Download presentation
Presentation is loading. Please wait.

1
Pathology of Kidney Dr. Sachin Kale, MD. Associate Professor, Dept of Pathology.

2
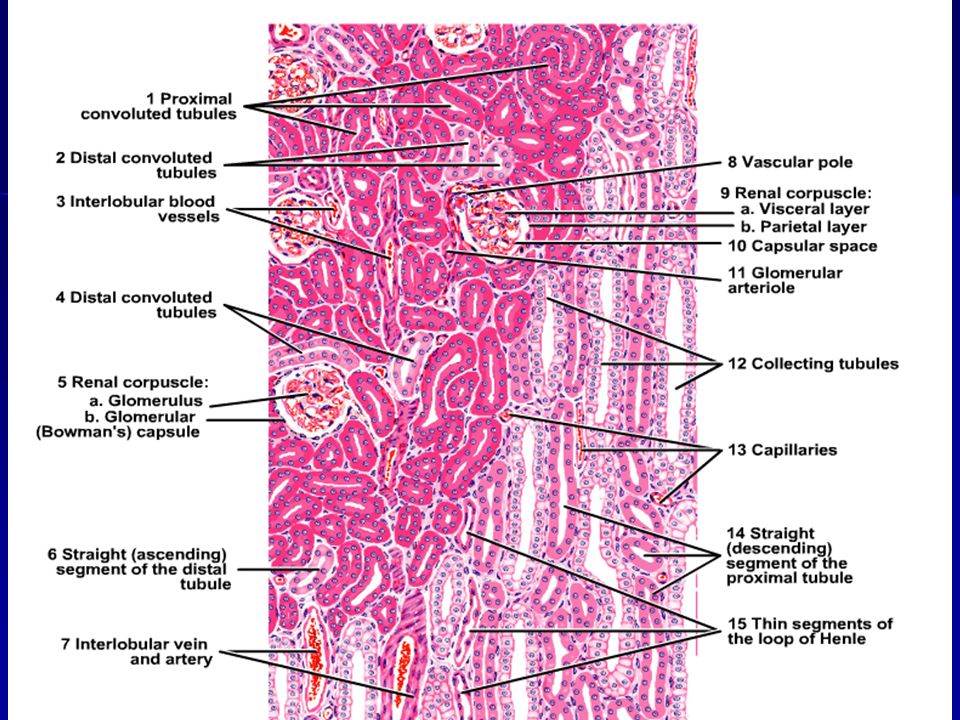
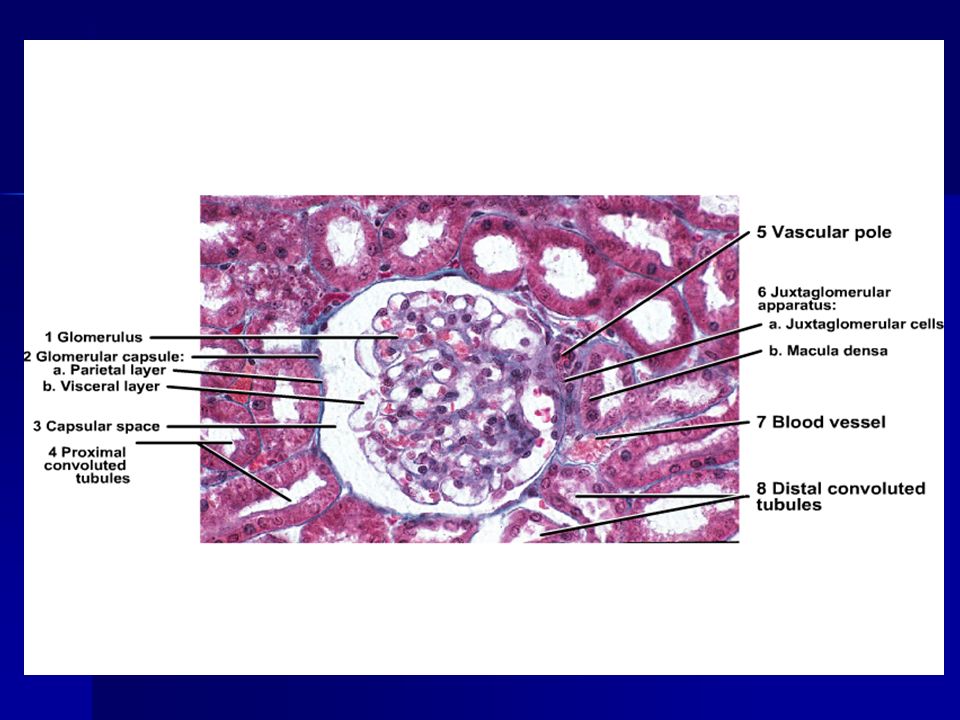
Anatomy of Kidney Note the positions of Glomerulus PCT, DCT, CT Cortex, Medulla, Pelvis.

