Download presentation
Presentation is loading. Please wait.

1
Here at TMC

2
2

3
3

4
Healthcare Associated Infection Definition: –A localized or systemic condition resulting from an adverse reaction to the presence of an infectious agent(s) or its toxin(s). –There must be no evidence that the infection was present or incubating at the time of admission to the care setting. –Clinical evidence may be derived from direct observation of the infection site or review of information in the patient chart or other clinical records. CDC

5
The Bundles of Care Prevent Healthcare Associated Infection It is a small straightforward set of practices – generally three to five – that, when performed collectively, reliably and continuously, have been proven to improve patient outcomes.

6
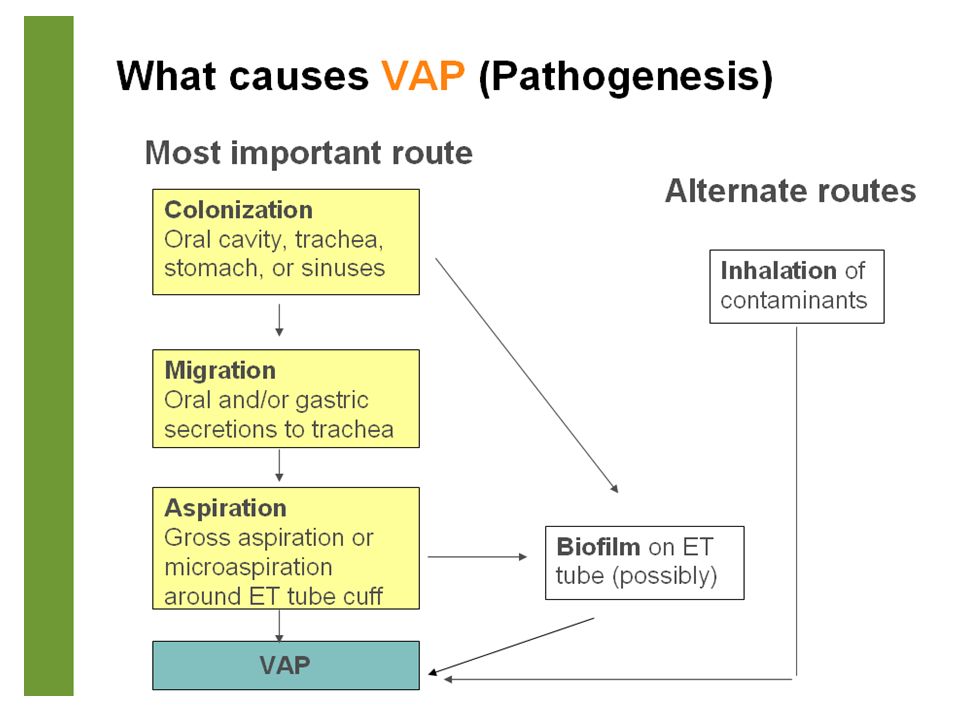
Ventilator Associated Pneumonia (VAP) Patient was intubated and ventilated at the time of or within 48 hours before the onset of the event NOTE: There is no minimum period of time that the ventilator must be in place in order for the PNEU to be considered ventilator-associated.
 Patient was intubated and ventilated at the time of or within 48 hours before the onset of the event NOTE: There is no minimum period of time that the ventilator must be in place in order for the PNEU to be considered ventilator-associated.")
9
The Bundles of Care in the Prevention of Ventilator Associated Pneumonia (VAP) Details of CareResponsibility Hand hygiene before and after touching the patient RN MD Oral hygiene every after suctioning, turning to sides and feeding session RN Use suction catheter only ONCE or use Closed Suction System for 72hrs RN If there is no contraindication, elevate the head of bed at an angle of 30 – 45 0 RN MD Use of Endotracheal tube with subglottic suction MD Always check proper placement of feeding tube RN Assess patient’s intestinal motility RN Use daily sedation vacations and assess the patient’s readiness to extubate MD Decrease pH of gastric content – give peptic ulcer disease prophylaxis MD Include deep vein thrombosis prophylaxis MD Remove devices such as ET, tracheostomy and/or enteral tubes from patients as soon as the clinical indications for these are resolved. MD

10
Central Line Associated Bloodstream Infection (CLABSI) CLABSI: A central line or umbilical catheter was in place at the time of, or within 48 hours before, onset of the event NOTE: There is no minimum period of time that the central line must be in place in order for the BSI to be considered central line-associated. Central line: An intravascular catheter that terminates at or close to the heart or in one of the great vessels which is used for infusion, withdrawal of blood, or hemodynamic monitoring.

