Download presentation
Presentation is loading. Please wait.

1
Dolphins and cows Neal Maskrey / Jonathan Underhill
National Prescribing Centre Liverpool UK

2
what should we be doing differently?
why evidence-based practice doesn’t happen as often as it sometimes should what should we be doing differently?

5
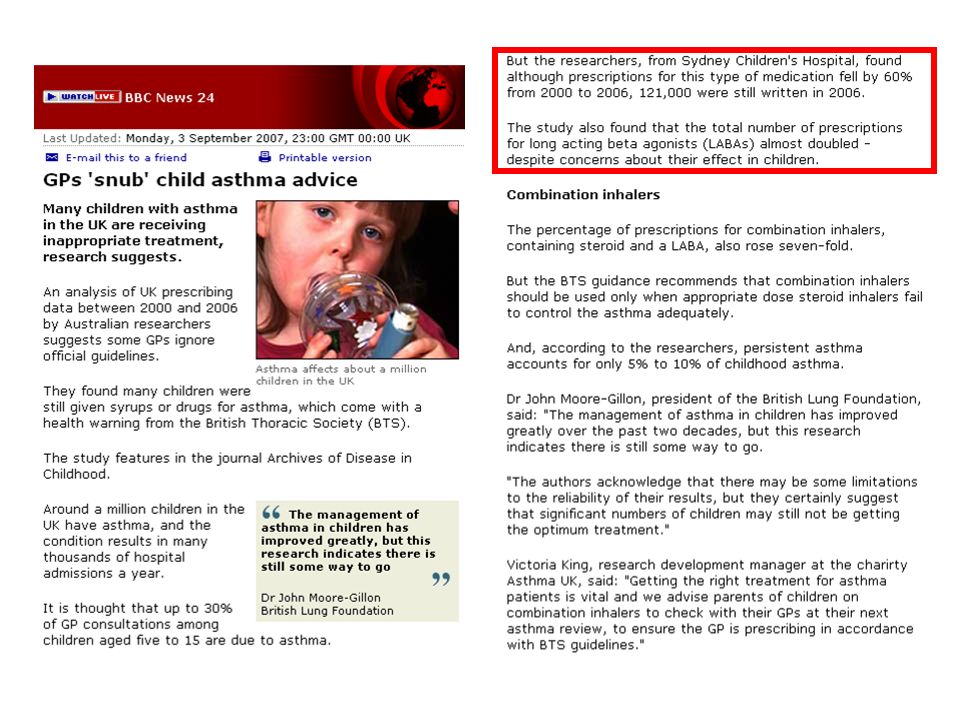
BTS/SIGN Asthma guidelines 2004, 2005, 2007
BTS Asthma guidelines 1997 BNF says “but inhalation preferred” BNF for children “not recommended” BTS/SIGN Asthma guidelines 2004, 2005, 2007

7
The doxazosin arm of ALLHAT
The doxazosin arm of ALLHAT? Hypertension 2003; 42: , Ann Intern Med 2002; 137: , JAMA 2000; 283: Increased risk of stroke (RR 1.26), combined CVD (RR 1.20) and heart failure (RR 1.80) with doxazosin The ALLHAT Study also included an alpha blocker arm. However, because of an apparent excess risk of CVD in this groups, this arm was stopped early. Final analysis confimred an increased risk of CVD and heart failure, without any difference for the primary outcome of coronary death/ MI.
, combined CVD (RR 1.20) and heart failure (RR 1.80) with doxazosin. The ALLHAT Study also included an alpha blocker arm. However, because of an apparent excess risk of CVD in this groups, this arm was stopped early. Final analysis confimred an increased risk of CVD and heart failure, without any difference for the primary outcome of coronary death/ MI.")
8
Prescribing of alpha-blockers in the US following ALLHAT Stafford RS, et al. JAMA 2004; 291: 54-62
In the US, active marketing of doxazosin was stopped and the amount prescribed reduced appropriately.

