Download presentation
Presentation is loading. Please wait.

1
Management of Sling Failures: Recurrent Stress Incontinence, Urethral Obstruction and Overactive Bladder Howard B Goldman MD Center for Female Pelvic Medicine and Reconstructive Surgery Glickman Urologic and Kidney Institute The Cleveland Clinic Lerner College of Medicine Case Western Reserve University

2
Sling Outcomes Depending on study 5-15% of patients who have had a midurethral sythetic sling procedure are considered “failures” Rechberger et al, EU, 2009 Richter et al, NEJM, 2010

3
Sling Outcomes Richter et al, NEJM, 2010

4
Failure Greater than 90% of patients generally happy with outcome – “success” – Exact numbers depend on definition What to do with the 5-10% that still leak? Rule out persistent OAB – treat SUI???

5
Persistent Bothersome SUI Observation – Does not get better with time Bulking Agent – Works temporarily but usually recurs “Tighten” sling – Some positive data Repeat sling – Retropubic approach better outcomes than obturator

6
Bulking Agents Outcomes similar to first-line bulking – Works in some patients – Typically not long-lasting – Requires repeat injections Sometimes used as temporizing measure

7
Sling Tightening Based on idea that sling was placed too loosely for this particular patient Sling dissected out Folded and permanent suture placed in to “shorten” length of sling under urethra

8
De Landsheere, et al, IUGJ, 2010

9
Redo Sling Timing? What type of sling? What approach? What about original sling?

10
What type of sling? Midurethral synthetic sling in most cases Fascial sling – If “fixed” perhaps needed fascial sling from the get go My sense is more are comfortable with MUS

11
What approach? Retropubic Transobturator Mini-sling

12
Severity of SUI 208 patients without ISD randomized according to SUI grade – I – loss of urine during significant strain II – loss of urine during minor strain (worse) OutcomesSUI ISUI II retropubic100%100 transobturator10066% Araco, et al, Int Urogyn J, 2008
 OutcomesSUI ISUI II retropubic100%100 transobturator10066% Araco, et al, Int Urogyn J, 2008")
13
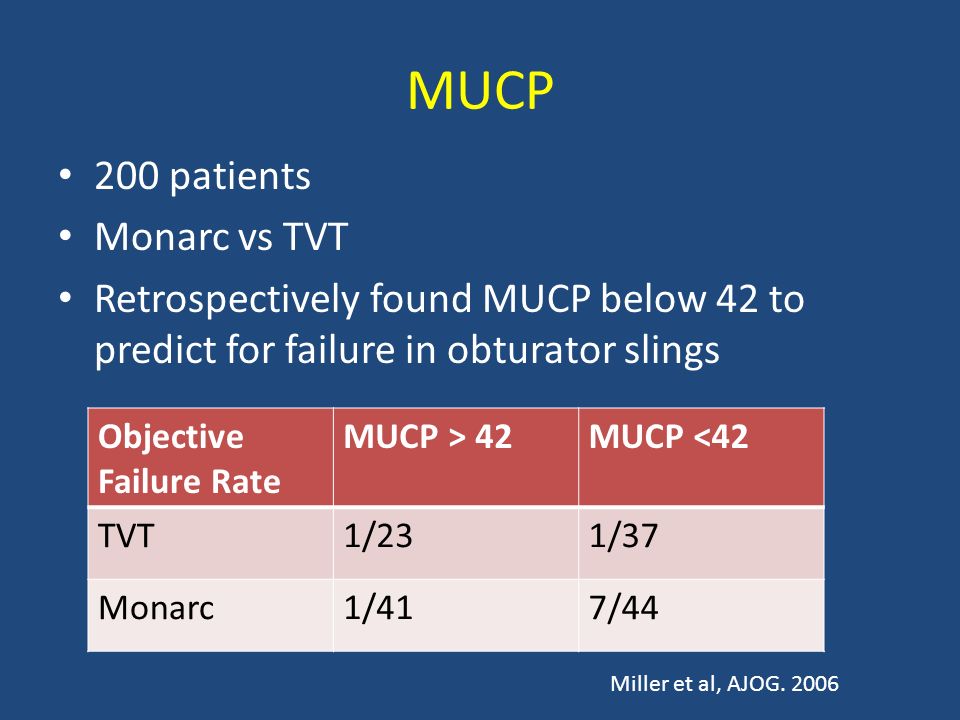
MUCP 200 patients Monarc vs TVT Retrospectively found MUCP below 42 to predict for failure in obturator slings Objective Failure Rate MUCP > 42MUCP <42 TVT1/231/37 Monarc1/417/44 Miller et al, AJOG. 2006
14
ISD Fong, et al, BJUI, 2010

