Download presentation
Presentation is loading. Please wait.

1
The Gold Standard: Autologous Fascial Pubo-Vaginal Sling
Jerry G. Blaivas Clinical Professor of Urology Joan & Sanford Weil Medcial School Cornell University Adjunct Professor of Urology SUNY Downstate Medical School

2
Cartoon of taking fascia

4
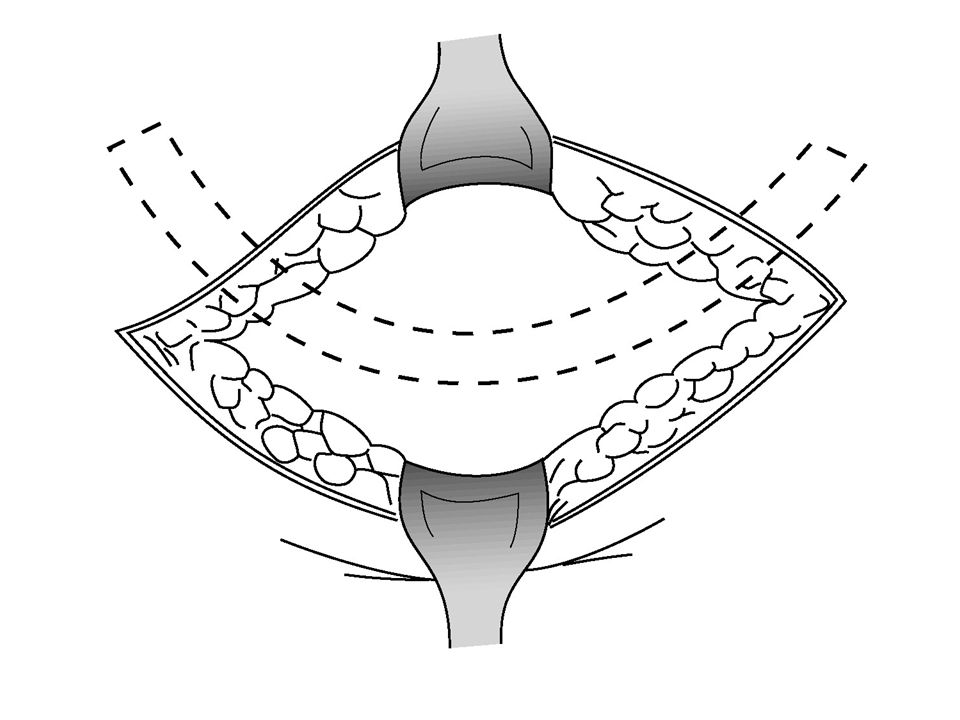
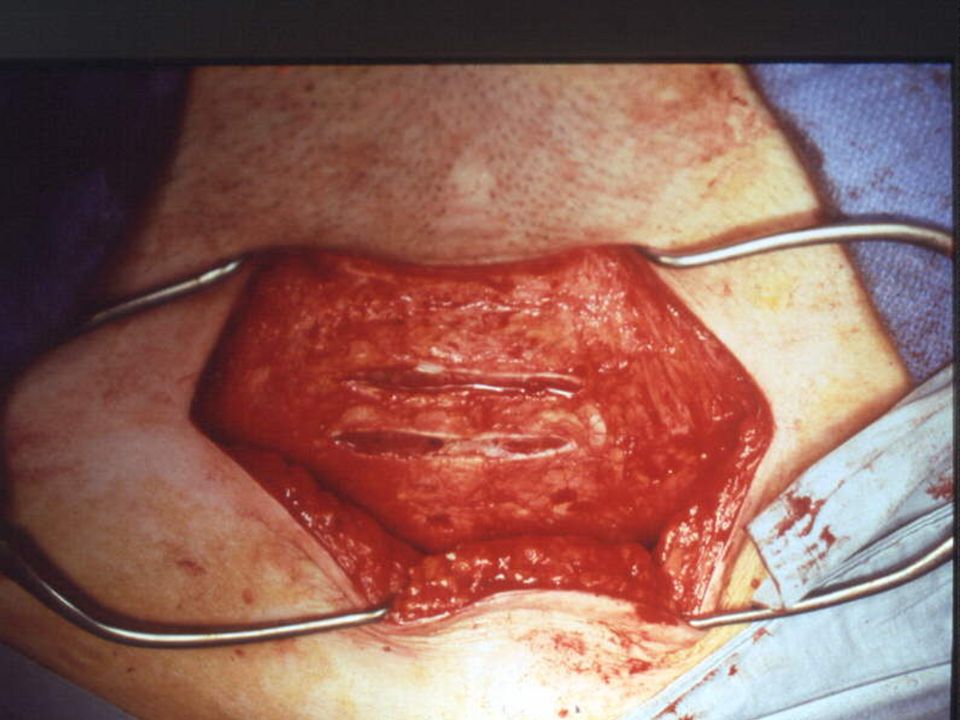
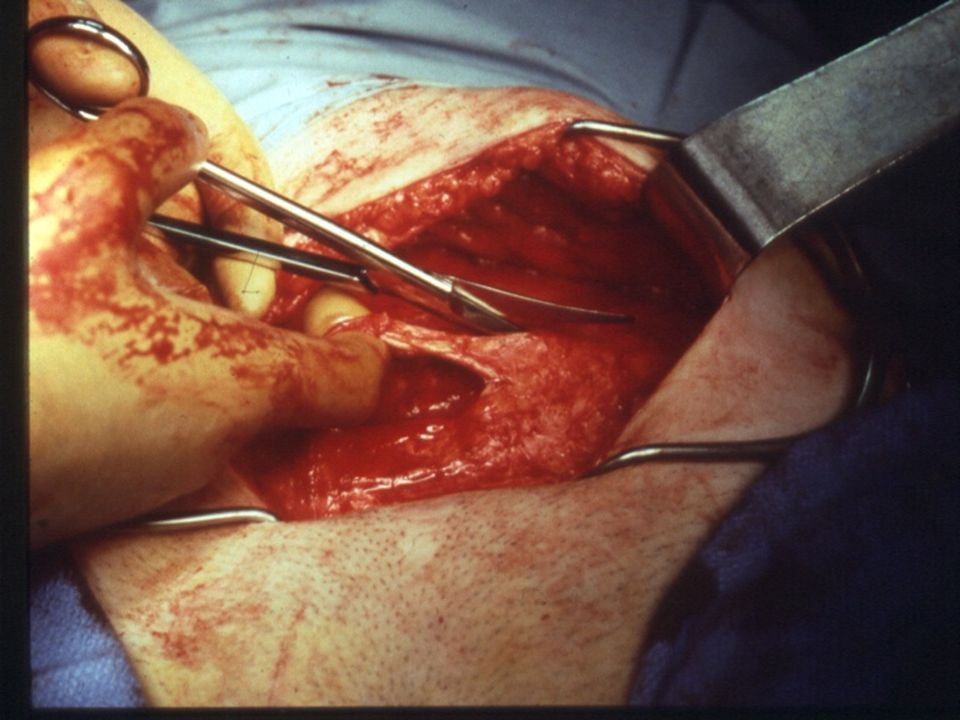
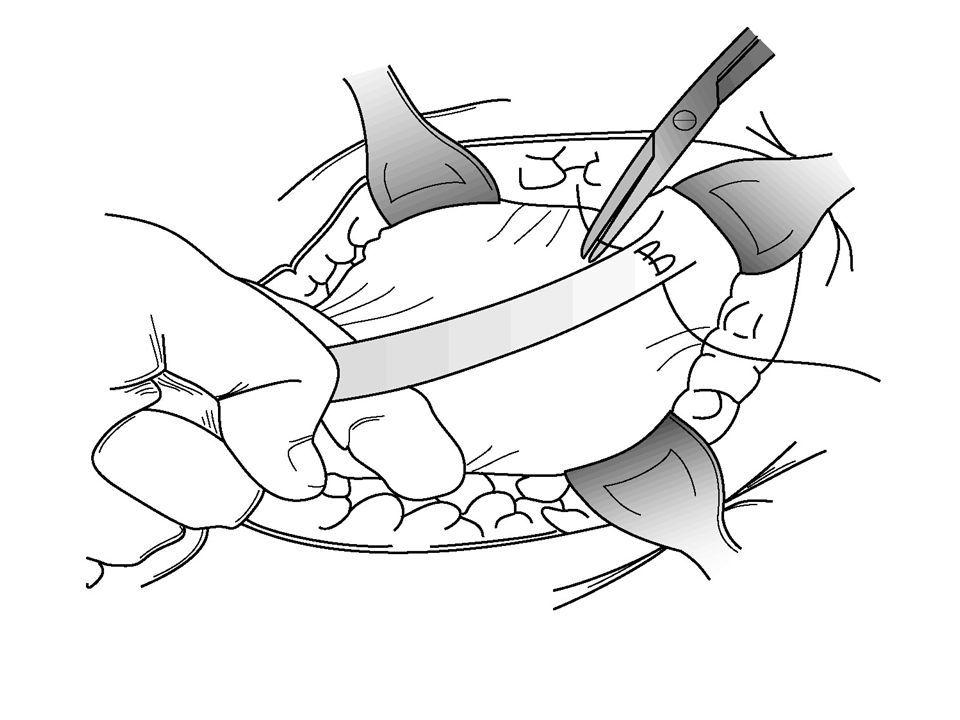
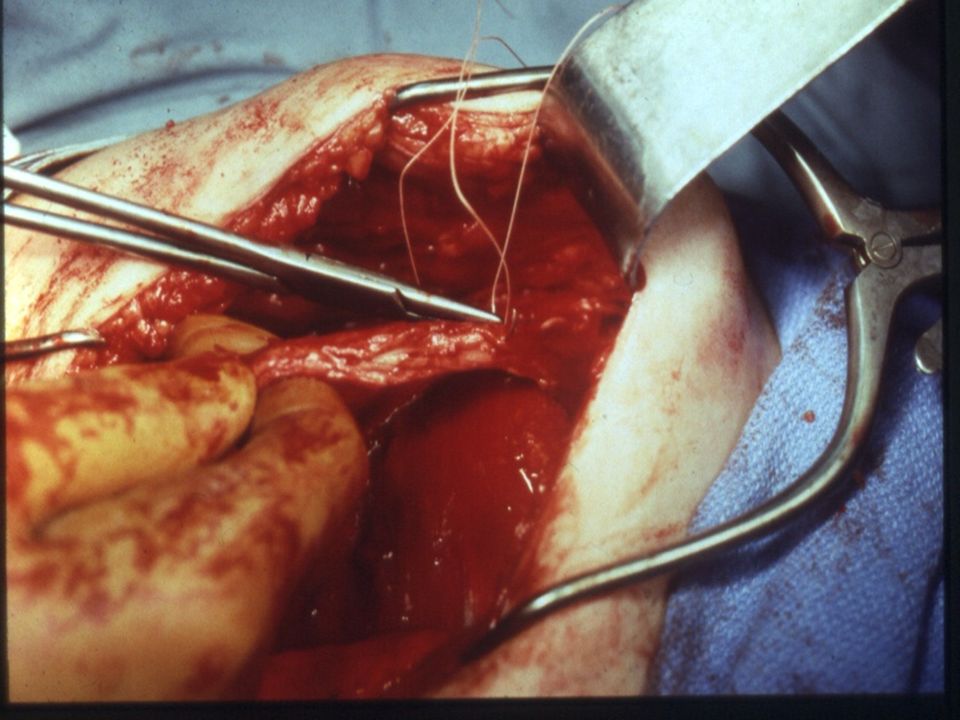