9
ALLHAT (doxazosin arm)
PUBLISHED Bu this was not the case in the UK, where doxazosin prescribing continued to increase…

10
Trends in the prescribing of alpha blocking drugs in England
……..and is still doing so. Remember, that guidelines now place alpha-blockers as at least a 4th line measure for treatment of hypertension. There are of course caveats with this prescribing data – prescribing for benign prostatic hypertrophy being the major confounder – but they have BPH in the States too.

11
Cox IIs MeReC Briefing 2002; 20
The GI safety of rofecoxib and celecoxib has been assessed in large clinical outcome trials which, on first analysis, show benefits over non-selective NSAIDs in the incidence of serious upper GI complications. However, longer-term GI data from the celecoxib study (CLASS) and cardiovascular adverse event data from the rofecoxib study (VIGOR) have questioned the risk/benefit profile of these new drugs and, until they are better understood, it seems sensible not to use them routinely in large numbers of people.
 and cardiovascular adverse event data from the rofecoxib study (VIGOR) have questioned the risk/benefit profile of these new drugs and, until they are better understood, it seems sensible not to use them routinely in large numbers of people.")
12
Trends in Prescribing of NSAIDs in General Practice in England
Well, some people may have taken notice, but this data seems to indicate that lots didn’t. The lilac coloured bar is rofecoxib which was of course withdrawn voluntarily following increased CV event rates, and the peach bar is celecoxib which increased following the rofecoxib withdrawal and which then fell away again as the MHRA issued warnings about cardiovascular risks of all coxibs. All this is still subject to litigation but calculations of the numbers of avoidable or premature heart attacks associated with the prescribing of these agents is more than 100,000 in the USA alone. 12

13
MeReC Extra 30 November 2007 NSAIDs - GI and CV risk
Long-term, randomised controlled trials (RCTs) have demonstrated that coxibs cause a small increased risk of thrombotic events in comparison with placebo. The excess risk was estimated to be about three cases per 1000 users treated for one year. This risk appears to increase with dose and persists throughout treatment.
 have demonstrated that coxibs cause a small increased risk of thrombotic events in comparison with placebo. The excess risk was estimated to be about three cases per 1000 users treated for one year. This risk appears to increase with dose and persists throughout treatment.")
14
….following a review of the evidence in October 2006, the Commission on Human Medicines (CHM) advised that there was sufficient evidence to suggest that traditional NSAIDs may also be associated with a small increased risk of thrombotic events when used at high doses and for long-term treatment. Furthermore, they identified that not all traditional NSAIDS carried the same CV risk: Naproxen 1000mg/day may be associated with a lower risk of thrombotic events than coxibs. Ibuprofen …..at low doses (e.g. 1200mg/day) …. does not suggest an increase [in] thrombotic risk Diclofenac 150mg/day has a thrombotic risk profile similar to that of etoricoxib▼ 60/90mg, and possibly other coxibs.
 …. does not suggest an increase [in] thrombotic risk. Diclofenac 150mg/day has a thrombotic risk profile similar to that of etoricoxib▼ 60/90mg, and possibly other coxibs.")
15
Diclofenac accounted for 46% of all NSAID prescribing …in primary care in England ……. If the excess risk for CV events is the same as COX-2 inhibitors (3 per 1000 patients per year) then approximately 2000 additional or premature CV events per year could be caused by diclofenac prescribing, compared with no treatment.
 then approximately 2000 additional or premature CV events per year could be caused by diclofenac prescribing, compared with no treatment.")
17
#1 However good the information is, on its own it is
usually insufficient to change practice

18
Work harder Be more effective Be imaginative and try some new things

19
1. Work harder I’m not working hard enough My workload is just right
I’m working too hard

20
Without innovation, public services costs tend to rise faster than the rest of the economy. Without innovation, the inevitable pressure to contain costs can only be met by forcing already stretched staff to work harder. Mulgan G & Albury D (2003). Innovation in the Public Sector. Strategy Unit, London.
. Innovation in the Public Sector. Strategy Unit, London.")
21
#2 It’s hard to find NHS workers who have substantial spare capacity