5
Glomerular diseases: Primary Primary –Acute diffuse post streptococcal –RPGN –Membranous GN –FSGS –MPGN –Lipoid nephrosis or minimal change –IgA nephropathy Secondary Secondary –SLE, Diabetes, Amyloidosis, Goodpasture’s syndrome, PAN, WG, HSP, Hypertension etc.

6
Clinical Syndromes: Ne phritic syndrome. Ne phritic syndrome. –Oliguria, Haematuria, Proteinuria, Oedema, Azotemmia, Hypertension. Nephrotic syndrome. Nephrotic syndrome. –>3.5 gm proteinuria, Hypoalbuminemia hyperlipidemia, Lipiduria RPGN. RPGN. –Nephritis, loss of Kidney function - within weeks Chronic renal failure. Chronic renal failure. –Azotemia/uremia progressing over months and years Asymptomatic Hematuria or proteinuria

7
Fluid and Electrolytes: Dehydration, Edema, Hyperkalemia, Metabolic acidosis Calcium Phosphate and Bone: Hyperphosphatemia, Hypocalcemia, Secondary hyperparathyroidism, Renal osteodystrophy Hematologic: Anemia, Bleeding diathesis Cardiopulmonary: Hypertension, Congestive heart failure, Pulmonary edema, Uremic pericarditis Gastrointestinal: Nausea and vomiting, Bleeding, Esophagitis, gastritis, colitis Neuromuscular: Myopathy, Peripheral neuropathy, Encephalopathy Dermatologic: Sallow (greenish-yellow) color, Pruritus, Dermatitis CHRONIC RENAL FAILURE
 color, Pruritus, Dermatitis CHRONIC RENAL FAILURE")
8
ACUTE TUBULAR NECROSIS Destruction of renal TUBULAR epithelium Loss of renal function 50% of ACUTE renal failure Two types: ISCHEMIC NEPHROTOXIC - AMINOGLYCOSIDES - AMPHOTERICIN B - CONTRAST AGENTS

9
NORMAL

10
ATN

11
ATN PATHOGENESIS BLOOD FLOW DISTURBANCES (ISCHEMIC) TUBULAR INJURY (NEPHROTOXIC)
 TUBULAR INJURY (NEPHROTOXIC)")
12
CLINICAL COURSE INITIATION (36 hours) –Mild OLIGURIA –Mild AZOTEMIA MAINTENANCE –More OLIGURIA –More AZOTEMIA –DIALYSIS NEEDED RECOVERY –HYPOKALEMIA main problem –BUN, CREATININE return to normal
 –Mild OLIGURIA –Mild AZOTEMIA MAINTENANCE –More OLIGURIA –More AZOTEMIA –DIALYSIS NEEDED RECOVERY –HYPOKALEMIA main problem –BUN, CREATININE return to normal")
13
Immune Mechanisms of Glomerular injury: Antibody mediated: Antibody mediated: In-Situ immune complex deposition In-Situ immune complex deposition –Tissue antigens - Goodpasture anti GBM Ag –Planted antigens - infections, toxins, drugs. Circulating immune complex deposition. Circulating immune complex deposition. –Endogenous - DNA as in SLE –Exogenous – infections – HBsAg, Syphilis, Streptococcal, Falciparum, Cell mediated Immune injury Cell mediated Immune injury Activation of alternate complement pathway Activation of alternate complement pathway

