Download presentation
Presentation is loading. Please wait.

1
IVF - ICSI ÖNCESİ ENDOMETRIOMALAR ÇIKARTILMALI MI? Prof. Dr. Bülent Baysal İ.Ü. İstanbul Tıp Fakültesi

2
ENDOMETRİOZİS 17.yy...............peritoneal ülser 1860..............Von Rokitansky (mikroskopik tanı)
")
3
Prevalans: kadınların %5 inde, infertilite problemi olan kadınların %30-50 sinde

6
Impact of ovarian endometrioma on oocytes and pregnancy outcome in in vitro fertilization. Suzuki T, et al. Fertil Steril 2005 Group A: 80 cycles with ovarian endometriomas; group B: 248 cycles with endometriosis - without endometrioma group C: 283 cycles - tubal factor. Fewer oocytes were retrieved from groups A and B than from group C (P<.005). pregnancy rates (group A: 25.3%, group B: 22.3%, group C: 23.9%). CONCLUSIONS: Endometriosis affects oocyte number but not embryo quality or pregnancy outcome
. pregnancy rates (group A: 25.3%, group B: 22.3%, group C: 23.9%). CONCLUSIONS: Endometriosis affects oocyte number but not embryo quality or pregnancy outcome.")
7
KİSTEKTOMİNİN OVER REZERVİNE ETKİSİ ??

