Download presentation
Presentation is loading. Please wait.

1
The up-to-date evidence on colposcopy practice
Cancer Treatment Review (2006)32, The up-to-date evidence on colposcopy practice and treatment of cervical intraepithelial neoplasia : The cochrane colposcopy & cervical cytopathology collaborative group (C5 group) approach OBGY R4 Eun Suk Lee
32, The up-to-date evidence on colposcopy practice. and treatment of cervical intraepithelial neoplasia. : The cochrane colposcopy & cervical cytopathology. collaborative group (C5 group) approach. OBGY R4 Eun Suk Lee.")
2
Introduction Introduced early in the last century (1925) by Hinselman
Visualisation of the lower genital tract before and after applying an acetic acid solution under magnification with an appropriate light source

3
Colposcopy as a screening tool
Combination of cytology & colposcopy in primary screening to reduce the impact of false negative results of cytology Cervical cytology : reported by Georgios Papanicolaou (1943) Proven its efficacy during the last 50 years by reducing both incidence & mortality from cervical cancer False negative rate ☞ vary from 10% to 80% with an estimate of 20–25% being generally acceptable
 Proven its efficacy during the last 50 years by reducing both. incidence & mortality from cervical cancer. False negative rate ☞ vary from 10% to 80% with an estimate of 20–25% being generally acceptable.")
4
Colposcopy as a screening tool
Known prevalence of CIN in the general population(1–2%) False negative rate of cytology ☞ 20% In a total population of 10,000 women screened, 100 → pre-invasive lesion 80 → detected with cytology 20 → missed 9920 women ☞ referred & undergo colposcopic exam in order to detect the 20 missed ones Colposcopy in primary screening ☞ Expensive Time-consuming Requires extensive training Unnecessary psychological morbidity in women Long-term pregnancy-related morbidity Obvious Disadvantages
 False negative rate of cytology ☞ 20% In a total population of 10,000 women screened, 100 → pre-invasive lesion. 80 → detected with cytology. 20 → missed women ☞ referred & undergo colposcopic exam. in order to detect the 20 missed ones. Colposcopy in primary screening ☞ Expensive. Time-consuming. Requires extensive training. Unnecessary psychological morbidity in women. Long-term pregnancy-related morbidity. Obvious Disadvantages.")
5
Diagnostic accuracy of colposcopy
<Colposcopic findings> Unsatisfactory colposcopy (upper limit of transformation zone or squamous columnar junction not visible) Subtle (e.g. simple HPV infection) Normal (e.g. immature or metaplasia changes) Histological Dx ☞ punch bx or excision of transformation zone Diagnostic deficiencies of colposcopy : Colposcopic impression vs histological Dx In a series of 2100 women, Colposcopic & histological agreement only 37% ∴ Colposcopy → an excellent secondary test for cervical disease in women with abnormal cytology
 Subtle (e.g. simple HPV infection) Normal (e.g. immature or metaplasia changes) Histological Dx ☞ punch bx or excision of transformation zone. Diagnostic deficiencies of colposcopy. : Colposcopic impression vs histological Dx. In a series of 2100 women, Colposcopic & histological agreement only 37% ∴ Colposcopy → an excellent secondary test for cervical disease. in women with abnormal cytology.")
6
The HPV DNA testing, as a triage tool for colposcopic referral
10% of screened population ☞ borderline or minor cytological abnormalities (such as ASCUS, AGUS, LgSIL) on cervical smear 5–47% of lesions presenting c low grade cytological phenotype ☞ Reveal in histology an occult high grade CIN Management options : Immediate referral to colposcopy for every woman c minor findings in cytology Selection of those likely to have underlying high-grade ds Currently available triage methods Repeat cytology HPV DNA test
 on cervical smear. 5–47% of lesions presenting c low grade cytological phenotype. ☞ Reveal in histology an occult high grade CIN. Management options : Immediate referral to colposcopy. for every woman c minor findings in cytology. Selection of those likely to have underlying high-grade ds. Currently available triage methods Repeat cytology. HPV DNA test.")
7
The HPV DNA testing, as a triage tool for colposcopic referral
Recent meta-analysis by Arbyn et al. (2004) Accuracy of HPV DNA test & repeat cytology as triage methods for equivocal cytological findings (ASCUS/AGUS) & for an histological outcome of CIN II+ or CIN III+ HPV DNA test, in Hybrid Capture-2 (HC-2) Increased sensitivity (95%) vs repeat cytology (82%) Specificity : Low without statistically significant difference HC-2 (67%) vs Repeat Cytology (58%) The Conclusion : HPV DNA test → improved accuracy (higher sensitivity, similar specificity) Compared to repeat Pap smear
 Accuracy of HPV DNA test & repeat cytology as triage methods. for equivocal cytological findings (ASCUS/AGUS) & for an histological outcome of CIN II+ or CIN III+ HPV DNA test, in Hybrid Capture-2 (HC-2) Increased sensitivity (95%) vs repeat cytology (82%) Specificity : Low without statistically significant difference. HC-2 (67%) vs Repeat Cytology (58%) The Conclusion : HPV DNA test → improved accuracy. (higher sensitivity, similar specificity) Compared to repeat Pap smear.")
8
The HPV DNA testing, as a triage tool for colposcopic referral
HPV DNA testing in the triage of cases with low-grade cytology (i.e. HPV infection and CIN1) Sensitivity of HC-2 ☞ high (97%) Specificity ☞ low (29%) Significantly lower specificity than repeat Pap smear (40%) Not more performable to women c LSIL than repeat cytology More research identify accurate LSIL triage methods such as HPV typing & molecular progression markers (HPV specific viral load, mRNA E6/7, cell cycle proteins, etc.)
 Sensitivity of HC-2 ☞ high (97%) Specificity ☞ low (29%) Significantly lower specificity than repeat Pap smear (40%) Not more performable to women c LSIL than repeat cytology. More research identify accurate LSIL triage methods. such as HPV typing & molecular progression markers. (HPV specific viral load, mRNA E6/7, cell cycle proteins, etc.)")
9
The HPV DNA testing, as a triage tool for colposcopic referral
Management of low grade squamous intraepithelial lesion Immediate referral to colposcopy Repetition of Pap smear in six months Accuracy parameters of cytology & HPV DNA test as triage tools ☞ geographically vary HPV infection and subtypes’ rate may vary between countries These phenomena might influence cost-benefit calculations as the costs of these tools vary quite significantly in countries