14
Immune Glomerulonephritis: 1. Antigen or Antibody - Immune reaction 2. Activation of complements, Neutrophils… 3. destruction of glomerular structure 4. Inflammation, exudation swelling. 5. ↓ blood flow, GFR, - 6. Oliguria, Proteinuria, Hematuria, Hypertension.

15
Neutrophil Activity Proteases – GBM degradation Proteases – GBM degradation Reactive oxygen metabolites – cell damage Reactive oxygen metabolites – cell damage Arachidonic acid metabolites – Reduction in GFR Arachidonic acid metabolites – Reduction in GFR

16
Other Mediators Cytotoxic antibodies Cytotoxic antibodies Macrophages Macrophages Platelets Platelets Resident glomerular cells Resident glomerular cells Fibrin related products Fibrin related products

17
Nephritic Syndromes : Diffuse Proliferative GN Diffuse Proliferative GN –Post Streptococcal. Rapidly Progressive GN (or Crescentic) Rapidly Progressive GN (or Crescentic) –Post Streptococcal, Goodpasture’s, Focal Glomerulonephritis Focal Glomerulonephritis –Primary: Bergers disease (IgA Nephritis) –Secondary IgA nephritis, Henoch Schonlein purpura, SBE, Coeliac Disease etc.
 Rapidly Progressive GN (or Crescentic) –Post Streptococcal, Goodpasture’s, Focal Glomerulonephritis Focal Glomerulonephritis –Primary: Bergers disease (IgA Nephritis) –Secondary IgA nephritis, Henoch Schonlein purpura, SBE, Coeliac Disease etc..")
18
Diffuse Proliferative GN: Post streptococcal* common – Post streptococcal* common – Primary infection - Pharynx, skin, ear etc.. Primary infection - Pharynx, skin, ear etc.. Kidney damage – 1-4 weeks after infection. Kidney damage – 1-4 weeks after infection. Malaise, fever, nausea, edema*, ↑ ASO, ↓ C3 Malaise, fever, nausea, edema*, ↑ ASO, ↓ C3 Resolution in 6-8 weeks. Resolution in 6-8 weeks.

19
Post Streptococcal GN (Prol.GN): 1-4 weeks following streptococcal infection by nephritogenic strains (time for Ab formation) 1-4 weeks following streptococcal infection by nephritogenic strains (time for Ab formation) Immune mediated Immune mediated Granular deposits of IgG,IgM & C3 in GBM, (subepithelial location common) Granular deposits of IgG,IgM & C3 in GBM, (subepithelial location common) Humps in GBM on EM or IF Microscopy Humps in GBM on EM or IF Microscopy
: 1-4 weeks following streptococcal infection by nephritogenic strains (time for Ab formation) 1-4 weeks following streptococcal infection by nephritogenic strains (time for Ab formation) Immune mediated Immune mediated Granular deposits of IgG,IgM & C3 in GBM, (subepithelial location common) Granular deposits of IgG,IgM & C3 in GBM, (subepithelial location common) Humps in GBM on EM or IF Microscopy Humps in GBM on EM or IF Microscopy")
20
Normal Inflammation Proliferation Swelling. Narrow capillary ↓GFR-Renin-BP Post Strepto GN

21
Diffuse Proliferative GN: Enlarged hypercellular glomeruli. Enlarged hypercellular glomeruli. Hyperplasia of epithelium & endothelium. Cell Swelling. Hyperplasia of epithelium & endothelium. Cell Swelling. Inflammatory cells. Inflammatory cells. Collapsed capillaries. Obstruction to blood flow. Collapsed capillaries. Obstruction to blood flow.

