Download presentation
Presentation is loading. Please wait.

1
Drugs used in Parkinson disease

2
Epidemiology Average age of onset 62.5 Men and women affected equally Genetic Link African-Americans and Asians less likely than Caucasians to develop Parkinson ’ s Caffeine and smoking shows some protective effects

3
Pathogenesis Four Theories Oxidative damage Impaired protection Environmental toxins MPTP-Methyl-phenyl tetrahydropyridine Genetic predisposition Mutations in the gene for the protein alpha-synuclein located on chromosome 4 Accelerated aging

4
Pathophysiology Imbalance of dopamine and acetylcholine Loss of 80 to 90% of dopaminergic production in the substantia nigra Lewy Bodies

5
Degeneration of dopaminergic neurons in the substantia nigra. Dopamine 5

6
Symptoms caused by insufficient dopamine. 3 main symptoms: TremorsRigidity Slowed motion (Bradykinesia) Other symptoms include: Dementia, sleep disturbances, depression, etc. 6
 Other symptoms include: Dementia, sleep disturbances, depression, etc. 6.")
7
Degenerative disease of the basal ganglia causing tremor at rest, muscle rigidity hypokinesia, often with dementia. Associated with aggregation of α-synuclein (a protein normally involved in vesicle recycling) in the form of characteristic Lewy bodies. Often idiopathic but may follow stroke or virus infection; can be drug-induced (neuroleptic drugs). Rare familial forms also occur, associated with various gene mutations, including α- synuclein. Associated with early degeneration of dopaminergic nigrostriatal neurons, followed by more general neurodegeneration. Can be induced by 1-methyl-4-phenyl-1,2,3,6- tetrahydropyridine (MPTP), a neurotoxin affecting dopamine neurons. Similar environmental neurotoxins, as well as genetic factors, may be involved in human Parkinson's disease.
 in the form of characteristic Lewy bodies. Often idiopathic but may follow stroke or virus infection; can be drug-induced (neuroleptic drugs). Rare familial forms also occur, associated with various gene mutations, including α- synuclein. Associated with early degeneration of dopaminergic nigrostriatal neurons, followed by more general neurodegeneration. Can be induced by 1-methyl-4-phenyl-1,2,3,6- tetrahydropyridine (MPTP), a neurotoxin affecting dopamine neurons. Similar environmental neurotoxins, as well as genetic factors, may be involved in human Parkinson s disease..")
9
PARKINSON'S is a progressive disorder of movement that occurs mainly in the elderly. The chief symptoms are: tremor at rest, usually starting in the hands which tends to diminish during voluntary activity muscle rigidity, detectable as an increased resistance in passive limb movement suppression of voluntary movements (hypokinesis), due partly to muscle rigidity and partly to an inherent inertia of the motor system, which means that motor activity is difficult to stop as well as to initiate.
, due partly to muscle rigidity and partly to an inherent inertia of the motor system, which means that motor activity is difficult to stop as well as to initiate..")
10
Parkinsonian patients walk with a characteristic shuffling gait. They find it hard to start, and once in progress they cannot quickly stop or change direction. PD is commonly associated with dementia, probably because the degenerative process is not confined to the basal ganglia but also affects other parts of the brain.

11
Parkinson's disease often occurs with no obvious underlying cause, but it may be the result of cerebral ischaemia, viral encephalitis or other types of pathological damage.

12
The symptoms can also be drug-induced, the main drugs involved being those that reduce the amount of dopamine in the brain (e.g. reserpine) or block dopamine receptors (e.g. antipsychotic drugs such as chlorpromazine;).
 or block dopamine receptors (e.g. antipsychotic drugs such as chlorpromazine;)..")
13
There are rare instances of early-onset PD that runs in families, and several gene mutations have been identified, the most important being synuclein and parkin. Study of these gene mutations has given some clues about the mechanism underlying the neurodegenerative process