10
Colposcopy during pregnancy
During pregnancy, the need for colposcopy Women that conceive after the punch biopsies but prior to the definite treatment of the lesion Those with a lesion detected after an opportunistic smear during usually the first antenatal visits After abnormal cytology → subsequently to be pregnant Conservative management and surveillance even when the index smear indicates high-grade SIL with repeat cytology & colposcopy every 2–3 months

11
Satisfactory colposcopy
Colposcopy during pregnancy Extension of the squamous columnar junction to the ectocervix → Treatment for preinvasive lesions during pregnancy Increased risk of severe intraoperative haemorrhage Possibility of incomplete excision & disease persistence↑ Biopsy Where there is cytologic or colposcopic impression of stromal invasion Conventional knife wedge Bx → Small loop wire excision which contain stroma in order to safely confirm or exclud invasion Satisfactory colposcopy

12
CIN – how to treat Hysterectomy
The majority of women who are diagnosed with CIN ☞ Young & yet to start or complete their family Need for conservative treatment Not compromise therapeutic efficacy Preserve Cx anatomy & future cervical function Hysterectomy Radical procedure rarely used today Limited to older women with coexisting uterine pathology or women who have completed their families

13
CIN – how to treat Cold knife conzation
Prior to hysterectomy, invasive ds needs to be excluded by histological evaluation of the transformation zone Cold knife conzation Conservative Tx aimed at preserving cervical anatomy Rarely used today by out-patient conservative procedures Requires general anaesthesia & hospitalisation Fertility & pregnancy-related morbidity is associated Restricted in selected cases (particularly in older women) Suspicion of microinvasion Severe glandular lesions Residual/recurrent ds after more conservative Tx
 Suspicion of microinvasion. Severe glandular lesions. Residual/recurrent ds after more conservative Tx.")
14
CIN – how to treat Destructive techniques
The more recent conservative methods of Tx Destructive (electrocoagulation, cryotherapy, laser ablation) Excisional (laser conization & electrosurgical excision -LLETZ/ LEEP/NETZ) Destructive techniques Rather easier to perform Destroy the transformation zone epithelium Cone specimen is not provided Marginal status can not be evaluated Precise grade of the treated lesion – not guarantied More intensive or longer f/u
 Excisional (laser conization & electrosurgical excision. -LLETZ/ LEEP/NETZ) Destructive techniques. Rather easier to perform. Destroy the transformation zone epithelium. Cone specimen is not provided. Marginal status can not be evaluated. Precise grade of the treated lesion – not guarantied. More intensive or longer f/u.")
15
CIN – how to treat Excisional techniques
☞ Comprehensive histological evaluation of excised tissue with precise evaluation of excision margins LLETZ : Most popular, by combining all the advantages of the excisional techniques Relatively shorter duration Low cost Good compliance Simplicity Easier learning curve