22
2. Be more effective

23
2003 1994 2007

24
Summary of recommendations
Incentive scheme for all practices Better co-ordination of resources promoting rational prescribing Better information Education Audit Formularies and guidelines Use skills of community pharmacists Practice visits should be better targeted, more focussed, effectively followed up Summarise information for prescribers Improve local consensus Involve and educate patients

25
The median effect size overall was approximately 10% improvement in absolute terms. Grimshaw J, et al. Implementing clinical guidelines: current evidence and future implications: Journal of Continuing Education in the health professions 2004; 24: S31-S37. The only factors that had a significant relationship with implementation of these important prescribing changes were an innovative approach among the doctors (most practitioners were cautious of change), and fundholding status. Salisbury C, et al. The implementation of evidence-based medicine in general practice prescribing. BJGP 1998; 48; 102 trials of educational interventions in the health care professions published between 1970 and 1993 inclusive. Dissemination-only strategies, such as conferences or the mailing of unsolicited materials, demonstrated little or no changes in health professional behaviour or health outcome when used alone. More complex interventions, such as the use of outreach visits or local opinion leaders, ranged from ineffective to highly effective but were most often moderately effective (resulting in reductions of 20% to 50% in the incidence of inappropriate performance). Oxman AD, et al. CMAJ 1995; 153: Grimshaw J, et al. Implementing clinical guidelines: current evidence and future implications: Journal of Continuing Education in the health professions 2004; 24: S31-S37. One of the most common findings from health services research is a failure to routinely translate research findings into daily practice. Previous systematic reviews of strategies to promote the uptake of research findings suffered from a range of methodologic problems that have been addressed in a more recent systematic review of guideline dissemination and implementation strategies. Changes in practitioner behavior; in the desired direction, were reported in 86% of the comparisons made. The median effect size overall was approximately 10% improvement in absolute terms. The review suggests that interventions that were previously thought to be ineffective (e.g., dissemination of educational materials) may have modest but worthwhile benefits. Also, multifaceted interventions, previously thought to be more effective than single interventions, were found to be no more effective than single interventions. Overall, there is an imperfect evidence base for decision makers to work from. Many studies had methodologic weaknesses, and reporting of this kind of research is generally poor, making the generalizability of study findings frequently uncertain. A better theoretical underpinning of studies would make this body of research more useful.
, and fundholding status. Salisbury C, et al. The implementation of evidence-based medicine in general practice prescribing. BJGP 1998; 48; trials of educational interventions in the health care professions published between 1970 and 1993 inclusive. Dissemination-only strategies, such as conferences or the mailing of unsolicited materials, demonstrated little or no changes in health professional behaviour or health outcome when used alone. More complex interventions, such as the use of outreach visits or local opinion leaders, ranged from ineffective to highly effective but were most often moderately effective (resulting in reductions of 20% to 50% in the incidence of inappropriate performance). Oxman AD, et al. CMAJ 1995; 153: Grimshaw J, et al. Implementing clinical guidelines: current evidence and future implications: Journal of Continuing Education in the health professions 2004; 24: S31-S37. One of the most common findings from health services research is a failure to routinely translate research findings into daily practice. Previous systematic reviews of strategies to promote the uptake of research findings suffered from a range of methodologic problems that have been addressed in a more recent systematic review of guideline dissemination and implementation strategies. Changes in practitioner behavior; in the desired direction, were reported in 86% of the comparisons made. The median effect size overall was approximately 10% improvement in absolute terms. The review suggests that interventions that were previously thought to be ineffective (e.g., dissemination of educational materials) may have modest but worthwhile benefits. Also, multifaceted interventions, previously thought to be more effective than single interventions, were found to be no more effective than single interventions. Overall, there is an imperfect evidence base for decision makers to work from. Many studies had methodologic weaknesses, and reporting of this kind of research is generally poor, making the generalizability of study findings frequently uncertain. A better theoretical underpinning of studies would make this body of research more useful.")
26
#3 If it was possible to deliver implementation
strategies with 100% effectiveness, the best results we could expect are a shift in the desired direction of 10-50%.

