Download presentation
Presentation is loading. Please wait.

1
Red urine Hemoglobinuria Myoglobinuria Drugs (rifampicin),food
Inborn errors of metabolism(porphyria) Urate crystals Hematuria Do dipstick,microscopy (>5cells/ul in fresh uncentrifuged urine, >3 cells/HPF in centrifuged sediment.
 Urate crystals. Hematuria. Do dipstick,microscopy (>5cells/ul in fresh uncentrifuged urine, >3 cells/HPF in centrifuged sediment.")
2
Red if fresh(bladder), or brown color as Hb converted to acid haematin by urinary acids
Early hematuria:urethral cause Terminal hematuria:bladder cause Microscopy:dysmprhic RBC,RBC cast:glomerular bleeding Prevelance of % in school children

3
RBC casts

4
RBC casts

5
History Fever,urinary symptoms….infection
Colicky loin pain,lower tract symptoms…..renal calculus Rash,arthritis…HSP,SLE Preceding URTI…..PSGN,IgA nephropathy Coagulopathy,trauma,tumor,exercise FH of hematuria,deafness,renal failure…Alport O/E:HTN,kidneys,genitalia,rash

9
Investigations Urine protein/creat ratio EUC,albumin ASOT,C3,C4,ANA
FBC,clotting studies Urine calcium/creat ratio U/S ,XRAY,CT Urine analysis on parents IgA,cystoscopy Renal biobsy

10
Macroscopic hematuria
Most common cause is infection,then perineal irritation,trauma Viral infections,adenovirus 11,12 may cause hemorrhagic cystitis Exercise induced hematuria not associated with renal disease. Recurrent gross hematuria as IgA nephropathy,Alport,nut cracker (thin,loin pain,compression of renal vein bet aorta,SMA

11
Causes of hematuria 1.Glomerular causes Familial benign hematuria
GN:primary as postinfectious,MPGN,IgA nephropathy secondary GN as SLE,HSP. HUS,interstital nephritis,renal vein thrombosis,cystic renal disease Alport

12
Non glomerular causes UTI Hypercalcuria,renal calculi Trauma,exercise
Coagulpathy as sickle Vascular malformations Nut cracker syndrome Menarche Malignancy as nephroblastoma of the kidney or bladder tumors

13
Persistent MA without proteinuria :
1.Beningn familial hematuria 2.idiopathic hypercalcuria 3.IgA nephropathy 4.Alport syndrome

14
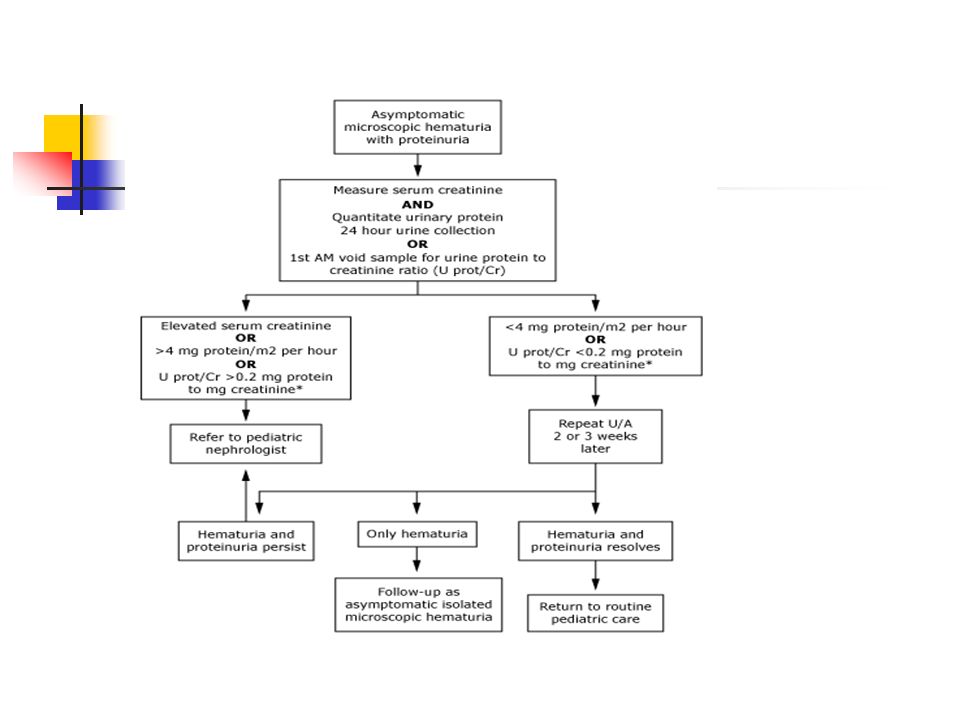
Figure 10-1 Algorithm for investigating hematuria.

