Download presentation
Presentation is loading. Please wait.

1
1120 Male Reproductive By Diana Blum RN MSN Metropolitan Community College

4
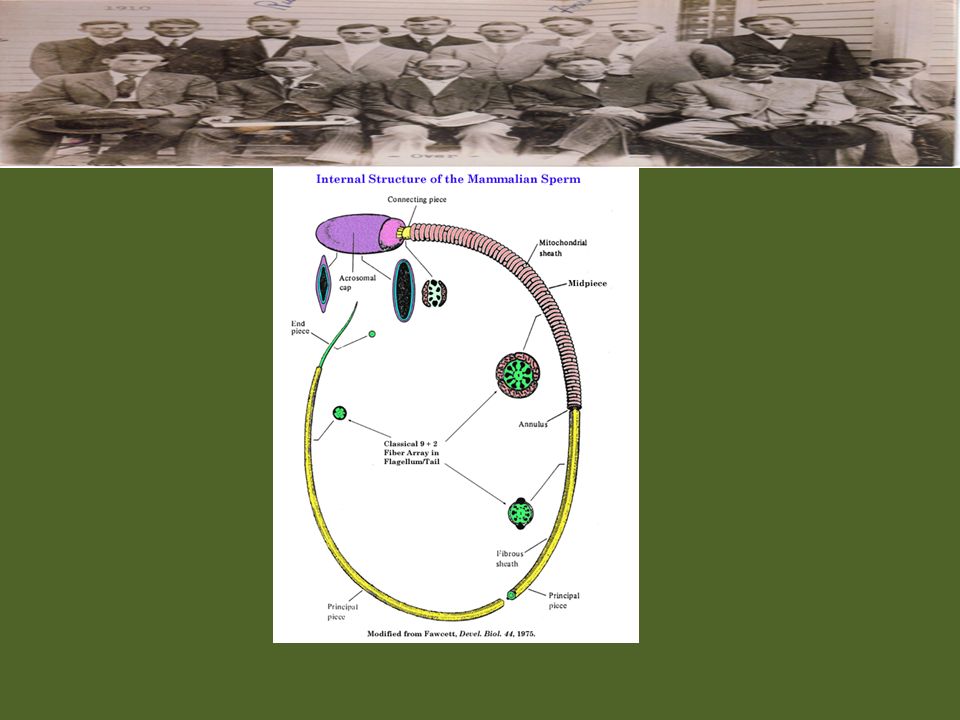
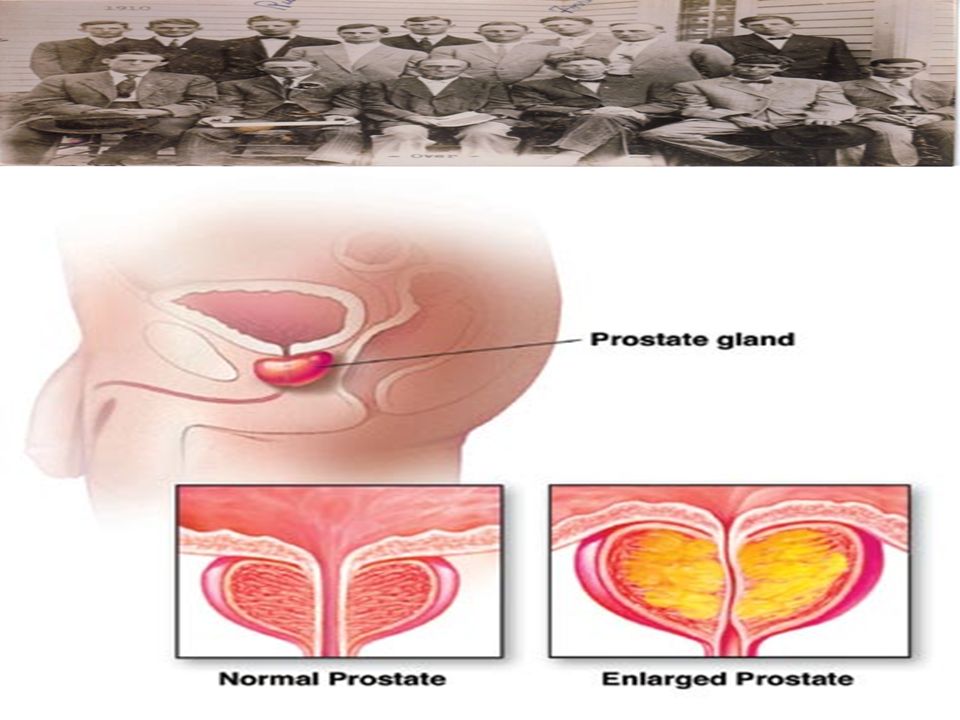
Anatomy Scrotum} thin pendulous sac that holds 2 testes in separate components (protects and insulates) Testes} male reproductive organs. Suspended from spermatic cord. Secretes testosterone. Descend in last 2 mths gestation. Prostate} produces thin milky alkaline liquid that enhances motility and fertility of the sperm. Contracts during ejaculation Cowper’s gland} pea sized..just below prostate, secretes clear mucus into urethra Urethra} empties urine from bladder and provides outlet for ejaculation Epididymis} coiled tubule almost 20 ft long Vas Deferens} tubes of secretory duct that store sperm, contribute semen, and propel fluid during ejaculation Seminal vesicles} hollow twisted tubular secretory glands in posterior bladder. Produce 60% of semen