15
Prior Sling Failures 29 patients with prior failed MUS CureFailure Retropubic121 Transobturator106 Lee, et al, J Urol, 2007

16
Prior Sling Failures 77 with prior failed MUS Second procedure NMean VLPPSubjective cure retropubic485771% transobturator298448% Stav et al, J Urol, 2010

17
Risk of Repeat Sling Failure 3 yr fu – prospective randomized trial – 6 mo data previously published – Ob Gyn 2008 TVT vs Monarc n=164 Included those with ISD Mean 37 months – 1.2% TVT required another sling – 18.3% Monarc required another sling Schierlitz, et al, ICS, 2010

18
What about original sling? Don’t look for it – leave alone – Assuming no obstructive or de novo OAB sxs If see it (assuming new one is RP) – Original RP – continue next to it – Original TO – may need to cut and strip some off in either direction Work under it If trochar hits it – move tip slightly
 – Original RP – continue next to it – Original TO – may need to cut and strip some off in either direction Work under it If trochar hits it – move tip slightly.")
19
Iatrogenic Obstruction

20
Symptoms of Iatrogenic Obstruction Retention Incomplete emptying Diminished force of stream Bending forward to void Recurrent UTI “de novo” OAB – may be result of obstruction

21
“de-novo” OAB Make sure was not pre-existing and simply did not improve If “de-novo” evaluate for: – Infection – Iatrogenic urethral obstruction – Sling in bladder/urethra

22
Incidence of Iatrogenic Obstruction True incidence after SUI surgery difficult to pin down – Literature estimates 2.5 - 24% – Contemporary mid urethral sling series 0-5% De Novo Urgency 6 – 25% following TVT 0 – 16% following TOT

23
Basic Evaluation History – TEMPORAL RELATIONSHIP - most important – Symptoms Retention (obvious) Diminished force of stream Positional change to void Irritative symptoms (urgency, UUI, frequency) Recurrent UTI (perhaps due to high PVR) Vague: painful void, pelvic pain, dysuria Physical exam – Hyper-suspension or over correction? – Hypermobility, prolapse PVR UA Goldman, Urologic Clinics N Am, 38, 31-37, 2011

24
Tests and Secondary Evaluations Endoscopy – Eroded sutures – Eroded sling – Urethral kink or displacement Urodynamics (not crucial) – Multi-channel pressure flow with EMG – Video-urodynamics
 – Multi-channel pressure flow with EMG – Video-urodynamics")
25
History Chief Complaint: recurrent UTIs History: 70yo ♀ with recurrent UTIs for last 6 yrs – 4 in past 12 months – Febrile UTIs – Multiple hospital admissions, intravenous abxs Surgical history: – 7 years ago: Uterosacral vault suspension Anterior, posterior repair Retropubic midurethral synthetic sling

26
Urinary Symptoms Urinary Symptoms: – Storage: No incontinence – Voiding: Straining Positional voiding – Postmicturition: Incomplete emptying

27
Physical Exam Abdomen: – Soft, no masses Pelvic Exam: – Urethral mobility 0 - 40º – Tenderness at vaginal apex – No prolapse – PVR 65 cc

