Download presentation
Presentation is loading. Please wait.

1
PROTEINURIA AND HEMATURIA ASHIK HAYAT M.D.

2
Proteinuria and Nephrotic Syndrome Occurrence of proteinuria in a single urine is relatively common. Will present in 5% to 15% of normal children in a random urine specimen.

3
-Proteinuria is a marker of renal disease. -The dilemma for the PCP is to differentiate the child with transient or any other benign forms of proteinuria from children with renal disease.

4
PATOPHYSIOLOGY AND CLASSIFICATION Normal protein excretion normal child <100 mg/m2/day or 150mg/day neonates is higher up to 300 mg/m2 (reduced reabsorption of filtered protein)
")
5
The normally low rate of urinary protein excretion is: -Restriction of the filtration -Reabsorption of freely filtered low molecular weight protein

6
Abnormal protein excretion Urinary protein excretion in excess of 100 mg/m2/day or 4mg/m2/hr Nephrotic range proteinuria is defined as >1000 mg/m2/day or 40mg/m2/hr

7
Three main mechanism: Glomerular (increase filtration) Tubular (increase excretion- decrease reabsorption) Overflow (marked overproduction of a particular protein)
 Tubular (increase excretion- decrease reabsorption) Overflow (marked overproduction of a particular protein)")
8
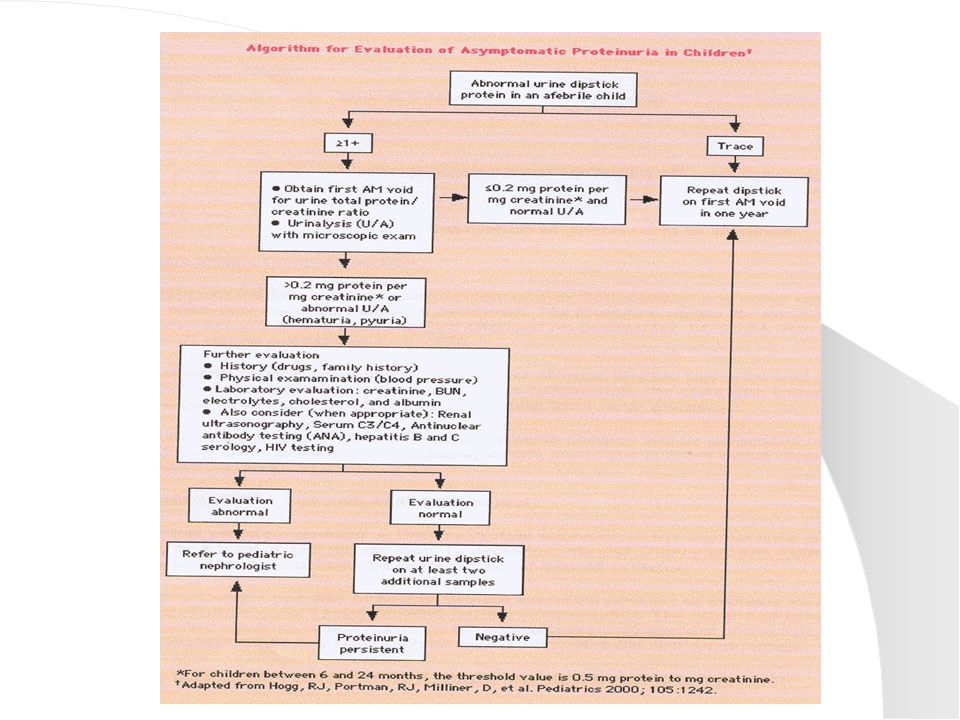
Measurement of urinary protein Urine dipstick negative trace between 15-30mg/dl 1+ 30-100 mg/dl 2+ 100-300mg/dl 3+ 300-1000mg/dl 4+ >1000mg/dl

9
Quantitative assessment Measurement of 24-hour protein excretion or total protein/creatinine ratio in a spot urine in the morning normal in children: <0.2mg protein/mg creatinine (+2 years) <0.5mg protein/mg creatinine (6-24-month)
 <0.5mg protein/mg creatinine (6-24-month)")
10
Qualitative assessment May be necessary to differentiate glomerular from tubular protein

11
Approach to the child with proteinuria Transient or Intermittent Orthostatic Persistent

13
History and physical Thorough history and physical change in urine volume or color edema increase BP recent strep infection family history for renal disease and hearing loss (Alport disease)
")
15
The Need for Renal Biopsy The key indication for biopsy in any renal disorder are the need to make specific diagnosis for therapeutic reasons or to provide a prognosis.