14
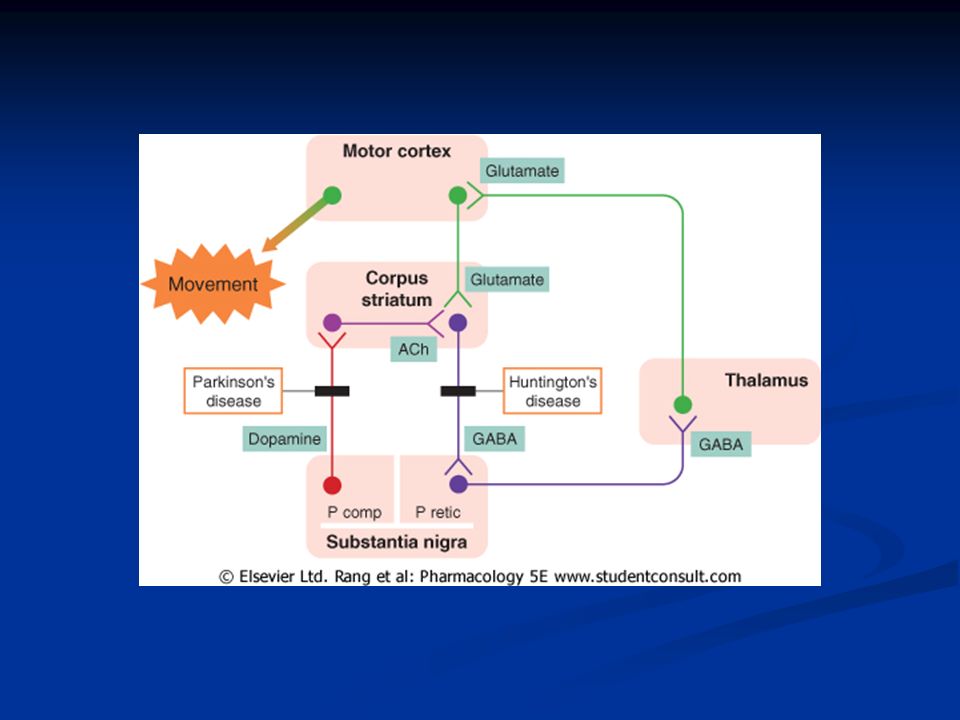
Pathophysiology Motor system-fine balance of inhibitory and excitatory inputs of basal ganglia and cerebellum Cerebellar output is excitatory, basal ganglia is inhibitory

15
Pathophysiology Apoptosis of dopaminergic neurons in substantia nigra-leads to decrease in inhibition Disruption of signals to motor cortex via thalamus Smooth, coordinated movement is lost

17
Neurotoxins In 1982, a group of young drug addicts in California suddenly developed an exceptionally severe form of PD (known as the 'frozen addict' syndrome), and the cause was traced to the compound 1-methyl-4-phenyl-1,2,3,6- tetrahydropyridine (MPTP), which was a contaminant in a preparation used as a heroin substitute. MPTP causes irreversible destruction of nigrostriatal dopaminergic neurons in various species, and produces a PD-like state in primates. MPTP acts by being converted to a toxic metabolite, MPP+, by the enzyme monoamine oxidase (MAO, specifically by the MAO-B subtype). MPP+ is taken up by the dopamine transport system, and thus acts selectively on dopaminergic neurons; it inhibits mitochondrial oxidation reactions, producing oxidative stress
. MPP+ is taken up by the dopamine transport system, and thus acts selectively on dopaminergic neurons; it inhibits mitochondrial oxidation reactions, producing oxidative stress.")
18
MPTP appears to be selective in destroying nigrostriatal neurons and does not affect dopaminergic neurons elsewhere-the reason for this is unknown. Selegiline, a selective MAO-B inhibitor,prevents MPTP- induced neurotoxicity by blocking its conversion to MPP+. Selegiline is also used in treating PD as well as inhibiting dopamine breakdown, it might also work by blocking the metabolic activation of a putative endogenous, or environmental, MPTP-like substance, which is involved in the causation of PD. It is possible that dopamine itself could be the culprit, because oxidation of dopamine gives rise to potentially toxic metabolites.

19
Whether or not the action of MPTP reflects the natural pathogenesis of PD, the MPTP model is a very useful experimental tool for testing possible therapies. Various herbicides, such as rotenone, that selectively inhibit mitochondrial function cause a PD-like syndrome in animals, suggesting that environmental toxins could be a factor in human PD, because impaired mitochondrial function is a feature of the disease in humans.

20
What is an animal model? A laboratory animal used in research that simulates processes comparable to those that occur in humans.

22
Two common animal models. Lab rats. Vertebrate model Somehow resistant to MPTP Rotenone administered systemically - Chronic nigrostriatal cell loss, dopamine depletion, Akinesia, rigidity, tremor, flexed posture, piloerection. Fruit flies. Invertebrate model Dopamine is depleted. But is reversible by Hsp70 coexpression. Is there any use for this in human model?