22
IF- Diffuse Proliferative GN

23
Pathogenesis of Diffuse PGN: Streptococcal infection – Antibody attack GBM - inflammation & proliferation. Streptococcal infection – Antibody attack GBM - inflammation & proliferation. Glomerular capillary obstruction: Glomerular capillary obstruction: –J.G.A stimulation – Renin – high blood pressure –Reduced filtration – raised blood urea –Fluid retention – Oedema Damage to GBM: Damage to GBM: –Unselective proteinuria (form Pr. casts in tubule) –Haematuria (form RBC casts in tubule)
 –Haematuria (form RBC casts in tubule).")
24
Progression of DPGN: Poststreptococ cal DPGN CGN Cardiac Failure or Uremia; death in acute phase Complete Healing Rapidly Progressive GN

25
RPGN Clinicopathologic syndrome Clinicopathologic syndrome Glomerular damage Glomerular damage Rapid progressive decline in renal function Rapid progressive decline in renal function Histology: accumulation of cells in Bowman’s space in the form of “Crescents” Histology: accumulation of cells in Bowman’s space in the form of “Crescents”

26
RPGN: Classification & Pathogenesis Postinfectious Postinfectious GN associated with systemic diseases GN associated with systemic diseases Idiopathic RPGN Idiopathic RPGN Glomerular injury is immunologically mediated. Glomerular injury is immunologically mediated. Goodpasture’s syndrome – classic anti- GBM nephritis Goodpasture’s syndrome – classic anti- GBM nephritis

27
RPGN classification Post-infectious RPGN Post-infectious RPGN Systemic diseases – Systemic diseases – –SLE, Goodpasture’s, Vasculitis (PAN), Wegener’s granulomatosus, HSP, Essential cryoglobulinemia Idiopathic RPGN Idiopathic RPGN
, Wegener’s granulomatosus, HSP, Essential cryoglobulinemia Idiopathic RPGN Idiopathic RPGN")
28
RPGN cont.. Idiopathic : ½ the cases, Idiopathic : ½ the cases, Linear, Granular or minimal to none immune deposits Linear, Granular or minimal to none immune deposits Gross: Enlarged pale kidneys Large white kidney Gross: Enlarged pale kidneys Large white kidney Petechial hemorrhages in cortex Petechial hemorrhages in cortex M/E: Glomeruli: focal necrosis, endothelial proliferation M/E: Glomeruli: focal necrosis, endothelial proliferation

29
RPGN… Formation of crescents: Formation of crescents: Proliferation of parietal cells, migration of monocytes and macrophages into Bowman’s space Proliferation of parietal cells, migration of monocytes and macrophages into Bowman’s space Crescents obliterate Bowman’s space, compression capillary tuft Crescents obliterate Bowman’s space, compression capillary tuft Crescents undergo sclerosis Crescents undergo sclerosis

30
RPGN: Clinical features Goodpasture’s Syndrome: recurrent hemoptasis & renal manifestations Goodpasture’s Syndrome: recurrent hemoptasis & renal manifestations Hematuria, Red cell casts, Moderate proteinuria, Hematuria, Red cell casts, Moderate proteinuria, Variable HT and edema Variable HT and edema Oliguria Oliguria

32
Which of the following presents with hematuria, proteinuria and hypertension Nephrotic syndrome Nephrotic syndrome Nephritic Syndrome Nephritic Syndrome UTI UTI Renal Tubular Acidosis Renal Tubular Acidosis

33
All of the following are seen in renal failure except Hypercalcemia Hypercalcemia Hyperkalemia Hyperkalemia Bone lesions Bone lesions Metobolic Acidosis Metobolic Acidosis

