Download presentation
Presentation is loading. Please wait.

1
Postpartum Hemorrhage
Abdulah Al-Tayyem;MD;JBOG Consultant Ob&Gyn Urogynaecology Zarka Govern. Hospital

2
PPH: excessive blood loss after delivery sufficient to affect the general condition of the mother
(tachycardia and or hypotension). Types: -primary within 24h -secondary after the first 24h up to 42nd day
. Types: -primary within 24h. -secondary after the first 24h up to 42nd day.")
3
Causes -uterine atony -genital trauma -coagulations disorders
-3rd stage complications: -mismanagement of the 3rd stage of labour -acute inversion of the uterus -abnormal or incomplete placental separation

4
Factors predispose to uterine atony
Overdistended uterus:-polyhydramnios -macrosomia -multiple pregnancy Uterine muscle exhaustion: -prolonged labour -grand multiparity -precipitate labour Intrauterine infection: -prolonged ROM -chorioamionitis Functional or anatomic distortion of the uterus: -fibroid uterus – placenta previa –uterine anomalies Certain general anesthetics( halothane) History of previous PPH
 History of previous PPH.")
5
Factors predispose to genital tract trauma
A precipitate delivery, or an operative or manipulative delivery predispose the genital tract to lacerations : -cervix vagina -perineum Malposition ,malpresentations or deep engagement of the fetal head ) CS,instrumental deliveries) Previous uterine surgery Abuse of oxytocin
 CS,instrumental deliveries) Previous uterine surgery. Abuse of oxytocin.")
6
Factors predispose to retained product of conception
An incomplete placenta at delivery Previous uterine surgery Multiparity An abnormal placenta on US Intrauterine infections may lead to adherent placenta

7
Abnormalities of coagulation
Hemophilia A or Von Willebrad’s disease Idiopathic thrombocytopenic purpura(ITP) History of liver disease Use of anticoagulants Acquired in pregnancy: -thrombocytopenia with PET(HELLP syndrome) -DIC caused by: -abruptio placentae -chorioamionitis -IUFD
 History of liver disease. Use of anticoagulants. Acquired in pregnancy: -thrombocytopenia with PET(HELLP syndrome) -DIC caused by: -abruptio placentae. -chorioamionitis. -IUFD.")
8
Diagnosis History taking Physical examination
tachycardia and hypotension my be present without evidence of excessive blood loss in cases of uterine rupture Consistency of the uterus( lax,firm) Asses amount of vaginal bleeding Look for laceration Determine whether the placenta has been delivered
 Asses amount of vaginal bleeding. Look for laceration. Determine whether the placenta has been delivered.")
9
In women with hypertension or pre-eclampsia,
severe blood loss may cause a misleading normal blood pressure reading and an under diagnosed state of shock

10
Degree of Hemorrhagic Shock
Symptom Systolic B.P Volume loss %of B.V Grade type Palpitation dizziness normal ml (10-15%) Grade 1 compensated Weakness sweating Slight fall ml (15-25%) Grade 2 Restlessness, pallor,oliguria 70-80 mmHg ml (25-35%) Grade 3 Collapse,anuria Shortness off breath 50-70 mmHg ml (35-45%) Grade 4
 Grade 1. compensated. Weakness. sweating. Slight fall ml. (15-25%) Grade 2. Restlessness, pallor,oliguria mmHg ml. (25-35%) Grade 3. Collapse,anuria. Shortness off breath mmHg ml. (35-45%) Grade 4.")
11
Investigations : as in APH
After the history and physical examination are completed, the cause of PPH can be determined as follow:

12
Diagnosis off PPH Probable diagnosis
Symptoms and sings sometimes present Symptoms and sings typically present Atonic uterus shock Primary PPH , Uterus soft and not contracted Tears of cervix, Vagina or perineum Complete placenta Uterus contracted Primary PPH Retained placenta Placenta not delivered with 30 min after delivery Immediate PPH Portion of the maternal surface of the placenta missing or torn membranes with vessels