23
Pharmacotherapy Levodopa Dopamine agonists COMT inhibitors Amantadine Anticholinergics Rasagiline MAO-B inhibitor ex. Selegiline, Rasagiline

25
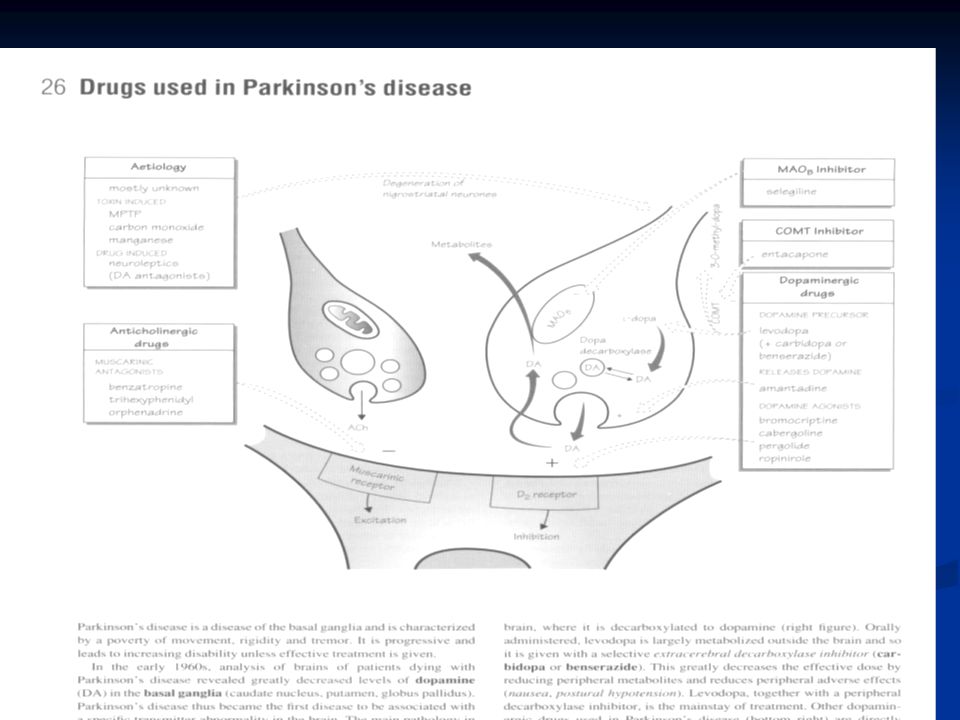
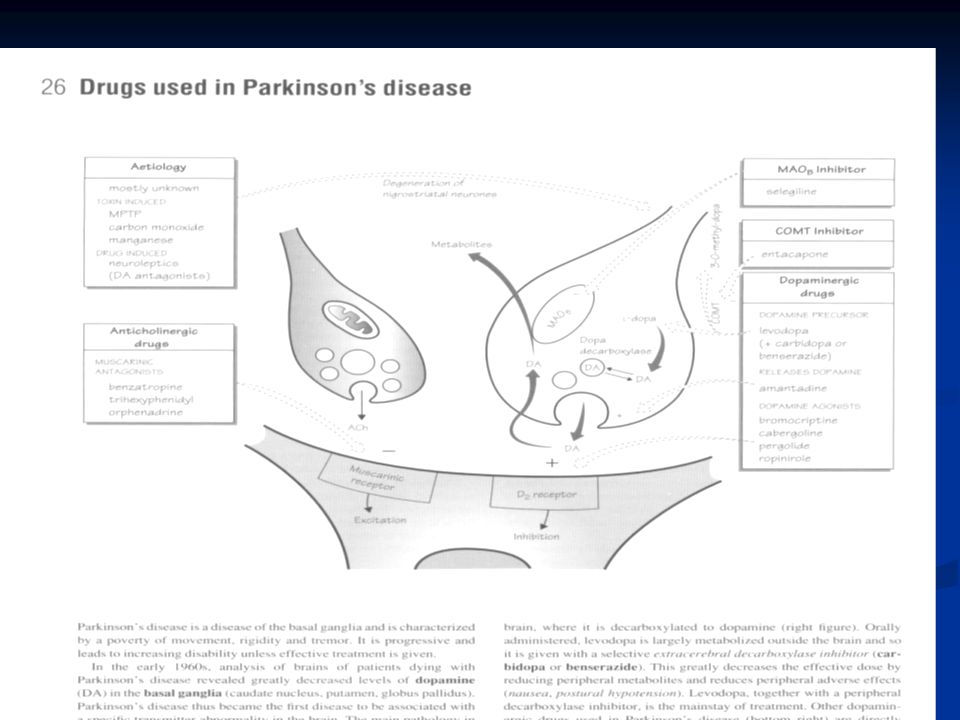