34
Anemia in renal failure is generally Microcytic hypochromic Microcytic hypochromic Normocytic normochromic Normocytic normochromic Dimorphic Dimorphic megaloblastic megaloblastic

35
Which of the following is not a primary GN Minimal Change disease Minimal Change disease Membranous GN Membranous GN Diabetes mellitus Diabetes mellitus RPGN RPGN

36
Which of the following is not part of nephrotic syndrome Lipiduria Lipiduria Hypertension Hypertension Proteinuria Proteinuria Edema Edema

37
True about Post-strepto GN - Occurs 1 – 4 months after infection Occurs 1 – 4 months after infection Occurs 1 – 4 days after infection Occurs 1 – 4 days after infection Occurs 1 – 4 weeks after infection Occurs 1 – 4 weeks after infection Non of the above Non of the above

38
False about RPGN.. Formation of crescents Formation of crescents Small contracted kidneys Small contracted kidneys Hematuria Hematuria Oliguria Oliguria

39
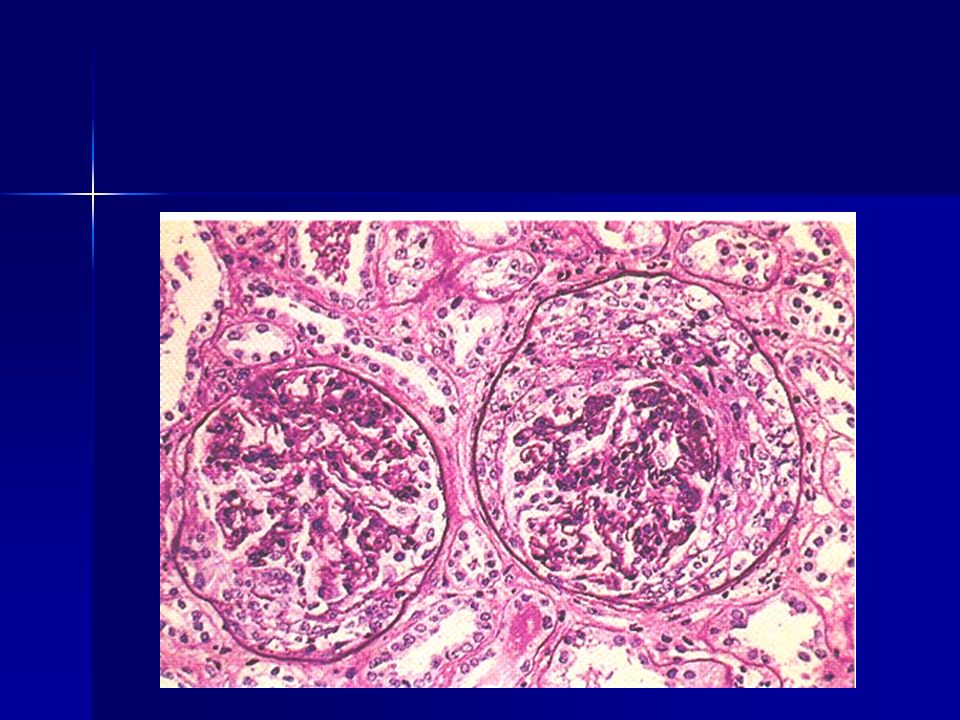
Spot the diagnosis RPGN

40
Spot the diagnosis ATN

41
Spot the diagnosis Post streptoco ccal GN

42
Thought for the day… Ours is a world where people don't know what they want and are willing to go through hell to get it. Ours is a world where people don't know what they want and are willing to go through hell to get it.

43
Thanks… http://sachinkale1.tripod.com http://sachinkale1.tripod.com

Similar presentations













 RENAL DISEASE: OVERVIEW AND ACUTE RENAL FAILURE Pathophysiology of Disease: Chapter 16 (388-394) Jack.>")




 is the sudden onset of: – Haematuria (macroscopic/microscopic)>")
SC>")