27
Let it happen Help it happen Make it happen
Greenhalgh T, et al. NCCSDO. April 2004 Let it happen Help it happen Make it happen Marketing: based on health promotion and social marketing theories. Attractive product, adapted to local needs (after assessment). Stepwise approach, multiple channels for communication Educational: based on adult learning theories. Focus on internal motivation of professionals. Bottom up, PBL, small interactive groups Epidemiological: based on rational, cognitive theories; information. Guideline development; dissemination via courses, journals, mailing
. Stepwise approach, multiple channels for communication. Educational: based on adult learning theories. Focus on internal motivation of professionals. Bottom up, PBL, small interactive groups. Epidemiological: based on rational, cognitive theories; information. Guideline development; dissemination via courses, journals, mailing.")
28
Let it happen Help it happen Make it happen
Social interaction: based on social learning and innovation theories, social influence and power theories. Peer review in local networks, outreach visits, opinion leaders, patient mediated interventions Organisational: based on management & system theories. Create structural and organisational conditions to improve care. Re-engineering care processes, TQM, team building, leadership. Behavioural: based on learning theory. Control performance by audit, feedback, reminder systems, £, sanctions. Coercive: based on economic, power and learning theories. Regulations, budgeting, contracting.

29
#4 The NHS mostly does things to clinicians,
rather than helping them acquire for themselves the knowledge, skills and attitudes to do a better job

30
The NHS professional bureaucracy
Front line staff have a large measure of control over decisions Hierarchical directives issued by those nominally in control often have limited impact – even resisted Negotiation, not imposition Collegial influences – credibility of professionals at their core, not simply those in formal positions of “authority” Mintzberg H. The Structuring of Organisations: a synthesis of research. 1979

31
3. Be imaginative

32
information management
cognitive psychology explaining risks and benefits to patients

33
information management
So let’s start, as we did, with Information Management. information management

35
information management
Volume of published material is unmanageable Reading is haphazard Formal CPD is haphazard

36
"We surveyed one acute medical take in our hospital
"We surveyed one acute medical take in our hospital. In a relatively quiet take, we saw 18 patients with a total of 44 diagnoses. The guidelines that the on call physician should have read remembered and applied correctly for those conditions came to 3679 pages. This number included only NICE, the Royal Colleges and major societies from the last 3 years. If it takes 2 min to read each page, the physician on call will have to spend 122h reading to keep abreast of the guidelines" (for one 24h on-call period). Allen D, Harkins KJ. Lancet 2005; 365: 1768
. Allen D, Harkins KJ. Lancet 2005; 365:")
37
More reading? Potential journals 10,000
Potential new articles per week 40,000 Even if 97% are not relevant (no POOs) 1,200 Time to read each article 15minutes 10h a day, 6 days a week = articles. So at the end of the first week you are about 4 weeks behind in your reading. At the end of the first month, you are 4 months behind in your reading. And at the end of the first year you are almost 5 years behind in your reading.
 1,200. Time to read each article 15minutes. 10h a day, 6 days a week = 240 articles. So at the end of the first week you are about 4 weeks behind in your reading. At the end of the first month, you are 4 months behind in your reading. And at the end of the first year you are almost 5 years behind in your reading.")
39
Effect of exercise on pain in knee OA Roddy E, et al
Effect of exercise on pain in knee OA Roddy E, et al. Ann Rheum Dis 2005; 64: 544-8 There is reasonable evidence to support the use of exercise in patients with knee osteoarthritis. This systematic review considered RCTs of trials of exercise against non-exercise Both aerobic walking and home based quadriceps strengthening exercise reduce pain and disability (data not shown) from knee osteoarthritis.
 from knee osteoarthritis.")
40
Clinician reading journals
Evidence-based treatment for the patient Clinician reading journals