Surgical Technique Horizontal suprapubic incision (4 cm)
Excise rectus fascial strip (6 – 8 cm) Temporarily leave fascia open Horizontal incision over vesical neck
 Temporarily leave fascia open. Horizontal incision over vesical neck.")
5
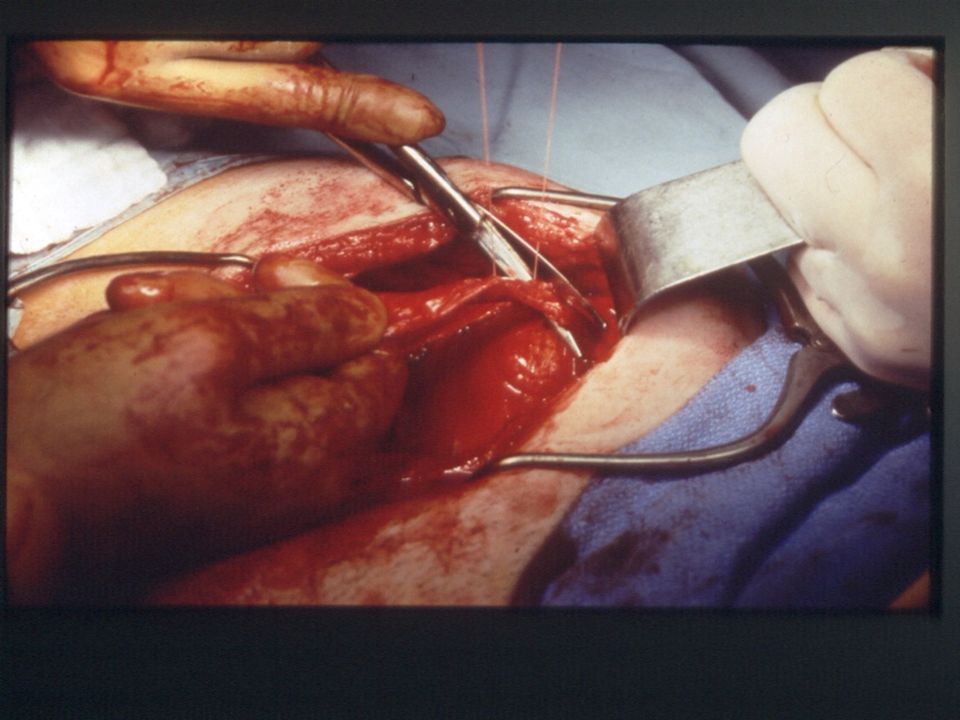
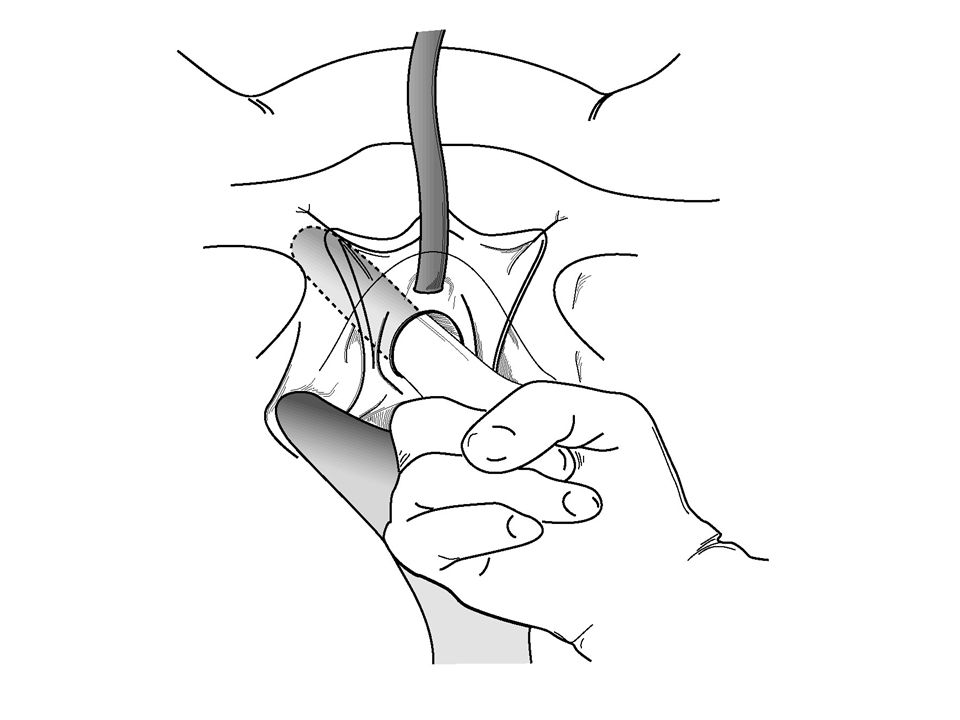
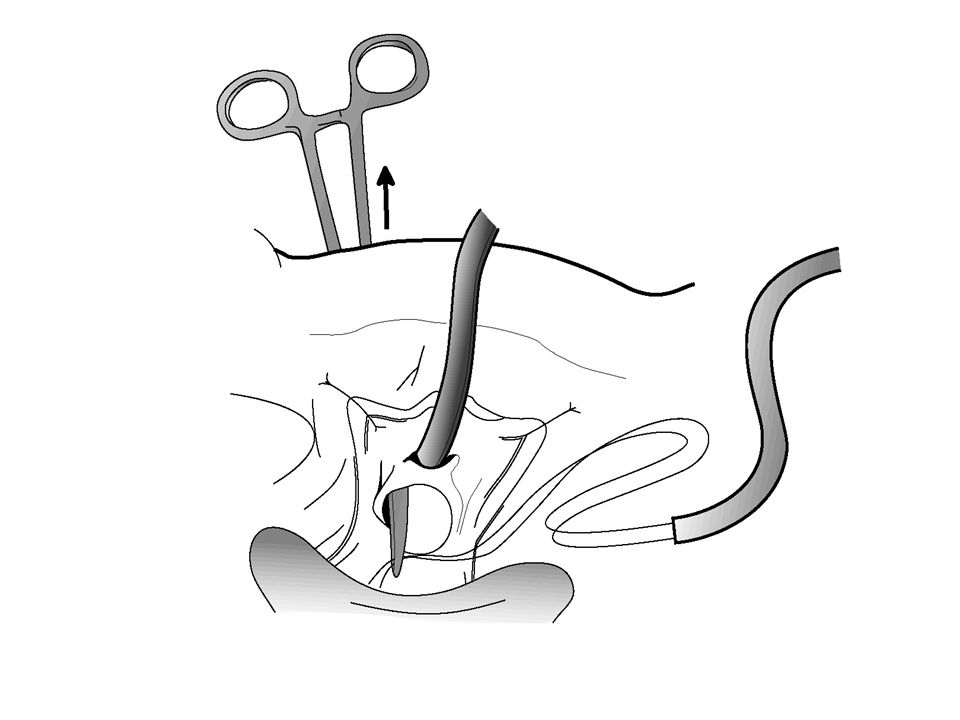
Surgical Technique Mobilize vesical neck from below
Perforate endopelvic fascia Create tunnel & pass sling around vesical neck Cystoscopy