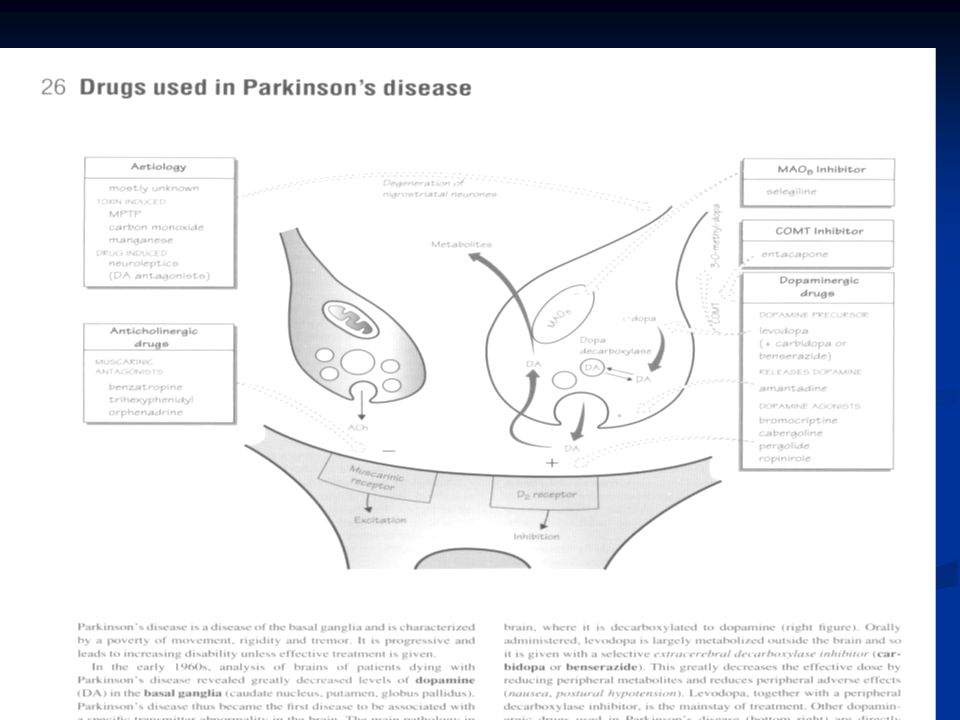
Drugs used in Parkinson'sdisease Drugs act by counteracting deficiency of dopamine in basal ganglia or by blocking muscarinic receptors. None of the available drugs affect the underlying neurodegeneration.