16
Persistent MA without proteinuria :
1.Beningn familial hematuria 2.idiopathic hypercalcuria 3.IgA nephropathy 4.Alport syndrome

17
Alport Syndrome 80% XL,20% AR
Renal failure,sensorineural deafness higher frequencies,ocular changes(anterior lenticonus,retinal changes Present as micro and rarely macroscopic hematauria with URTI Proteinura,HTN later age

18
Diagnosis by EM:Thinning of GBM,split and duplicated lamina densa,basket weave
Males progress to ESRD,deafness by 30y ACEI may delay progression to ESRD Defiency of α5 of type 4 collagen

19
Benign Familial Hematuria(TBMN)
AD inheritance Present as microscopic hematuria,no proteinuria or renal failure EM:thinning of GBM Follow up for proteinuria,HTN

20
GBM in Alport syndrome

22
GBM in Alport syndrome

23
IgA nephropathy Recurrent macroscopic hematuria,loin pain 1-2 days following URTI,last < 3 days. Persistent microscopic hematuria ±proteinuria Nephritic,nephrotic syndrome rare Present second decade,more in males

24
Familial cases reported
IgA high in 35-50% Diagnosis:LM:focal or diffuse mesangial cell proliferation,expansion of mesangial matrix IM:IgA,C3 deposits Prognosis for children better than adults Young children without macroscopic hematuria have the best long term outcome

25
Heavy proteinuria is a risk factor for progression to ESKD.
Progression to ESRD is slow(25% need dialysis in 20y) Children with nephrotic syndrome are treated with steriods ACEI are used to delay progression,decrease proteinuria Fish oil
 Children with nephrotic syndrome are treated with steriods. ACEI are used to delay progression,decrease proteinuria. Fish oil.")
26
IF showing mesangial depostis

27
Normal glomerulus

28
IgA deposits

29
Thin glomerular basement membrane disease

31
PROTEINURIA DIPSTICK values
.trace (.15g/l),+1 (.3g/l),+2 (1g/l),+3 (3g/l),+4 (20g/l) False postive when urine concentarted,alkaline urine Children excrete 150 mg/day of protein or mg/m2/day 40 % of normal urinary protein is tissue rather than plasma as tamm-horsfall (a gp secreted in TALH ) Almost of the flitered smaller proteinare absorbed in the proximal CT.
,+1 (.3g/l),+2 (1g/l),+3 (3g/l),+4 (20g/l) False postive when urine concentarted,alkaline urine. Children excrete 150 mg/day of protein or mg/m2/day. 40 % of normal urinary protein is tissue rather than plasma as tamm-horsfall (a gp secreted in TALH ) Almost of the flitered smaller proteinare absorbed in the proximal CT.")
32
Protein-creatinine ratio to estimate protein excretion

33
Urine protein/creat ratio correlates with measurement of protein in 24 hour collection.
Most normal subjects have a ratio below.02 mg/umole (.2g/g) in above 2y,.05 in children 6-24 m Micoalbuminuria ranges mg albumin/g creat B2-microglobulin in urine indicates proximal tubular injury
 in above 2y,.05 in children 6-24 m. Micoalbuminuria ranges mg albumin/g creat. B2-microglobulin in urine indicates proximal tubular injury.")
34
Classification 1-Functional:seen in stress,fever,cold,exercise,CHF 2-Idiopathic transient or intermittent 3-postural:in adolesents,males,less than 2g/day,proteinuria in upright position but not when recumbent Decrease in amount with age Has a good outcome

35
4-pathologic:increase permeability of GBM,loss of anions(nephrotic,GN)
Loss of nephron mass:single kid,cystic disease from hyperfilteration secretory,overflow:UTI,in newborns as tam

Similar presentations



















 RENAL DISEASE: OVERVIEW AND ACUTE RENAL FAILURE Pathophysiology of Disease: Chapter 16 (388-394) Jack.>")


 Characteristics : Proteinuria ( urine protein loss > 2 gm/day ) Hypo-proteinemia ( serum albumin < 2.5 gm/dL ) Edema Hyperlipidemia.>")