13
Diagnosis off PPH Probable diagnosis
Symptoms and sings sometimes present Symptoms and sings typically present Retained placental fragments Inverted uterus apparent at vulva Primary PPH Uterine fundus not felt on abd.palpation Slight or intense pain Rupture uterus Amount of bleeding is not related to the degree of shock Tender abdomen Rapid maternal pulse State of shock Primary PPH) bleeding intraabdominal a/o vaginal) Severe abdominal pain(may decrease after ruptrure Secondary PPH Bleeding is variable) light to heavy,continuous or irregular) and may be foul-smellig Anemia Fever Bleeding occurs more than 24h after delivery Uterus softer and larger than expected for time since delivery
 bleeding intraabdominal a/o vaginal) Severe abdominal pain(may decrease after ruptrure. Secondary PPH. Bleeding is variable) light to heavy,continuous or irregular) and may be foul-smellig. Anemia Fever. Bleeding occurs more than 24h after delivery. Uterus softer and larger than expected for time since delivery.")
14
Management Preventive are during the antenatal period.
Preventive care during labour and delivery. Emergency rules First aid management Use of utertonic agents :oxytocin,misoprostol

15
Active Management Placenta retained: manual removal under adequate anesthesia. Uterine inversion reposition of the uterus Placenta delivered: -uterus soft use oxytocin -exploration under general anesthesia , repair any cervical tears. -tear extends beyond the vaginal vault do laparotomy.

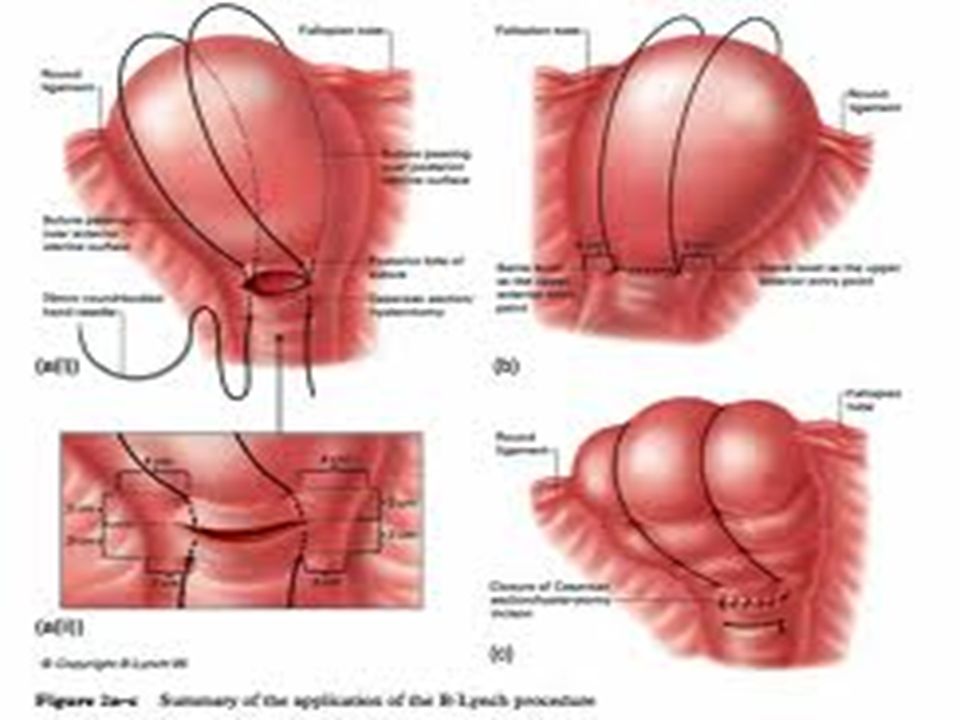
18
At Lapatotomy : Surgical compression suture-(Lynch suture)
Balloon tamponade Surgical repair Ligation of the uterine ,utero-ovarian or hypogastric arteries Subtotal hysterectomy

20
Important Considerations
Remember that a postpartum women can lose a large amount of blood in a very short time. You must act promptly and anticipate complications Assure adequate team coverage A laparotomy for PPH is an extremely urgent situation, do not delay while waiting for blood transfusion. Administer prophylactic antibiotics, Ampicillin 2 gm IV ,before and after the procedure Do not give oxytocin as an undiluted IV push since the women may collapse

21
Thank you

Similar presentations



: leading cause of maternal mortality worldwide Prevalence rate: 6% Africa has highest prevalence.>")


 产后出血 林建华. Major causes of death for pregnancy women ( maternal mortality) Postpartum hemorrhage ( 28%) heart diseases pregnancy-induced.>")


 and abnormalities of the Third Stage Sept 12 – Dr. Z. Malewski.>")