26
Drugs include: levodopa (dopamine precursor;), given with an inhibitor of peripheral dopa decarboxylase (e.g. carbidopa ) to minimise side effects; sometimes a catechol-O-methyltransferase inhibitor (e.g. entacapone ) is also given, especially to patients with 'end of dose' motor fluctuations
 to minimise side effects; sometimes a catechol-O-methyltransferase inhibitor (e.g. entacapone ) is also given, especially to patients with end of dose motor fluctuations.")
27
bromocriptine (dopamine agonist;) selegiline (monoamine oxidase B inhibitor) amantadine (which may enhance dopamine release) benztropine (muscarinic receptor antagonist used for parkinsonism caused by antipsychotic drugs). Neurotransplantation, still in an experimental phase, may be effective but results are variable.

28
levodopa

29
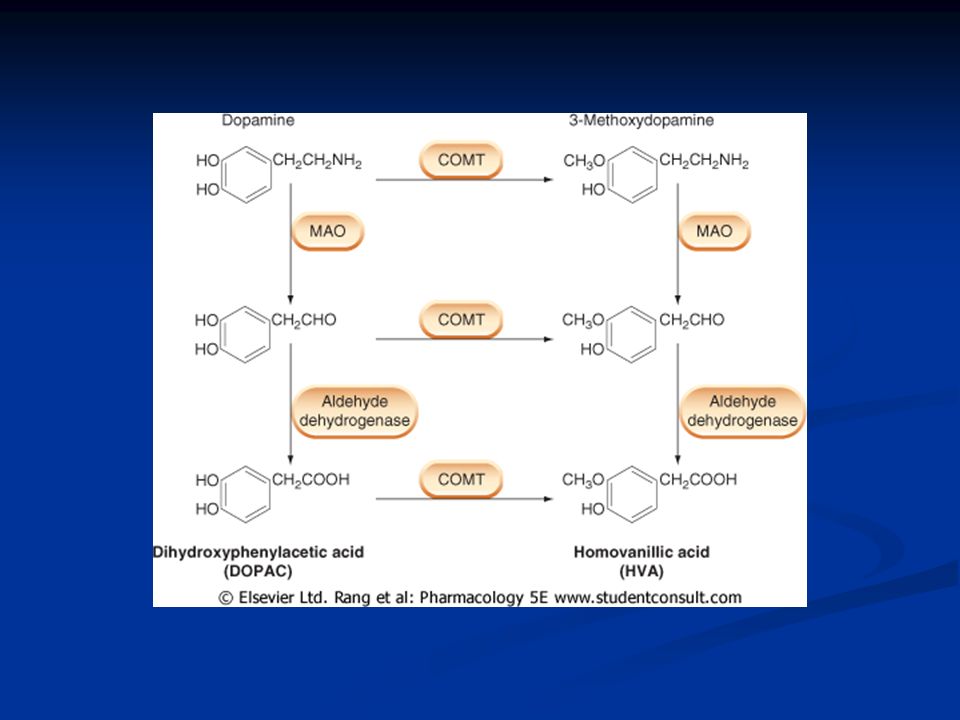
Dopamine is a neurotransmitter as well as being the precursor for noradrenaline. It is degraded in a similar fashion to noradrenaline, giving rise mainly to dihydroxyphenylacetic acid and homovanillic acid, which are excreted in the urine. There are three main dopaminergic pathways: nigrostriatal pathway, important in motor control mesolimbic/mesocortical pathways, running from groups of cells in the midbrain to parts of the limbic system, especially the nucleus accumbens, and to the cortex; they are involved in emotion and drug-induced reward systems

30
tuberohypophyseal neurons running from the hypothalamus to the pituitary gland, whose secretions they regulate

31
levodopa levodopa (dopamine precursor;), given with an inhibitor of peripheral dopa decarboxylase (e.g. carbidopa ) to minimise side effects; sometimes a catechol-O- methyltransferase inhibitor (e.g. entacapone ) is also given, especially to patients with 'end of dose' motor fluctuations
 to minimise side effects; sometimes a catechol-O- methyltransferase inhibitor (e.g. entacapone ) is also given, especially to patients with end of dose motor fluctuations.")
32
Levodopa L-Dopa (Larodopa by Roche) Introduced in the late 1960s Crosses the blood-brain barrier Adverse effects such as nausea, vomiting, postural hypotension, involuntary movements, restlessness, and cardiac arrhythmias
 Introduced in the late 1960s Crosses the blood-brain barrier Adverse effects such as nausea, vomiting, postural hypotension, involuntary movements, restlessness, and cardiac arrhythmias")
35
Dopamine Agonists “ Synthetic Dopamine ” Bromocriptine Mesylate (Parlodel) Pergolide Mesylate (Permax) Pramipexol (Mirapex) Ropinirole HCL (Requip) Rotigotine Rotigotine
 Pergolide Mesylate (Permax) Pramipexol (Mirapex) Ropinirole HCL (Requip) Rotigotine Rotigotine")
36
Dopamine Agonists Monotherapy or combination Are particulary usefull for: Prolonging the effective treatment period in patients with deteriorating response. Delaying the onset of L-dopa therapy. Particularly in younger patients. Treating patients who cannot tolerate high doses of L-dopa. Associated with more side effects than L-dopa Potential adverse effects include somnolence, dyskinesias, nausea, vomiting, orthostatic hypotension, nightmares, hallucinations, confusion, dizziness