41
Information Mastery requires two different approaches to managing information:
Foraging - a method of being alerted to new relevant, valid information when it is published Hunting - a method of finding information when it is needed NPC would add a third:- Hot-synching – clinicians rapidly checking once or, at the most, twice a year that their key approaches for the management of conditions they see commonly still match the best evidence DN Need a link on NPCi to Dave and Allen’s paper describing how to select a foraging service. Both clinicians and patients rate “keeping up to date” very highly. We discussed in the second workshop in this overview the information explosion and the resulting overload. The question is what tactics can be employed to manage the information. Two American professors – Dave Slawson and Allen Shaughnessy – came up with the Information Mastery concept and first published on it in They’ve described foraging as the first key approach. Everyone needs a service that alerts them to the key – and we’ll define the characterisitics that comprise “key” in a moment – the key new research in their specialty. Let’s use our NPC approach as an example. Five years ago we developed our own in house electronic currrent awareness bulletin. Our information scientist selected key websites with us – sites that would publish on a daily weekly, monthly or irregularly new developments relating to prescribing therapeutics and medicines management. So for example we’d capture policy developments as well as new clinical trials. We developed some selection criteria for the new information published on those sites…….and the service became so useful to us in-house that we rapidly made it available to anyone who wished to subscribe. We also devised some criteria for selecting the greatest hits of the daily digest and provide a weekly digest for those wanting a once a week update, rather than a once a day. More than 4,000 now subscribe. There are lots of services available that do this now for different audiences– and some are much better than others. As well as simple lists like our eCAB, there’s a need for a service that takes just the key new developments and both critically appraises the new data and sets those findings in the context of the rest of the evidence. We do that with our NPCi blog service – 2 or 3 key papers a week. The key feature of relying on foraging is that some one else – preferably a trusted public sector organisation – does the selection and critical appraisal for the subscribers. We don’t expect clinicians to read journals, select the papers to appraise and then incorporate the new data into their practice. We do the selection and appraisal, leaving clinicians to concentrate on what they need to do and are skilled at doing. This is a young science and developments are taking place all the time. We’ve recently recognised we need to put levels on evidence into the blogs, for example. As well as foraging, clinicians need an approach to finding information when its needed, when they are “stuck”. The appraoch need to be to finding the best answer , not just an answer. We’ll come to that in a minute. Over time, we’ve added a third approach – which links to a new and more logical approach to continuous professional development. It’s crazy to expect clinicians to be up to date with conditions they see rarely – the volume of material is too large to handle and by the time they see a condition its likely they’ll have forgotten what they learnt – or worse remembered what they learned incorrectly. So its unreasonable to expect a GP to know without checking how to manage hypertrophic cardiomyopathy, but entirely reasonable to expect a tertiary centre cardiologist to. Similarly, its unreasonable to expect a cardiologist to be up to date in managing depression in the postnatal period, but you’d expect a GP to be on the button. And yet the cardiologist ought to be spot on when managing depression in people after a heart attack. Multiple surveys have shown clinicians can spend a maximum of an hour a week keeping up to date. That’s enough time for a little foraging and then each year as a minimum hot synching. Hot synching is a term used in computing when one device connects to another and their memories update each other. I was describing the process of covering the key evidence in the 30 or so conditions a clinician sees commonly swiftly on a regular cycle when talking to some family medicine residents in the States and one of them said “You mean like hot synching” – and that’s exactly it. You’ll note we’ve designed NPCi specifically to enable hot synching for the common conditions in primary care and those topics as appropriate for some of the requirements of some specialist too. But with our resources we’re never going to be able to cover, for example lots of oncology because there are a hundred different cancers all with their own evidence base, or cover the requirements of orthopaedic hand surgeons, liver transplant teams and so on. But the same principles apply to people working in those fields.