6
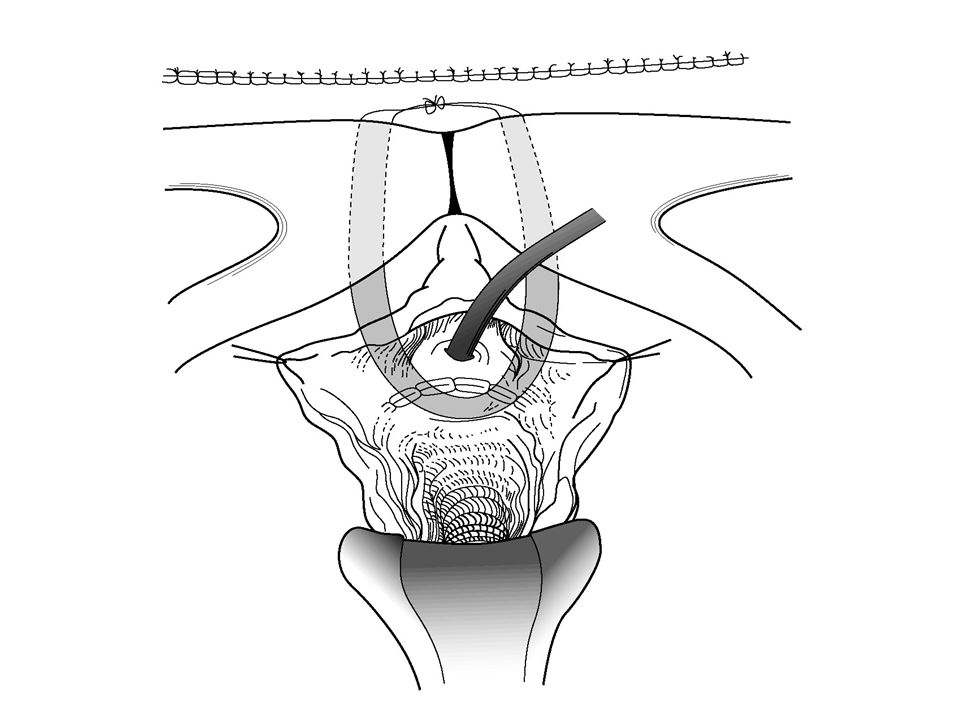
Surgical Technique Close vaginal wound Bring sutures through fascia
Close rectus fascia Suture ends of sling together in midline without tension Close abdominal wound