16
CIN – how to treat In incomplete excision, histologically residual disease ☞ 30–40% More likely to exist when the endocervical margins are involved Clear excisional margins ☞ 3–5% risk of residual ds Extension of the CIN to the endocervical glands & increased age Augment the possibilities of an incomplete Tx Detection, via colposcopy, of HPV satellite lesions outside the transformation zone →→ Independent factor towards treatment failure

17
CIN – how to treat Excisional methods as part of “see and treat” policy ☞ Both evaluation & treatment are performed in the first visit Risk of over-treatment Implemented if unnecessary treatment(+) in less than 10% “Select and treat” policy involves biopsy Prior to treatment which confirms or excludes the presence & the exact grade of the lesion Minimise the over-treatment rates↓ Demand a repeat visit for the appropriate Tx
 in less than 10% Select and treat policy involves biopsy. Prior to treatment which confirms or excludes the presence. & the exact grade of the lesion. Minimise the over-treatment rates↓ Demand a repeat visit for the appropriate Tx.")
18
CIN – how to treat Randomized controlled trial comparing LLETZ
followed or not by cautery of remaining cervical crater Avoiding generalized haemostatic cauterization following LLETZ, particularly around the newly created os, Better follow-up satisfactory colposcopy rates Significantly lower cervical stenosis rates Bleeding ↓↓after loop electrosurgical excision ☞ significantly less bleeding when treatment was performed during the follicular rather than the luteal phase --- J. Nuovo, J. Melnikow, A.R. Willan and B.K. Chan, Treatment outcomes for squamous intraepithelial lesions, Int J Gynaecol Obstet 68 (2000), pp. 25–33.
, pp. 25–33.")
19
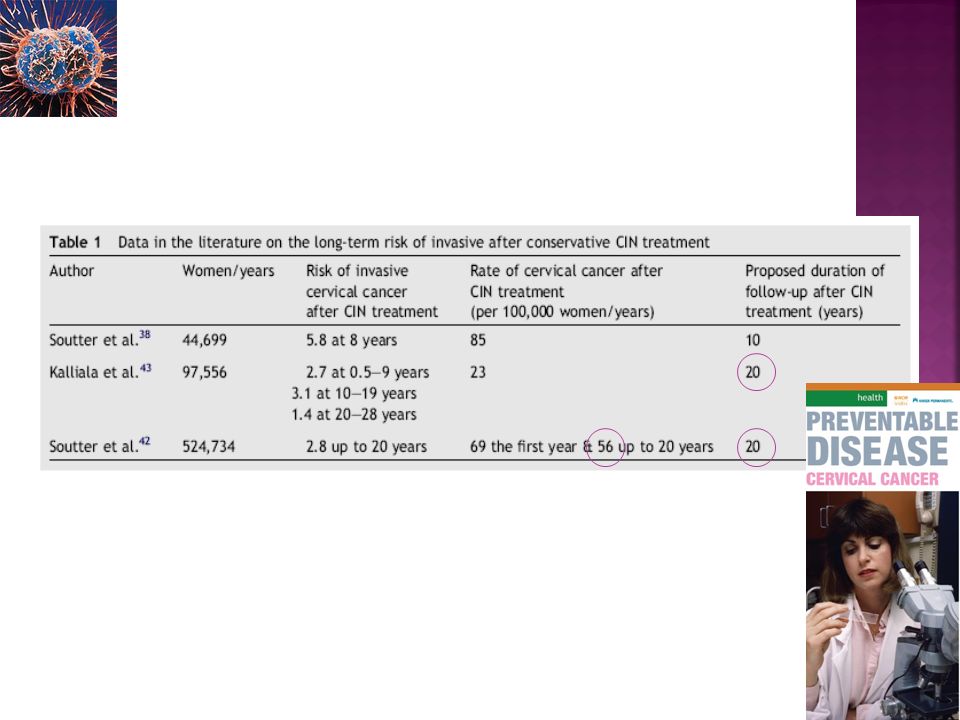
CIN – how to treat Despite the theoretical advantages of excisional techniques, the evidence base clearly suggests that all the conservative methods of treatment present more or less similar efficacy in terms of eradicating intra-epithelial lesions Systematic review on the risk of invasive cervical cancer following conservative therapy 4–5-fold greater risk in this group compared to the general population that remains stable throughout next eight postoperative years