11
Central Line Associated Bloodstream Infection (CLABSI) Definition: Presence of Central line 1. Patient has a recognized pathogen cultured from 1 or more blood cultures and organism cultured from blood is not related to an infection at another site. 2. Patient has at least 1 of the following signs or symptoms: fever (38.8C), chills, or hypotension and signs and symptoms and positive laboratory results are not related to an infection at another site and common skin contaminant (ie, diphtheroids [Corynebacterium spp], Bacillus [not B anthracis] spp, Propionibacterium spp, coagulase-negative staphylococci [including S epidermidis], viridans group streptococci, Aerococcus spp, Micrococcus spp) is cultured from 2 or more blood cultures drawn on separate occasions.
, chills, or hypotension and signs and symptoms and positive laboratory results are not related to an infection at another site and common skin contaminant (ie, diphtheroids [Corynebacterium spp], Bacillus [not B anthracis] spp, Propionibacterium spp, coagulase-negative staphylococci [including S epidermidis], viridans group streptococci, Aerococcus spp, Micrococcus spp) is cultured from 2 or more blood cultures drawn on separate occasions..")
12
Central Line Associated Bloodstream Infection (CLABSI) Definition: Presence of Central line 3. Patient #1 year of age has at least 1 of the following signs or symptoms: fever (38.8C, rectal), hypothermia (37.8C, rectal), apnea, or bradycardia and signs and symptoms and positive laboratory results are not related to an infection at another site and common skin contaminant (ie, diphtheroids [Corynebacterium spp], Bacillus [not B anthracis] spp, Propionibacterium spp, coagulasenegative staphylococci [including S epidermidis], viridans group streptococci, Aerococcus spp, Micrococcus spp) is cultured from 2 or more blood
, hypothermia (37.8C, rectal), apnea, or bradycardia and signs and symptoms and positive laboratory results are not related to an infection at another site and common skin contaminant (ie, diphtheroids [Corynebacterium spp], Bacillus [not B anthracis] spp, Propionibacterium spp, coagulasenegative staphylococci [including S epidermidis], viridans group streptococci, Aerococcus spp, Micrococcus spp) is cultured from 2 or more blood.")
13
Implantable Central Catheter

14
PICC

15
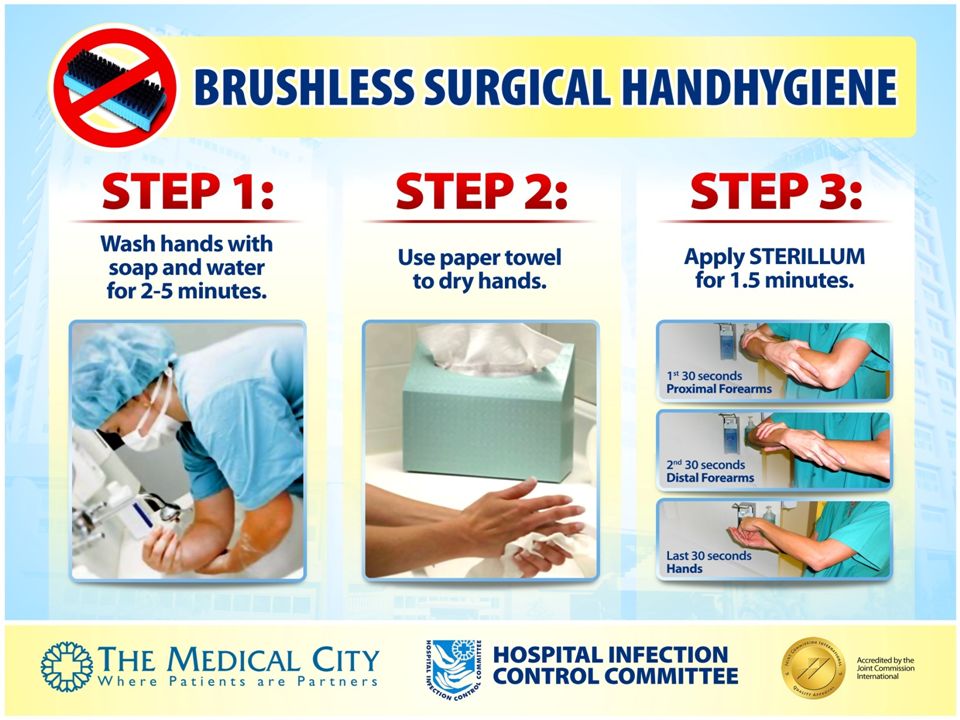
Infection Control Requirement for Central Line Insertion 1.Wash hands with soap and water; DRY with paper towel; Apply Sterillum from elbow up to hands for 1.5 minutes until dry. 2.Wear cap, mask, protective eyewear and sterile gown properly. 3. Wear sterile gloves. 4. Cleanse the insertion area with POVIDONE + ALCOHOL (Surgistat) from the insertion site in circular motion outward. Remove dripping and wait to dry. Do not wipe the painted area. 5. Place the sterile large drape exposing the operative site and fully covers the head down to toe. 7. Resident Assist should accomplish Central Line Insertion Checklist.
 from the insertion site in circular motion outward. Remove dripping and wait to dry. Do not wipe the painted area. 5. Place the sterile large drape exposing the operative site and fully covers the head down to toe. 7. Resident Assist should accomplish Central Line Insertion Checklist..")
16
NIC on the floor shall attach this CLIP Form to the Patient Chart if Central Line insertion shall be done in OR ICU, ACSU, ER insertion, the CLIP FORM is attached to the package prepared by CPU. Make sure that the form is properly filled –up by the RIC.

