bronchodilation than either drug alone Theophylline Minimal role because the effectiveness and relative safety of rapid acting B2 agonist Associated with severe and potentially fatal side effect (in patient with long term therapy with theophylline)
")
30
Systemic glucocorticosteroid Speeds resolution of exacerbation Should be utilized in all cases, esp: Initial rapid acting inhaled B2 agonist therapy fails to achieve lasting improvement The exacerbation develops even though the patient was already taking oral glucocorticosteroid Previous exacerbations required oral glucocorticosteroid Oral vs iv equally effective Course: 7days vs 14days No need to taper down as long as pt on inhaled corticosteroid

31
Inhaled corticosteroid Effective therapy for exacerbation Combination of high dose inhaled glucocorticosteroid and salbutamol in acute asthma provide greater bronchodilation than salbutamol alone Effective for prevent relapse Discharge with prednisolone and inhaled budesonide lower rate of relapse

32
Magnesium sulphate IV MgSO4 2g infusion over 20min Reduce hosp admission rates in certain patient

33
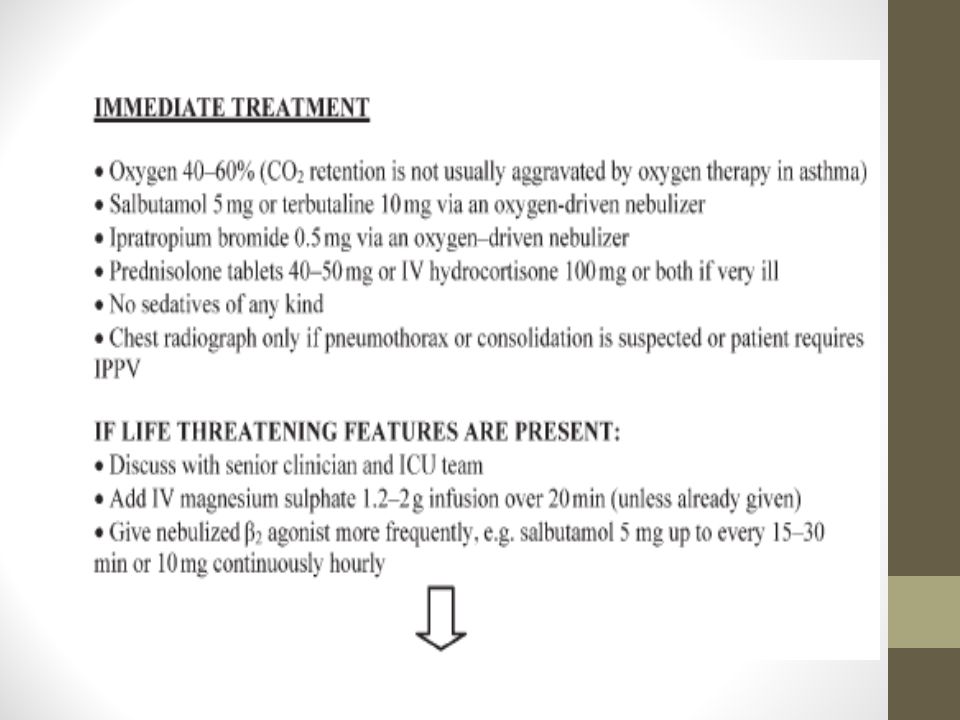
Life threatening asthma

34
Initial mx Rapid ABC assessment Oxygen therapy Correct hypoxemia with high concentrations of inspired oxygen Aim spo2> 92%

35
Nebulized B2 agonist Short acting B2 agonist should be given repeatedly in 5mg doses or by continuous neb or 10mg/hr driven by oxygen Administration should continue until there is significant clinical response or serious side effects

36
Nebulized ipratropium bromide Added to nebulized B2 agonist (500mcg 4hly) Produce significant greater bronchodilator than B2 agonist alone
 Produce significant greater bronchodilator than B2 agonist alone")
37
Steroids Systemic steroids in adequate doses should as early as possible (tables/intravenous) as it may improve survival Inhaled/nebulized steroids do not provide additional additional benefit
 as it may improve survival Inhaled/nebulized steroids do not provide additional additional benefit")
38
Iv MgSO4 Is a smooth muscle relaxant, producing bronchodilator Single dose 1.2-2g over 20min shown to be safe and effective in acute severe asthma Rapid administration may a/w hypotension