28
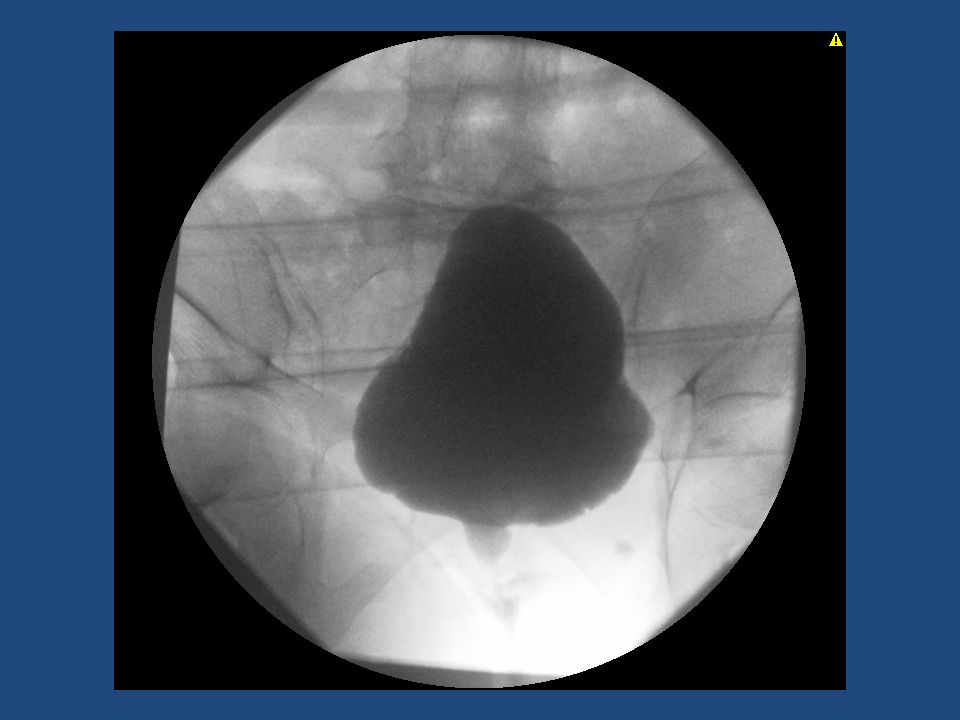
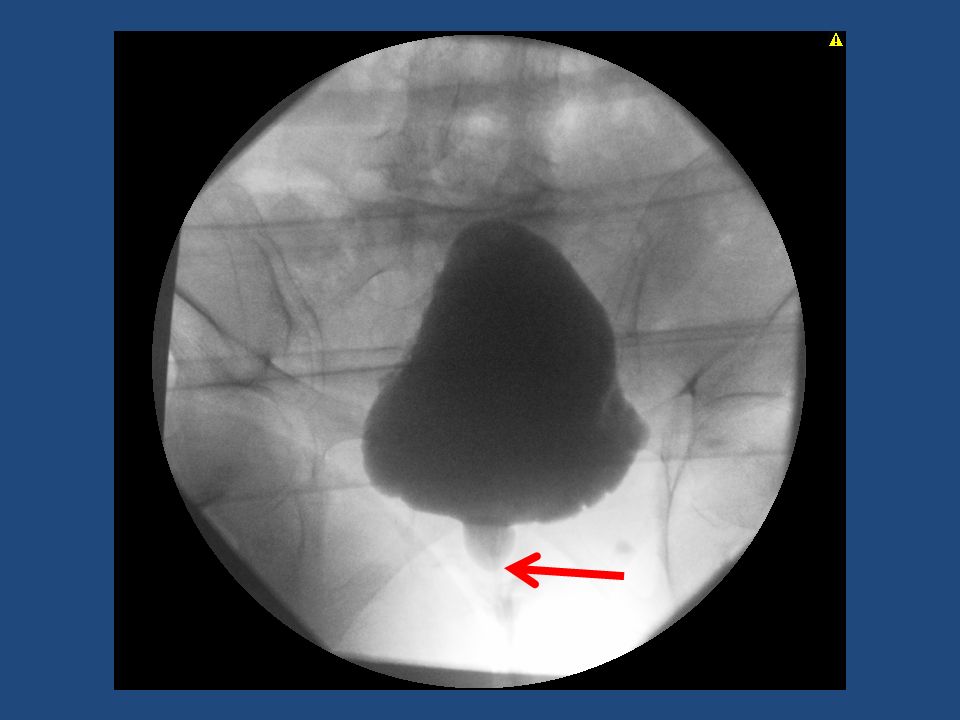
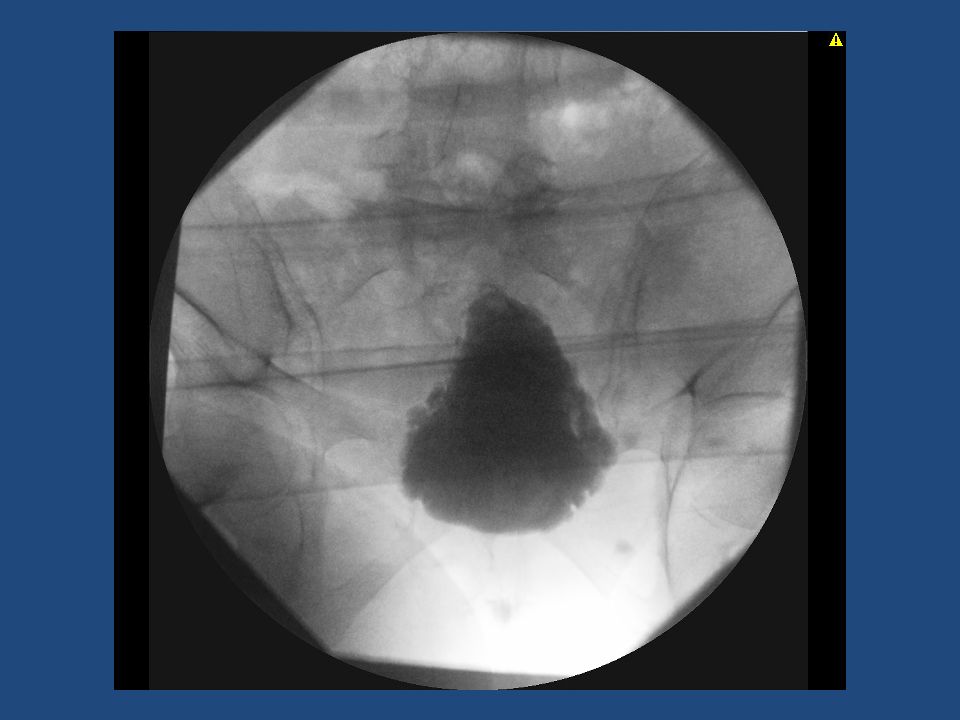
CystoscopyCystoscopy