17
The ICN fill-up the form and attach to chart then inform NIC about the Discharge Instruction. The RIC/AP shall fill- up the gray part on the day of discharge. The NIC shall detach the lower portion of the form and give it to the patient on the day of discharge but retain the upper portion on the chart. ICN will get the form to MID.

18
CHECKLIST FOR CARE AND MAINTENANCE OF CENTRAL & IV LINES 1. Mandatory HANDHYGIENE before and after Central Line (CL) access or manipulation. 2.Access CL ports aseptically. Cleanse with 70% alcohol for at least 15 seconds, wait to dry. Use ONLY sterile device. 3.Wear sterile gloves and mask whenever accessing a CL or performing CL care. 4.All CL in place but not currently being infused are to be flushed according to procedure for CL and Implanted Ports i.e. Heparin/Normal Saline Flush. 5.The IV tubing, add-on extension sets and stop cocks in use must be changed maximum of 7 days when used for medications and IV fluids only. 6.Change needleless access ports for locked CL every 72 to 96 hours. 7.Patients with parenteral nutrition should have dedicated access port and tubing changed every 24 hours. 8.Change of CL dressing: – every 7 days for transparent dressing if there is no visible soiling – every 48 hours for gauze dressing (Note: gauze under a transparent dressing is a gauze dressing). – when the integrity of dressing is compromised or when the dressing is non- occlusive. – when catheter is replaced. 9.Document IV tubing and CL changes in the KARDEX. (Nurse responsibility)
 access or manipulation. 2.Access CL ports aseptically. Cleanse with 70% alcohol for at least 15 seconds, wait to dry. Use ONLY sterile device. 3.Wear sterile gloves and mask whenever accessing a CL or performing CL care. 4.All CL in place but not currently being infused are to be flushed according to procedure for CL and Implanted Ports i.e. Heparin/Normal Saline Flush. 5.The IV tubing, add-on extension sets and stop cocks in use must be changed maximum of 7 days when used for medications and IV fluids only. 6.Change needleless access ports for locked CL every 72 to 96 hours. 7.Patients with parenteral nutrition should have dedicated access port and tubing changed every 24 hours. 8.Change of CL dressing: – every 7 days for transparent dressing if there is no visible soiling – every 48 hours for gauze dressing (Note: gauze under a transparent dressing is a gauze dressing). – when the integrity of dressing is compromised or when the dressing is non- occlusive. – when catheter is replaced. 9.Document IV tubing and CL changes in the KARDEX. (Nurse responsibility).")
19
Catheter Associated UTI (CAUTI) Patient had an indwelling urinary catheter at the time of or within 48 hours before onset of the event NOTE: There is no minimum period of time that the catheter must be in place in order for the UTI to be considered catheter- associated.
 Patient had an indwelling urinary catheter at the time of or within 48 hours before onset of the event NOTE: There is no minimum period of time that the catheter must be in place in order for the UTI to be considered catheter- associated.")
20
The Bundles of Care in the Prevention of Catheter Associated Urinary Tract Infection (CAUTI) Details of CareResponsibility Hand hygiene before and after handling the system RN MD Insert catheter only when necessary MD Insert catheter using aseptic technique and sterile equipment MD Secure catheter with a tape at inner thigh for female and left or right hypogastric area for male RN Maintain closed sterile drainage RN Maintain unobstructed urine flow RN Aspirate urine samples aseptically from the catheter without opening the system RN Always keep the catheter bag lower than the level of the bladder but should not touch the floor. RN