21
Long-term effects on future fertility & pregnancy outcome following conservative treatment for CIN
Recent meta-analysis by Kyrgiou et al.(2006) Cold knife conization risk of preterm delivery low birth weight caesarean section rate LLETZ : risk of preterm delivery, low birth weight & premature rupture of the membranes ↑↑ Laser conization : similar pregnancy-related morbidity Laser ablation : none of the parameters to be affected
 Cold knife conization risk of preterm delivery. low birth weight. caesarean section rate. LLETZ : risk of preterm delivery, low birth weight. & premature rupture of the membranes ↑↑ Laser conization : similar pregnancy-related morbidity. Laser ablation : none of the parameters to be affected.")
22
Figure 3. (A) Cumulative forest plot presenting the risk for obstetric outcomes
& different methods of treatment. (T): favours treatment, (C): favours control. Black: statistically significant. Grey: trends (but failed to reach level of signifi- cance). White: non-significant. (B) Relative risks and 95% confidence intervals For each outcome and method used.
: favours treatment, (C): favours control. Black: statistically significant. Grey: trends (but failed to reach level of signifi- cance). White: non-significant. (B) Relative risks and 95% confidence intervals. For each outcome and method used.")
23
Long-term effects on future fertility & pregnancy outcome following conservative treatment for CIN
The limited data on fertility outcome presented in this review did not reveal any adverse effects Prospectively designed studies dealing with long-term effects on fertility do not exist & would be very difficult to undertake All the original studies were retrospective c all the limitations that this implies and the data on confounding factors that predispose to prematurity might have been incomprehensive

24
Long-term effects on future fertility & pregnancy outcome following conservative treatment for CIN
Future prospectively designed research might give more insight onto whether possible different patterns of cervical behaviour during subsequent pregnancy Related to the proportion of either the cervical volume or the endocervical canal excised Meta-analysis supports observation management of low grade lesions, who have an extremely low risk of progression For young nulliparous women ☞ Reintroduction of laser ablation in selected cases

25
Follow up after treatment
Both cytology & colposcopy are used in different schemes, combinations, intervals and duration In the majority of cases the residual lesion → picked-up during the first few years following Tx, by performing cytology CIN I ☞ follow-up protocol is cytology at 6, 12 and 24 months if every examination is negative then return to national screening programme HgSIL ☞ more intensively monitored with cytology at 6 and 12 months afterwards If cytology turns positive, colposcopy necessity

26
Follow up after treatment
Involved or uncertain margins following excisional treatment ☞ Combination of cytology and colposcopy Reported of higher sensitivity than cytology alone Specificity is reduced, but to a less extend than performing colposcopy in all cases (clear and involved margins) An immediate second excision in case of involved endocervix margins(+) in cases of women older than 50 years of age or in cases of glandular intraepithelial neoplasia In case of an ablative treatment → a longer and closer follow-up surveillance is essential involving probably colposcopy
 An immediate second excision in case of involved endocervix. margins(+) in cases of women older than 50 years of age or. in cases of glandular intraepithelial neoplasia. In case of an ablative treatment. → a longer and closer follow-up surveillance is essential. involving probably colposcopy.")
27
Follow up after treatment
An increased risk for invasive cervical disease lasting nearly 20 years following CIN treatment Reported that HPV DNA test is more sensitive, compared to colposcopy or cytology in detecting CIN treatment failures Both HPV DNA test & cytology aiming to minimize possibility of false negative findings Estimation of HPV viral load → Relation to the higher or lower possibility of Tx failure

28
Follow up after treatment
Application and combination of cytology, colposcopy & more recently developed follow-up markers incorporated within the existing guidelines & alter the follow-up algorithms

29
Colposcopy should not be used as a screening method for the detection of CIN
HPV DNA test (HC-2) has a role in the triage of women c ASCUS, but not in those cases presenting c low grade abnormalities in the index smear Excisional conservative methods of treatment of CIN present long term obstetric morbidity Follow up policy could introduce HPV DNA test for the earlier recognition of treatment failures
 has a role in the triage of women c ASCUS, but not in those cases presenting c low grade abnormalities in the index smear. Excisional conservative methods of treatment of CIN present long term obstetric morbidity. Follow up policy could introduce HPV DNA test for the earlier recognition of treatment failures.")
Similar presentations