29
High pressure Low flow

34
Urodynamics Not always helpful in making diagnosis of obstruction after incontinence surgery – Webster & Kreder, 1990 “Urodynamics may fail to diagnose obstruction” – Foster & McGuire, 1993 Urodynamics did not predict outcome – Nitti & Raz, 1994 P det and Q max were not predictive of outcome independently or together. All “acontractile” patients successful

35
Intervention Only absolute selection criteria for urethrolysis should be a temporal relationship between surgery and onset of voiding symptoms Failure to generate a detrusor contraction during urodynamics should not exclude a patient from definitive treatment, e.g. urethrolysis

36
Treatment of Obstruction Time – With fascial slings may take weeks to void normally – With MUS should be voiding normally in hours-days Loosening – Can “loosen” MUS during first few days Full urethrolysis Sling Incision

37
Inverted U or midline incision Isolation of sling in the midline Incision of the sling

38
Sling incision

39
Sling Incision Freeing of the sling from the underlying urethra – May require sharp or blunt dissection No perforation of the endopelvic fascia No freeing of the urethra from the pubic bone Closure of the vaginal wall

40
Obstruction From MUS In cases of early intervention (up to 7-10 days) may be able to loosen by pulling down After 10-14 days need to incise as MUS is ingrown with native tissue Critical to identify and cut or loosen sling If MUS not identified treatment WILL FAIL Chronically can become a tight band
 may be able to loosen by pulling down After days need to incise as MUS is ingrown with native tissue Critical to identify and cut or loosen sling If MUS not identified treatment WILL FAIL Chronically can become a tight band")
42
Sling incision (various slings) NType of IncisionSuccessRecurrent SUI Kusada5Midline100%0% Nitti19Midline84%17% Amundsen32Various94% (for retention) 67% (for UUI) 9% Goldman14Midline93%21% Kusada, Urology, 57, 358-59, 2001 Nitti VW, et al. Urology 2002;59:47–52. Amundsen CL, et al. J Urol 2000;164:434–7. Goldman HB. 2003;62:714–8

43
Infection

44
Infections Sling related soft tissue infections with large pore polypropylene meshes are extremely uncommon Urinary tract infections can occur within the first month or later after sling surgery

45
Current Guidelines AUA recommends a single preop dose of intravenous cephalosporin…..and ≤ 24 hours of postoperative antibiotics Per SCIP a single oral dose of an abx is acceptable Few studies address perioperative antibiotics and incontinence procedures

46
11.7 % 27.5% 3.6% 54.5% 2.8% Swartz and Goldman, Urology, 2010

47
Sling Study - Antibiotics One dose versus multiple doses Group 1 – one perioperative dose of antibiotics Group 2 – one perioperative dose of antibiotics + a few days of oral antibiotics post operatively Swartz and Goldman, Urology, 2010

48
Infection and Adverse Events Related to Antibiotic Use After Sling Surgery OutcomesPeri(n=116) Peri and post (n=104) p value Postoperative UTI 11 (9.5%) 10 (9.6%) NS Postoperative vaginal yeast infection 1 (0.9%) 6 (5.8%) NS Antibiotic Adverse Event 1 (0.9) 8 (7.7%) 0.03 Swartz and Goldman, Urology, 2010
 Peri and post (n=104) p value Postoperative UTI 11 (9.5%) 10 (9.6%) NS Postoperative vaginal yeast infection 1 (0.9%) 6 (5.8%) NS Antibiotic Adverse Event 1 (0.9) 8 (7.7%) 0.03 Swartz and Goldman, Urology, 2010")
49
Sling Failures Continued bothersome SUI – Redo sling Retropubic highest success rate “de-novo” OAB – rule out: – Obstruction – Sling in bladder/urethra Iatrogenic Obstruction – Sling incision For MUS – 20-50% recurrent SUI

Similar presentations

>")


