16
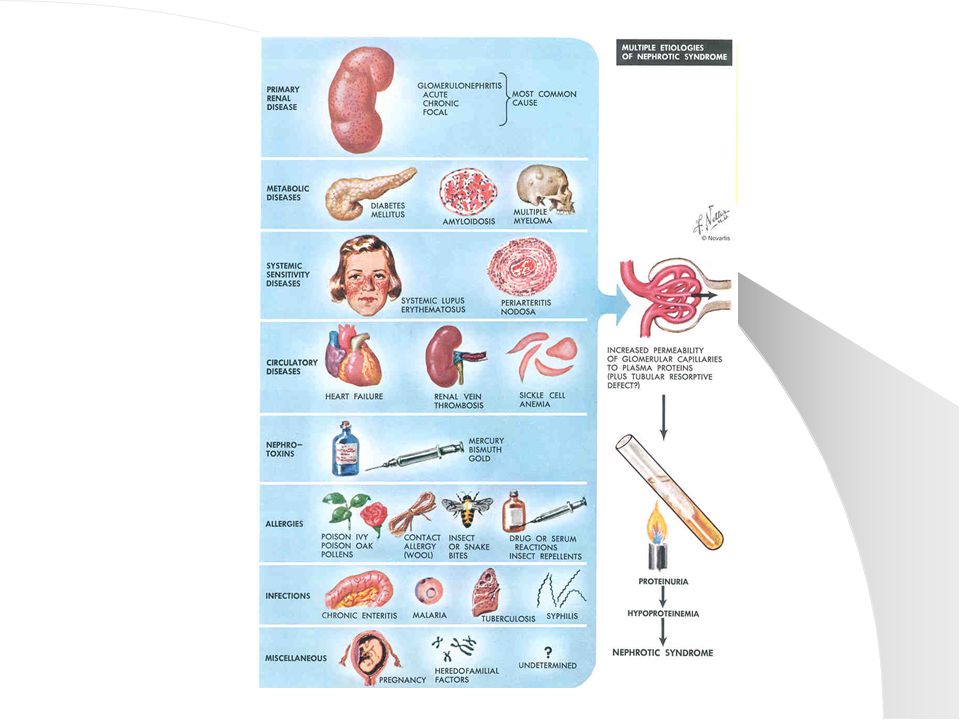
Neprotic Syndrome Nephrotic syndrome is characterized by massive proteinuria, hypoalbuminemia, edema, and hyperlipidemia; the most common presenting symptom is edema.

17
Introduction The annual incidence of Nephrotic syndrome in healthy children is 2 to 7 new case per 100,000 children younger than 18 years of age. The peak age lf onset is at 2 to 3 years.

18
Definition The diagnosis of NS is the presence of urinary protein, with the albumin disproportionately greater than globulin.

19
Clinical Diagnostic Criteria 1- Generalized edema 2- Hypoproteinemia <2 g/dL (disproportionately low albumin in relation to globulin)
")
20
3-Urine protein to urine creatinine ratio in excess of 2 (first A.M. void) or a 24- hour urine that exceeds 50mg/Kg body weight 4-Hypercholesterolemia (>200 mg/dL)
 or a 24- hour urine that exceeds 50mg/Kg body weight 4-Hypercholesterolemia (>200 mg/dL).")
23
The mechanisms for edema include: -Transudation of fluid from the intravascular space into the intestitium secondary to decreased albumin and - Increased renal tubular reabsorption of sodium and water

25
The hyperlipidemia is secondary to: -Increase in lipoprotein synthesis by the liver and -Decrease in lipid catabolism resulting from reduced activity of the enzyme lipoprotein lipase and lecithin cholesterol acetyltransferase.