39
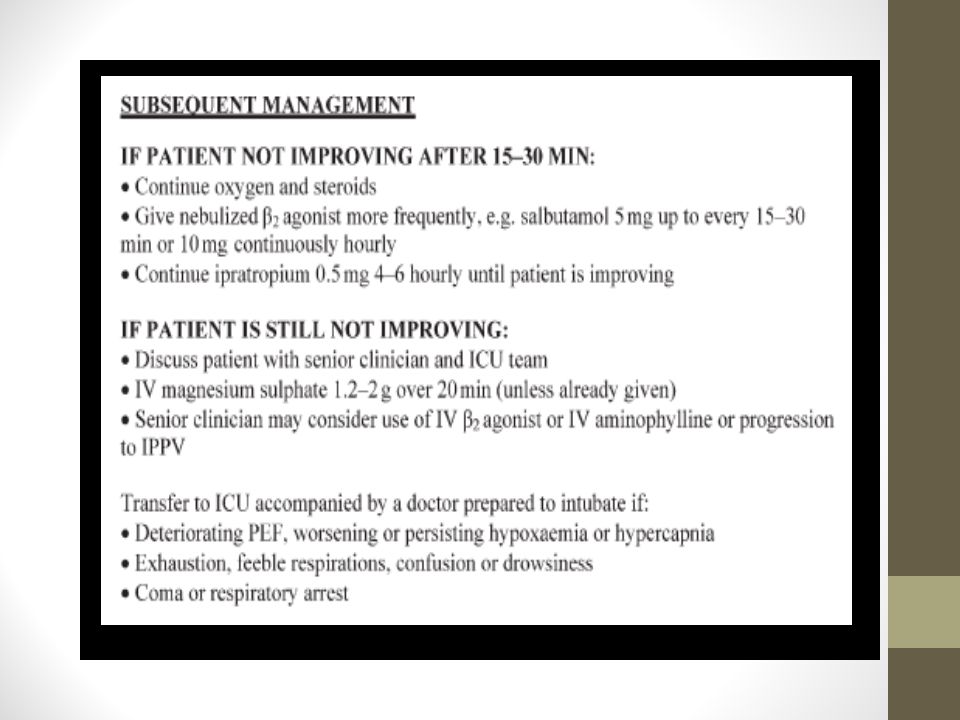
Iv bronchodilator Should be considered in ventilated pt and those with life threatening asthma Iv salbutamol 5-20mcg/min or terbutaline 0.05mcg/min should be titrated to response Lactic acidosis will develop on 70% of patients after 2-4hr therapy In extremis, salbutamol 100mcg can be given iv bolus or via ETT

40
Epinephrine Should be considered in pt not responding adequately to measure outlined above Route: s/c 0.3-0.4ml 1:1000 every 20min for 3 doses Neb 2-4ml of 1% solution hly Iv 0.2-1mg bolus 1-10mcg/min

41
Who should be intubated & when & how should mechanical ventilation be initiated? Bed side assessment based on assessment of risk and benefits Absolute indications: Coma Respiratory collapse / cardiac arrest Severe refractory hypoxemia

42
Relative indications not response to initial mx Fatigue Somnolence Cardiovascular compromise Development of pneumothorax

43
Intubation Place large ETT (≥7.5 for female, ≥8 for male) To facilitate suctioning of mucus plugs and reduce airway resistance Bags slowly to reduce auto-peep Sedation and often paralysis is necessary during and after intubation
 To facilitate suctioning of mucus plugs and reduce airway resistance Bags slowly to reduce auto-peep Sedation and often paralysis is necessary during and after intubation")
44
Mechanical ventilation Aim Achieve adequate oxygenation Avoid lung hyperinflation Buy time for medical mx to work

45
Recommended initial settings RR 10-14/min Vt 6-8mls/kg Minute ventilation 8-10L/min PEEP 0cm/H20 Inspiratory flow 100Ls I:E ≥1:3 FiO2 1.0

46
Keep Pplat <30cm H2O Keep PEEPi <12 cm H2O Allow permissive hypercarbia

47
Sedation Ketamine Propofol Fentanyl Midazolam Neuromuscular blockade -Rocuronium / pancuronium

48
Extubation Once airway resistance starts to fall & PaO2 normalizes, paralytic agents and sedatives should be withheld in anticipation of extubation

51
References GINA Management of life threatening asthma in adults David Stanley MRCP FRCA William Tunniciffe FRCP Bedside icu handbook

Similar presentations

>")
 Airway.>")
 Asthma GP monitoring Guideline 2) Asthma Diagnosis Guideline 3) Acute asthma.>")




 -based on the recognition of a characteristic pattern of symptoms and signs and the absence of an alternative.>")





 Diagnosis and management of chronic asthma in line with current BTS guidelines (Dr Lowery) 3 x Case.>")