7
Cartoon of skin incision

8
Picture of Cartoon of skin incision

18
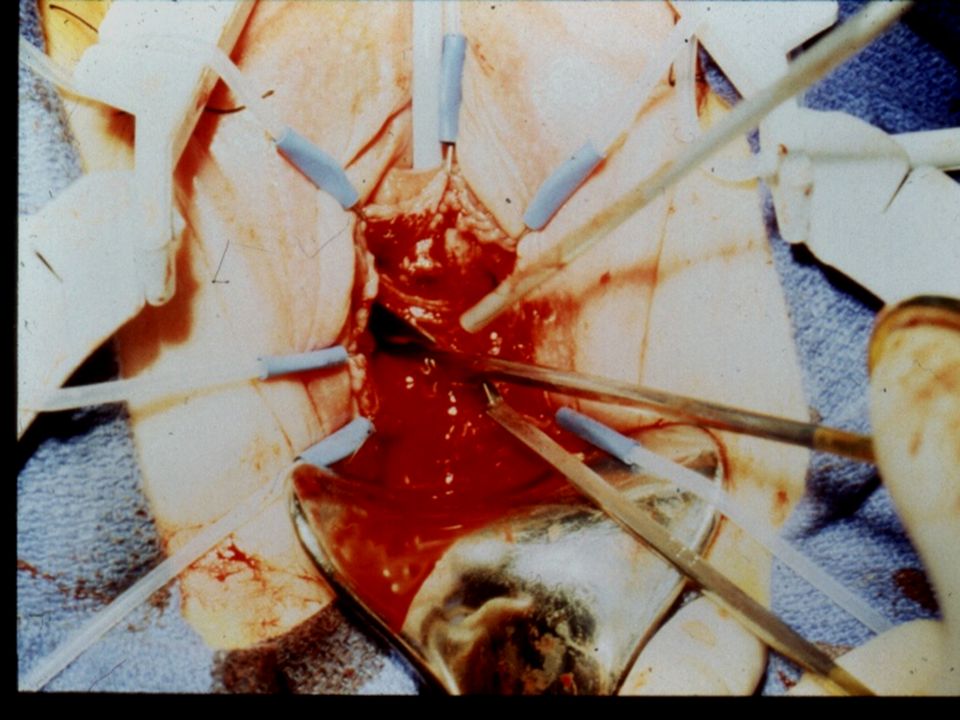
Balloon Incision

19
Allis clamps

20
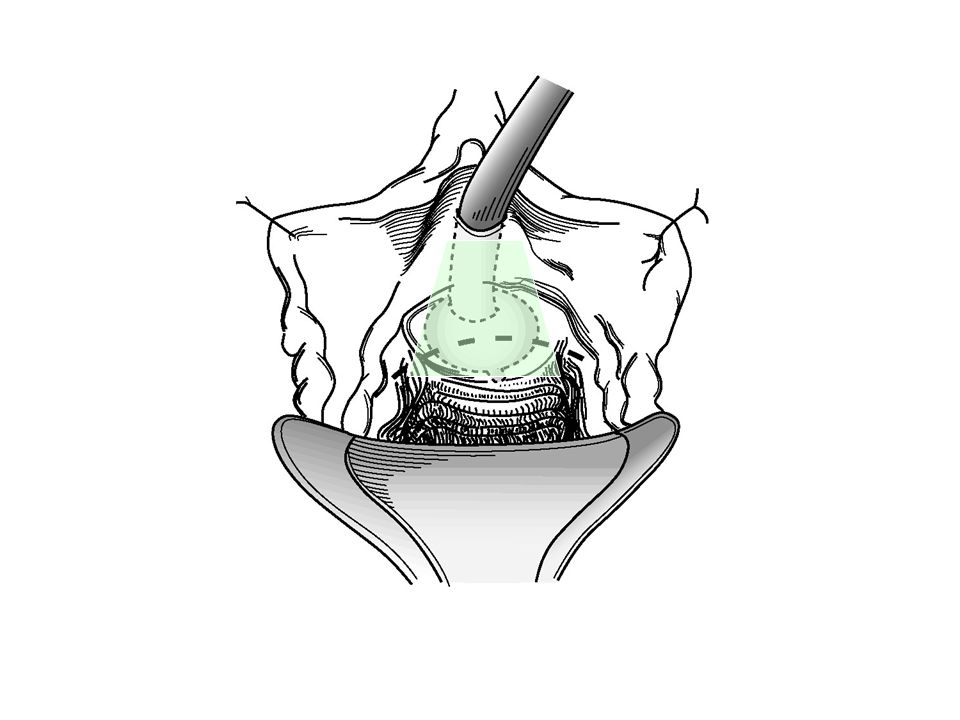
Push up with index finger on vaginal wall
Traction of clamp