26
INCIDENCE FOR UNDERLYING PATHOLOGY

30
TREATMENT

33
Complications One true complication of NS is the tendency to developed infections. IgG antibody is lost in the urine, and complement activation is impaired by concomitant loss of factor B.

34
Marked intravascular depletion causes diminished splachnic blood flow and hypoxia, and a marked tendency to thrombosis cause microinfarction, lowering resistance of the bowel wall to bacteria passage.

35
Peritonitis is a major contributor to the 1% to 2% mortality in NS The second major contributor is Thromboembolism, however anticoagulant therapy is not justified during remission.

36
Growth is often impaired in NS There may be losses of IGF-binding protein, which could account for the depressed serum concentration of IGF-I and IGF-II.

38
Prognosis Mortality in minimal-change NS is approximately 2% Of the remaining 98%, most are steroid- responsive about 2/3 experience1/3 possible single relapsedeveloping protracted series of relapses

39
Hematuria and Glomerulonephitis

40
Introduction Recognition, definition, differential diagnosis, and orderly evaluation of hematuria in infants and children is often an important issue in pediatric practice

41
Definition Hematuria is defined by the presence of an abnormal quantity of red blood cells in the urine Macroscopic: grossly visible Microscopic: only upon urinalysis >5-10 RBC’s per high power field

42
A large number of benign and serious conditions can cause hematuria in children.

43
Gross hematuria UTI Irritation of the meatus or perineum Trauma Nephrolithiasis Sickle cell disease/trait Post infectious glomerulonephritis IgA nephropathy

44
Microscopic hematuria Glomerulopathies Hypercalciuria Microlithiasis UTI

45
Children with hematuria may present in one of three way 1-Onset of gross hematuria 2-Onset of urinary or other symptoms with incidental finding 3-Incidental finding during a health evaluation

46
Historical clues The color of the urine Glomerulonephritis may be brown and/or frothy urine, while bleeding is suggested by the presence of blood clots, or pink or clearly red urine

47
The timing of the hematuria Initial (urethral bleeding) Terminal (bladder) Throughout (no localizing value)
 Terminal (bladder) Throughout (no localizing value)")
48
Circumstances associated History of trauma, pain, micturating symptoms, systemic signs including fever and skin and nasopharyngeal infection

49
Age of onset Periodicity Blood on diapers of underwear Exposure to medications Relation with exercise Flank pain (loin pain hematuria syndrome)
")
50
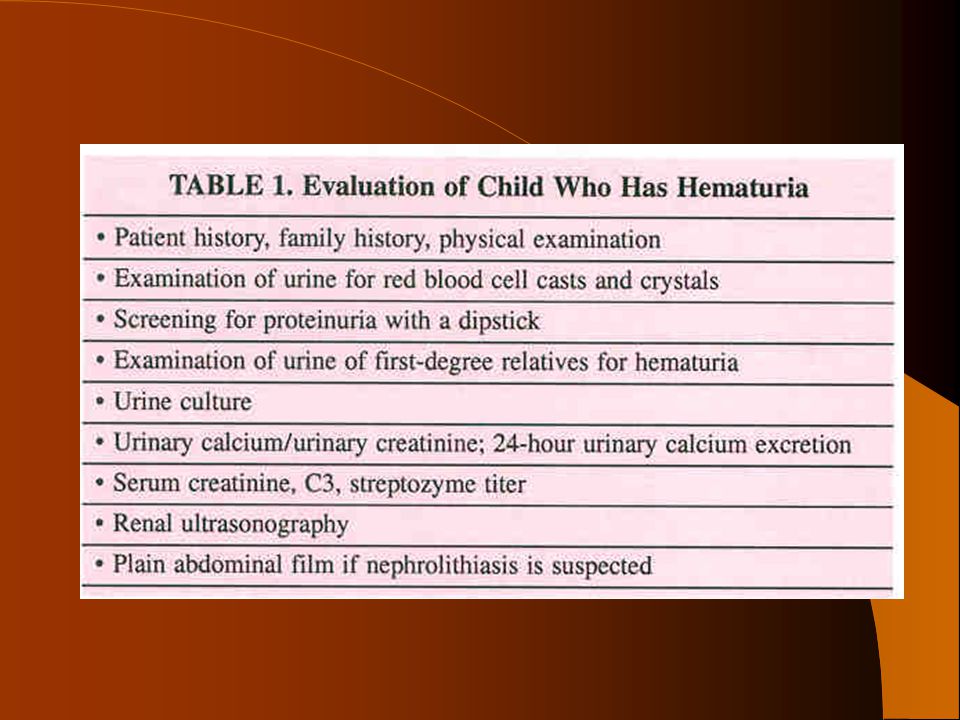
Physical examination Should Include Blood Pressure measurement Assessment for edema or weight gain Close skin examination Direct visualization of the genitals Abdominal mass or discomfort