42
Usefulness = Relevance x Validity Work
What are the criteria used when looking for the best answer or important evidence? Slawson DC and Shaughnessy AF. J Am Board Fam Pract 1999; 12: Usefulness = Relevance x Validity Work Dave and Allen recognised the three issues in using evidence – work, relevance and validity - when they came up with the usefulness equation.

43
How can we quickly spot what is NOT important to us?
Not RELEVANT Upstream to clinical decisions being made, e.g. animal or in vitro studies Study populations and / or settings do not reflect question type, practice population and settings Not VALID Poor study design Bias and confounding Measurement validity Insufficient power

44
So, filtering for relevance
Feasible (intervention) Outcomes (patient-orientated) Common (condition) Change in practice required
 Outcomes (patient-orientated) Common (condition) Change in practice required.")
45
Disease / condition DOO POO
DOOs can mislead and don’t always relate to POOs Ebell M, et al. Am Fam Physician 2004; 69: 548–56 Disease / condition DOO POO Doxazosin for BP In Blacks, reduces BP Increases mortality Lidocaine for arrhythmia after MI Suppresses arrhythmias Finasteride for BPH Improves urinary flow rate No clinically important change in patient symptom scores Arthroscopic surgery for OA knee Improves appearances after debridement No change in function or symptoms at 1 year Sleeping infants on their stomach or side Based on anatomy and physiology, will decrease risk of aspiration Increase in SIDS

46
Disease / condition DOO POO
Vitamin E for heart disease Reduces levels of free radicals No change in mortality HRT for CHD prevention Reduces LDL, increases HDL No decrease in CV or all cause mortality, increase in CV events over 60 years Insulin for PWT2D Keeps blood glucose below 6.7mmol/L No reduction in mortality Sodium fluoride for fracture prevention Increases bone density Does not reduce fracture rate Lidocaine prophylaxis after MI Suppresses arrhythmias Increases mortality Beta blockers for heart failure Reduce cardiac output Reduce mortality

47
If the answer to any of those is “no”
I don’t know and I don’t care

48
After checking it is relevant, is the answer likely to be valid?
How to quickly spot the fatal flaws: Is it a high level of evidence? Is it statistically significant? Is it clinically significant?: Do you understand what the the numbers tell you? Absolute vs. relative risk vs. NNT Was there enough people in the study for long enough? Was the allocation concealed?

49
Reading and critical appraisal MUST (largely) be replaced by reading pre-digested sources of evidence from trusted sources
 be replaced by reading pre-digested sources of evidence from trusted sources")
50
Be an Information Master! Slawson DC and Shaughnessy AF
InfoRetriever, DrCompanion, self-assembly Cochrane Library NICE, (NSFs) Usefulness Clinical Evidence InfoPOEMs, Prodigy BestTreatments NPC ref sheets EBM DTB MeReC Bandolier “Ivy League” journals Textbooks Medline
 Usefulness. Clinical Evidence. InfoPOEMs, Prodigy. BestTreatments. NPC ref sheets. EBM DTB MeReC. Bandolier. Ivy League journals. Textbooks. Medline.")
51
The five S approach Haynes RB. Evidence-Based Medicine 2006;11:162-4
NPCi therapeutics floors, Clinical Evidence, CKS (PRODIGY), etc NPCi blogs and podcasts, EBM, ACP Journal Club, etc Cochrane reviews, HTAs, NICE full guidelines, etc
, etc. NPCi blogs and podcasts, EBM, ACP Journal Club, etc. Cochrane reviews, HTAs, NICE full guidelines, etc.")
52
information management
Stop reading journals (to stay up to date) Read trusted summaries of evidence Concentrate CPD on the conditions you see commonly (c30 for a GP = two thirds of problems presenting)
 Read trusted summaries of evidence. Concentrate CPD on the conditions you see commonly (c30 for a GP = two thirds of problems presenting)")
53
#5 Information management is nowhere near being a
key component of undergraduate or postgraduate curricula – yet without it how can we expect clinicians to be up to date?

55
Comments / Questions

Similar presentations

















>")