37
COMT Inhibitors Entacapone (Comtan) Tolcapone (Tasmar)
 Tolcapone (Tasmar)")
38
COMT Inhibitor Entacapone (Comtan) Adjunct therapy Initial dose of 200mg with each dose of levodopa up to 8 times daily Decrease of L-dopa may be necessary Exacerbation of L-dopa side effects, diarrhea, urine discoloration, abdominal pain
 Adjunct therapy Initial dose of 200mg with each dose of levodopa up to 8 times daily Decrease of L-dopa may be necessary Exacerbation of L-dopa side effects, diarrhea, urine discoloration, abdominal pain")
39
COMT Inhibitor Tolcapone (Tasmar) Adjunct therapy Initial 100mg TID up to 200mg TID More potent and longer acting than entacapone Decrease L-dopa by 25 to 50% Exacerbation of L-dopa side effects, diarrhea, urine discoloration, liver toxicity.
 Adjunct therapy Initial 100mg TID up to 200mg TID More potent and longer acting than entacapone Decrease L-dopa by 25 to 50% Exacerbation of L-dopa side effects, diarrhea, urine discoloration, liver toxicity.")
40
Amantadine Amantadine HCL (Symmetrel) Inhibits dopamine recapture Blocks acetylcholine and glutamate receptors Dose 100mg BID to TID Caution in renal failure patients Currently used to reduce choreic movements Narrow therapeutic range Unpleasant side effects such as nausea, dizziness, confusion, hallucinations, nightmares, dry mouth peripheral edema.
 Inhibits dopamine recapture Blocks acetylcholine and glutamate receptors Dose 100mg BID to TID Caution in renal failure patients Currently used to reduce choreic movements Narrow therapeutic range Unpleasant side effects such as nausea, dizziness, confusion, hallucinations, nightmares, dry mouth peripheral edema.")
41
Anticholinergics Trihexyphenidyl HCL (Artane) Benztropine Mesylate (Cogentin) Monotherapy or adjunct most effective for reducing tremor Use Limited by side effects especially in the elderly.
 Benztropine Mesylate (Cogentin) Monotherapy or adjunct most effective for reducing tremor Use Limited by side effects especially in the elderly.")
42
Anticholinergics Trihexyphenidyl HCL (Artane) Initial dose of 1mg and increase by 2 mg every 3 to 5 days until 6 to 10 mg/day. Usually given TID with meals or QID with meals and at bedtime. Possible adverse effects include dry mouth, blurred vision, somnolence, hallucinations, memory impairment, confusion, urinary retention, and constipation. Benztropine Mesylate (Cogentin) Initial dose of 0.5 to 1 mg at bedtime. Increase by 0.5mg every 5 to 6 days up to a total daily dosage of 6mg. Possible adverse effects include dry mouth, blurred vision, somnolence, hallucinations, memory impairment, confusion, urinary retention, and constipation.
 Initial dose of 0.5 to 1 mg at bedtime. Increase by 0.5mg every 5 to 6 days up to a total daily dosage of 6mg. Possible adverse effects include dry mouth, blurred vision, somnolence, hallucinations, memory impairment, confusion, urinary retention, and constipation..")
43
Selegiline Selegiline HCL(Eldepryl)
")
44
Selegiline Monotherapy or adjunct MOA-inhibits monoamine oxidase-B (MAO-B) Inhibition of MAO-A does not occur Dosage of 5 mg BID with breakfast and lunch When used as monotherapy delays the need of L-dopa by an average of nine months. Possible adverse effects include nausea, dizziness, abdominal pain, confusion, and exacerbation of L-dopa side effects Controversial theory of decreased rate of neuronal death due to a reduction of free radicals.

45
Surgical Options Pallidotomy and Pallidal Stimulation Thalamotomy and Thalamic Stimulation Introduced in 1950 Pallidotomy improves tremor, rigidity, and bradykinesia Thalamotomy relieves tremor, rigidity, but not bradykinesia Neurosurgical treatment came to a end with the introduction of L-dopa in late 1960s Resurgence of neurosurgical intervention with the failure of pharmacological treatments after 10 to 15 years of disease progression Two methods: Ablation and deep brain stimulation

46
Surgery - Deep Brain Stimulation Brain pacemaker, sends electrical impulses to brain to stimulate the subthalamic nucleus. Improves motor functions and reduce motor complications. Complications include: brain hemorrhage, seizures, death. 46

47
Surgery... Deep Brain Stimulation (DBS) Reduces distressing symptoms such as rigidity. Tiny wire electrodes are implanted in the Basal Ganglia. They are connected to an Implantable Pulse Generator in the chest. Turn pulse on: symptoms reduce. Turn pulse off: symptoms return. Cost €40,000 to €50,000! Ideal candidates are younger and fit. Must have no history of severe depression.

48
Grafting Suprarenal to brain transplantation Fetal tissue transplantation Cell culture transplantation

49
Under Investigation Implantable pumps Implantable capsules containing dopamine- producing cells New medications to target one of the five individual brain receptors for dopamine Continued genetic research

50
What does the future hold? Stem cell research... scientists are creating dopamine-producing neural cells. These can be injected into patients brain to reverse the effects of Parkinson's. BUT - Will the injected cells be accepted by the patient? Or will they be destroyed in a natural immune response. Or will they be destroyed in a natural immune response. This research is ongoing. It may take 20 years before it is ready for widespread use.

Similar presentations

>")





>")