21
Identifying a Surgical Site Infection 1 Incisional Site Infections Superficial Superficial Deep Deep Organs/Space Infections Mangram, AJ, et.al. 1999. Guideline for Prevention of SSI. Infection Control and Hospital Epidemiology. 20(4)
.")
22
Surgical Site Infection A superficial incisional SSI must meet one of the following criteria: Infection occurs within 30 days after the operative procedure and involves only skin and subcutaneous tissue of the incision and patient has at least one of the following: a. purulent drainage from the superficial incision. b. organisms isolated from an aseptically obtained culture of fluid or tissue from the superficial incision. c.at least one of the following signs or symptoms of infection: pain or tenderness, localized swelling, redness, or heat, and superficial incision is deliberately opened by surgeon, and is culture-positive or not cultured. A culture-negative finding does not meet this criterion. d. diagnosis of superficial incisional SSI by the surgeon or attending physician.

23
A deep incisional SSI must meet on of the following criteria: Infection occurs within 30 days after the operative procedure if no implant is left in place or within one year if implant is in place and the infection appears to be related to the operative procedure and involves deep soft tissues (e.g., fascial and muscle layers) of the incision and patient has at least one of the following: a. purulent drainage from the deep incision but not from the organ/space component of the surgical site b. a deep incision spontaneously dehisces or is deliberately opened by a surgeon and is culture-positive or not cultured when the patient has at least one of the following signs or symptoms: fever (>38°C), or localized pain or tenderness. A culture-negative finding does not meet this criterion. c. an abscess or other evidence of infection involving the deep incision is found on direct examination, during reoperation, or by histopathologic or radiologic examination
, or localized pain or tenderness. A culture-negative finding does not meet this criterion. c. an abscess or other evidence of infection involving the deep incision is found on direct examination, during reoperation, or by histopathologic or radiologic examination.")
24
An organ/space SSI must meet one of the following criteria: Infection occurs within 30 days after the operative procedure if no implant is left in place or within one year if implant is in place and the infection appears to be related to the operative procedure and infection involves any part of the body, excluding the skin incision, fascia, or muscle layers, that is opened or manipulated during the operative procedure and patient has at least one of the following: a. purulent drainage from a drain that is placed through a stab wound into the organ/space b. organisms isolated from an aseptically obtained culture of fluid or tissue in the organ/space c. an abscess or other evidence of infection involving the organ/space that is found on direct examination, during reoperation, or by histopathologic or radiologic examination d. diagnosis of an organ/space SSI by a surgeon or attending physician.

25
The ICN fill-up the form and attach to chart then inform NIC about the Discharge Instruction. The RIC/AP shall fill- up the gray part on the day of discharge. The NIC shall detach the lower portion of the form and give it to the patient on the day of discharge but retain the upper portion on the chart. ICN will get the form to MID.

26
The Bundles of Care in the Prevention of Surgical Site Infection (SSI) Details of CareResponsibility Oral Care including cleaning of tongueRN 4% Chlorhexidine bath: first on the night of surgery and second on the morning before surgery and must wear hospital gown RN Use of C LIPPER in removing hairs RN Administration of A NTIBIOTIC Prophylaxis 60 minutes prior to skin incision or immediately after induction of anaesthesia MD Maintain normal body T EMPERATURE RN Maintain normal level of blood S UGAR MD
 Details of CareResponsibility Oral Care including cleaning of tongueRN 4% Chlorhexidine bath: first on the night of surgery and second on the morning before surgery and must wear hospital gown RN Use of C LIPPER in removing hairs RN Administration of A NTIBIOTIC Prophylaxis 60 minutes prior to skin incision or immediately after induction of anaesthesia MD Maintain normal body T EMPERATURE RN Maintain normal level of blood S UGAR MD")
27
Basic Wound Dressing Change dressing of surgical wound after 48 hours after the procedure if no soiling is observed. Prepare materials for use including yellow waste bin. Wash hands with soap and water then dry OR use Alcohol-based handrub. Wear surgical mask and clean gloves. If splashes is anticipated, wear long sleeve green gown properly. Remove dressing, note for the appearance of the incision site like discharge, etc. If the dressing sticks, wet with sterile water or NSS to loosen. Throw the old dressing into the waste bin together with the gloves used. Wash hands again with soap and water then dry OR use Alcohol-based handrub. Put on sterile gloves. Clean the surrounding of the incision site with gauze wet with NSS: dab or wipe gently to remove dried blood or material. Observe the wound if needing new dressing or not. NOTE: Change gloves when moving to other body sites. Waste generated should be disposed properly at the point of care. Document the procedure.

Similar presentations





 CATHETER RELATED URINARY TRACT INFECTIN (CR-UTI)>")

>")



>")








 449-9330>")