51
Laboratory evaluation -Urinalysis, urine culture, and urinary excretion studies -Glomerular bleeding evaluation (24-hour urinary protein excretion/creatinine ratio, excretion of casts, protein excretion, blood clots)
")
52
Imaging studies USD of the kidney and bladder. Cytoscopy Is rarely indicated. May be useful to determine if the bleeding comes from bladder or one or both ureters.

54
Etiology The causes of gross and microscopic hematuria are extensive.

55
Anatomical abnormalities Bladder and kidney infection Coagulation/hematology Drugs Exercise Familial hematuria Glomerulonephritis Hypercalciuria-hyperuricosuria-urolithiasis Interstitial nephritis Trauma and tumors

56
Extrarrenal causes Usually gross hematuria, no proteinuria, and RBC’s that are suggestive of nonglomerular origin.

57
-Neprholithiasis -UTI -Adenovirus -Kidney tumor -Polycystic kidney -Urethral irritation

58
-Obstructive uropathy -Post-traumatic kidney -Onset of menarche -Exposure to cyclophosphamide -Thrombogenic condition -Sickle cell trait

59
-Vascular bleeding -”Nutcracker syndrome” -Left renal vein entrapment (Also orthostatic proteinuria) -Loin pain hematuria syndrome -Urethrovesical bleeding
 -Loin pain hematuria syndrome -Urethrovesical bleeding")
60
Renal Causes (Glomerular causes) Most patients also have proteinuria, red cell casts, and/or renal insufficiency. The clinical context is also suggestive.

61
-Postinfectious glomerulonephritis -Henoch-Schonlein purpura (tetrad: rash, arthralgias, abdominal pain and renal disease) -IgA nephropathy persistent -Alport Syndrome hematuria -Thin base membrane disease (heterozygote carrier)
 -IgA nephropathy persistent -Alport Syndrome hematuria -Thin base membrane disease (heterozygote carrier)")
62
-Systemic diseases Lupus Shunt nephritis Hemolitic-uremic syndrome

63
Unexplained hematuria -Factitious hematuria

67
Poststreptococcal glomerulonephritis The most common type in children results through immunologic process, from A Beta-hemolytic streptococcus.

69
Immunoglobulin A nephropathy The most common variety of primary glomerulonephritis. Usually negative family history. Mesangial IgA deposition is the most prominent finding on renal biopsy.

70
Alport Syndrome Its classically X-linked form, suggested by hematuria in a male. Positive family history of hematuria, deafness, and renal failure. Abnormal collagen IV composition.

71
Thin base membrane disease Also called benign familial hematuria, transmitted in a dominant fashion but, in most cases a heterozygous form of autosomal recessive Alport syndrome.

72
Treatment General management Salt and water restriction. Specific treatment Depends of the etiology or severity of the disorder.

Similar presentations















 Acute GN Definition (Hricik et al, 1998) Syndrome characterized by the abrupt onset of macroscopic hematuria; oliguria; acute renal failure; manifested.>")



>")