21
Left index finger pushing up on vaginal wall
Shiny white surface superficial to pubo-cervical fascia

22
Right wrist flexed downward

23
Incorrect (deep) plane
Correct (superficial) plane
 plane.")
24
Correct plane Incorrect plane Vaginal wall Pubo-cervical fascia

25
Correct (superficial) plane
Pubo-cervical fascia Incorrect (deep) plane
 plane.")
31
Index finger between clamp & urethra & bladder at all times

34
Separate Fascial incision
Inferior edge of rectus Separate Fascial incision Separate stab wound for sling

35
Ends of sling thru fascia
Sutures through separate stab wounds in rectus fascia Ends of sling thru fascia

36
How much tension? None (create a backboard)
(Almost) can’t make it too loose Make sure Q-tip is not negative (elevation of vesical neck)
 can’t make it too loose. Make sure Q-tip is not negative (elevation of vesical neck)")
37
Take slack out of sling Push down on cystoscope parallel to the floor

38
Tie loosely with no tension

41
URINARY INCONTINENCE OUTCOME SCORE
Groutz & Blaivas, Neurourol & Urodyn 19:127,

42
Urinary Incontinence Outcome Score

43
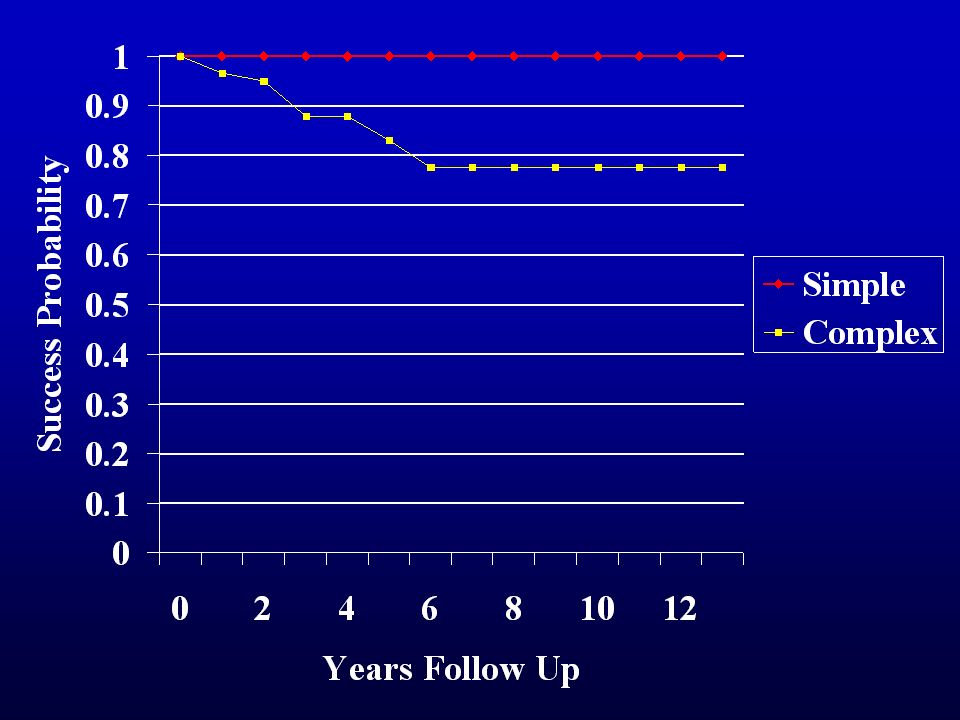
PVS for Simple & Complex SUI OUTCOME SCORE
93% 7%