5
Physiology Cryptorchidism} failure of testes to descend – may result in sterility Emission} result of sympathetic stimulation leaving spinal cord at L1 and L2 Ejaculation} expulsion of semen See page 1128

7
Age Related Changes Testerone continues throughout life but decreases after age 50 Slower to rouse Have longer refractory periods between erections

8
Assessment Look for erectile dysfuntion Assess injuries, diseases, surgeries, meds, allergies Look for knowledge deficit about self exams Assess family Hx Assess diet, exercise, changes in habits, or skin, endocrine problems exam} inspect and palpate

9
Definitions Smegma} white thick odiferous secretion b/w glans and foreskin Hydrocele} mass filled with serous fluid and glows red with light Hematocele} mass filled with serous fluid. Looks like a shadow in light because no light passes through

11
Diagnostics Semen analysis: too high or too low =infertility, look for thyroid, pituitary, adrenal, or testicular dysfunction Tumor markers X-ray See page 1133-1134

12
Disorders Prostatitis: inflamed prostate gland – S/S: swelling, warmth, tenderness, dysuria, frequency, hematuria, foul smelling urine, malaise – Tx: antibiotics, analgesics, sitz bath Epididymitis: inflamed epididymis – Causes: infection, trauma, urine reflux – S/S: scrotal edema, n/v, chills, fever – Tx: bedrest, antibx, analgesics, antiinflamatory, scrotal support Orchiditis: inflamed testes – Causes: trauma, mumps, pneumonia, TB – S/S: fever, tenderness, swelling of testes (can lead to sterility) – Tx: analgesics, antiyretics, bedrest, scrotal support, local heats
 – Tx: analgesics, antiyretics, bedrest, scrotal support, local heats")
13
Disorders BPH} enlargement of prostate – s/s: obstructive, irrative, decreased urine flow, urinary retention, post void dribbling, urgency, incontinence, frequency, dysuria, nocturia, hematuria – Tx: meds (proscar, flomax), TURP – Nsg Dx: fear, impaired urinary elimination, ineffective therapeutic regimen – Interventions: space fluid throughout day, avoid ETOH and antihistamines, bladder scan, foley (p. 1137--1138)
.")
15
Post-Op Vs Monitor blood in urine and clots seen Strict I/O CBI to prevent clots Manually irrigate as ordered Assess pain Care plan page 1139

16
Peyronie’s DX Development of plaque under skin of penis Occurs b/w 45-70 years of age result of an injury that caused inflammation Leads to failure to fill and store TX: topical or oral meds with vitamin E, chochicine, tamoxifen, etc

17
Erectile Dysfunction Failure to initiate- inability to initiate erection – Cause: nerve damage, stress, anxiety, hormone problems – Tx: therapy, hormones, injections, implant Failure to fill- erection develops slowly – Cause: arterial blockage – Tx: therapy, revascularization, implant Failure to store- poorly maintained erection – Cause: stress, aging, injury – Tx: therapy injections, sildenafil (viagra), venous ligation, implant BP meds interfere with erection Viagra: vasodilator and is contraindicated with those on nitrates and hypotension
, venous ligation, implant BP meds interfere with erection Viagra: vasodilator and is contraindicated with those on nitrates and hypotension")
18
Penile implant

19
Priapism Prolonged erection not related to desire Causes: sickle cell crisis, injury, neoplasms, or certain meds (see page 1147) May be painful, may obstruct urine, may cause hydronephrosis
 May be painful, may obstruct urine, may cause hydronephrosis")
20
Phimosis Edema that prevents retraction of the foreskin Causes: poor hygiene, inflammation Tx: antimicrobials, and proper cleansing Uncircumsized med need to retract foreskin for proper cleaning

22
Infertility Caused by: infection, cryptorchidism, variocele, testicular torsion, vasectomy Testicular torsion: when testicle is mobile and spermatic cord twists… requires surgery Variocele: lengthening and enlargement of scrotal portion that drains..caused by valve problems in the spermatic venous system Cryptorchidism: any testis located somewhere other than scrotum – Must be corrected in first 18 months of life to improve infertility – Men with undescended testicles have 10-30 times more incidence of testicular cancer

23
Vasectomy Surgical removal of a portion of the vas deferons Birth control must be used until lab determines that no sperm are present – Analysis will be started after 15 ejaculations post surgery

25
Testicular/Prostate Cancer Testicular – 3 risk factors: cryptorchidism, white race, previous history – Nsg Dx: anxiety, acute pain, impaired urinary retention, risk for injury, constipation, low self esteem, knowledge deficit Prostate – Tx: routine PSA level checks, radiation, hormone therapy, surgery, chemo

Similar presentations






















 Begin producing sperm.>")