44
PVS for Simple SUI OUTCOME SCORE
100% 0%

45
Mixed Incontinence Cure/Improved Rates (UIOS <= 4) :
SUI: 97% (n= 44) MUI: 93% (n= 47) non-significant difference (p: 0.33), with study powered a priori to detect > 20% difference in outcome score Chou et al, J Urol, 2003
 MUI: 93% (n= 47) non-significant difference (p: 0.33), with study powered a priori to detect > 20% difference in outcome score. Chou et al, J Urol,")
48
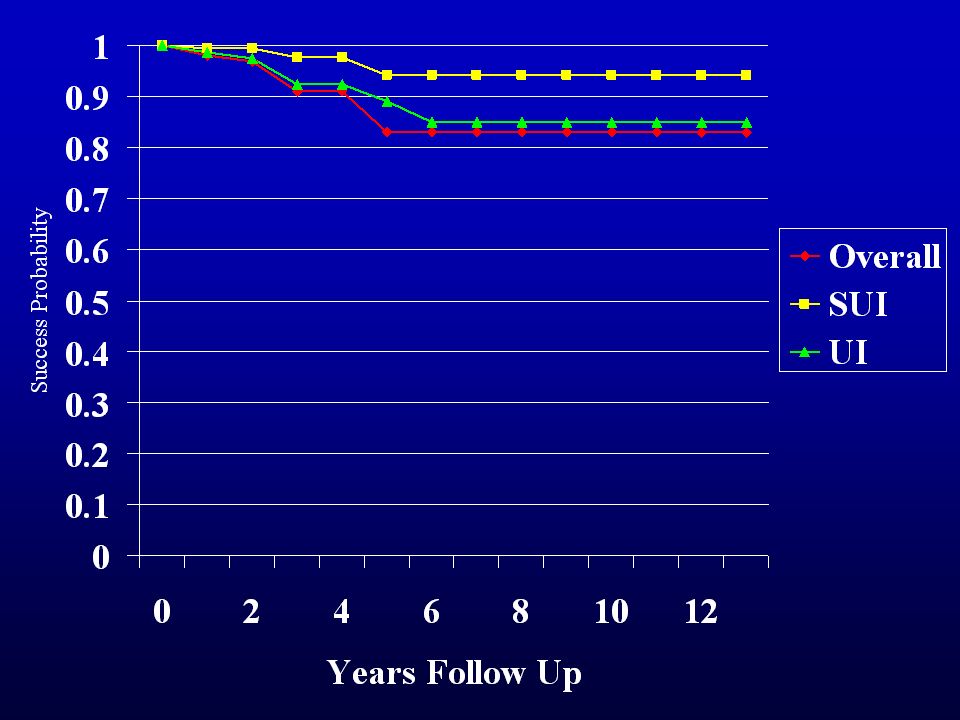
Autologous Sling Outcomes
Cure/Improve rate - 82% at 4 years Urinary Retention requiring intervention - 8% De Novo OAB - 9% (Dmochowski, et al. AUA Guidelines on the Surgical Management of Female Stress Urinary Incontinence, 2010)
")
49
Conclusions Pubovaginal sling effective for: Urethral hypermobility
Intrinsic sphincter deficiency Mixed incontinence Long lasting results Minimal morbidity

50
Conclusions Recurrent stress incontinence is rare
Major risk factor for recurrent SUI is “pipe stem” urethra Urge incontinence is the most common cause of failure Major risk factor for UI is: increasing # of preop urge episodes increasing # of preop UI episodes

51
Conclusions Permanent urinary retention is rare
Risk factors for permanent urinary retention are : preop areflexic neurogenic bladder grade 3 or 4 cytocele excessive sling tension > urethral obstruction

Similar presentations