8
IVF-ICSI outcome in women operated on for bilateral endometriomas. Somigliana E,et al. Hum Reprod. 2008 68 cases (bilat. cystectomy)- 136 controls the number of follicles (P = 0.006), oocytes retrieved (P = 0.024) and embryos obtained (P = 0.024) were significantly lower. The clinical pregnancy rate per started cycle in cases and controls was 7% and 19% (P = 0.037) CONCLUSIONS: IVF outcome is significantly impaired in women operated on for bilateral ovarian endometriomas.
- 136 controls the number of follicles (P = 0.006), oocytes retrieved (P = 0.024) and embryos obtained (P = 0.024) were significantly lower. The clinical pregnancy rate per started cycle in cases and controls was 7% and 19% (P = 0.037) CONCLUSIONS: IVF outcome is significantly impaired in women operated on for bilateral ovarian endometriomas..")
10
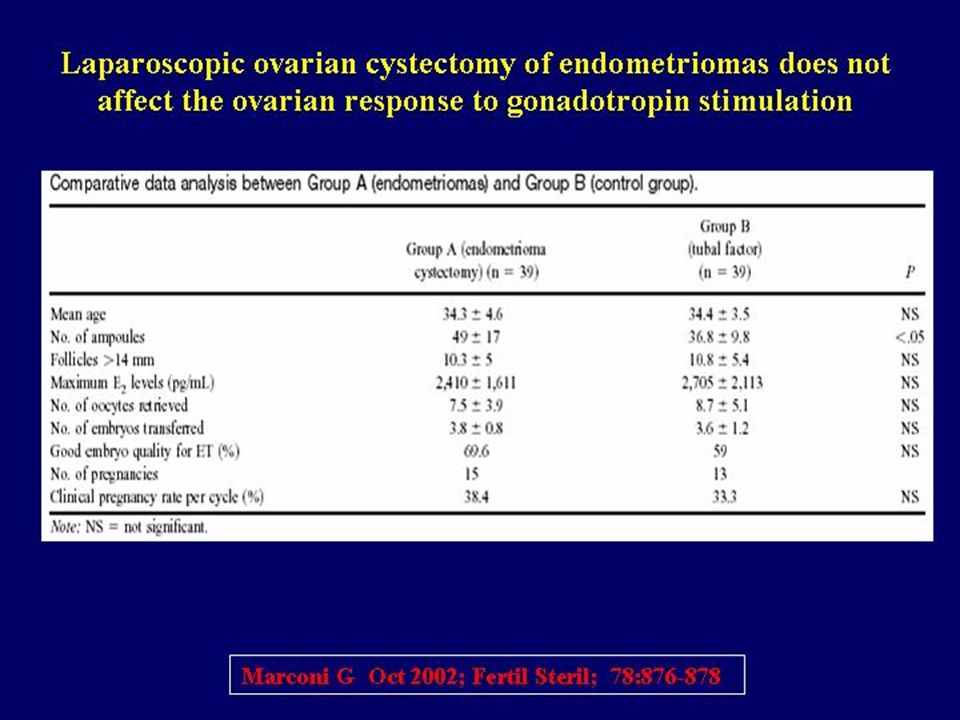
Studies evaluating response to ovarian stimulation in patients previously operated for endometriomas (EM) Number of casesOocytes retrievedEmbryos obtainedPregnancy rate Author Surgical technique olgu oositembryogebelik EMCtrEMCtrEMCtrEM (%)Ctr (%) Al-Azemi et al. (2000) * Not reported40806.9 ± 0.77.1 ± 0.5NA 15 Canis et al. (2001) Cyst enucleation 41599.4 ± 6.210.9 ± 6.5 4.7 ± 3.6 5.8 ± 4.9 3630 Donnez et al. (2001) Laser vaporization 8528 9 10.6 ± 4.2 8.6 ± 6.34.4 ± 3.2 4.0 ± 3.6 3735 Marconi et al. (2002) Cyst enucleation 39367.5 ± 3.98.7 ± 5.13.8 ± 0.8 3.6 ± 1.2 3833 Geber et al. (2002) 374612.0 ± 5.9 NA 5356 Pabucco et al. (2004) Cyst enucleation 44467.2 ± 1.5NA 2530
 * Not reported ± ± 0.5NA 15 Canis et al. (2001) Cyst enucleation ± ± ± ± Donnez et al. (2001) Laser vaporization ± ± ± ± Marconi et al. (2002) Cyst enucleation ± ± ± ± Geber et al. (2002) ± 5.9 NA 5356 Pabucco et al. (2004) Cyst enucleation ± 1.5NA")
11
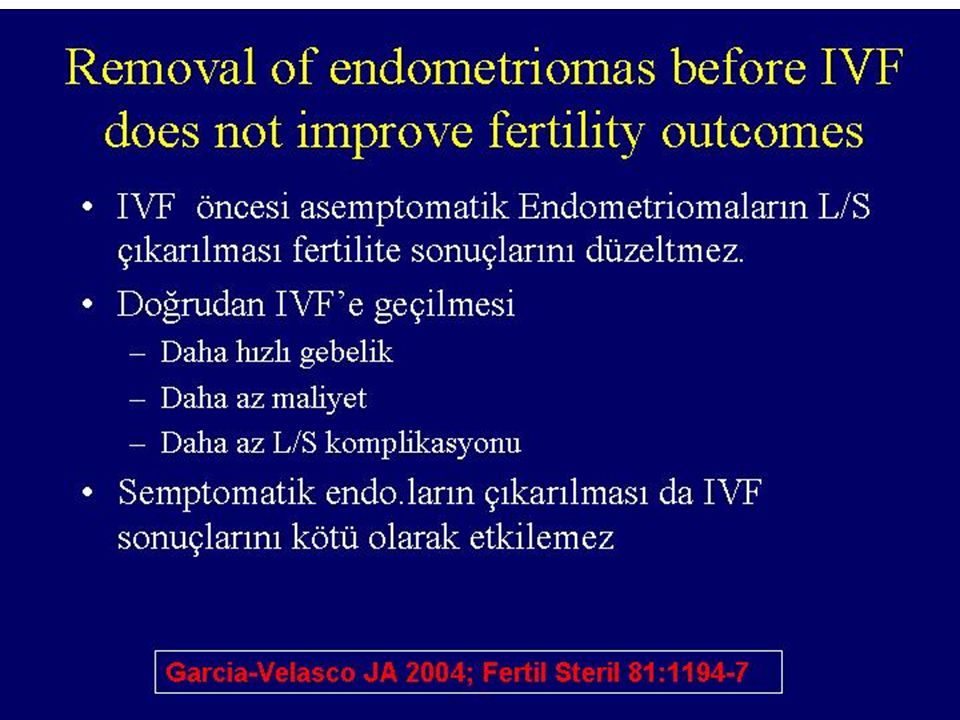
End.çıkarılmış 147 siklüs - %25.4 gebelik Çıkarılmamış 63 siklüs - %22.7 gebelik (p=0.776) (Fertil Steril 2004)
 (Fertil Steril 2004)")
13
Effect of endometrioma cystectomy on IVF outcome: a prospective randomized study. Demirol A, Reprod Biomed Online. 2006 prospectively randomized group I (49 patients) - ovarian surgery before ICSI group II (50 patients) -ICSI cycle directly Group 1- lower oocyte number There was no difference in terms of fertilization (86% in group I and 88% in group II), implantation (16.5% in group I and 18.5% in group II) pregnancy rates (34% in group I and 38% group II).
 - ovarian surgery before ICSI group II (50 patients) -ICSI cycle directly Group 1- lower oocyte number There was no difference in terms of fertilization (86% in group I and 88% in group II), implantation (16.5% in group I and 18.5% in group II) pregnancy rates (34% in group I and 38% group II)..")
14
Outcome of in vitro fertilization/intracytoplasmic sperm injection after laparoscopic cystectomy for endometriomas. Yaralı et al. Fertil Steril 2006 unilateral (n = 34) bilateral (n = 23) laparoscopic cystectomy control group (n= 99 ) tubal factor infertility The mean number of oocytes, metaphase II oocytes, and two-pronucleated oocytes were significantly lower in the bilateral cystectomy group fertilization rate, the mean number of embryos transferred, the mean number of grade 1 embryos transferred, the clinical PR/ET, implantation rate, were comparable among the three groups.
 bilateral (n = 23) laparoscopic cystectomy control group (n= 99 ) tubal factor infertility The mean number of oocytes, metaphase II oocytes, and two-pronucleated oocytes were significantly lower in the bilateral cystectomy group fertilization rate, the mean number of embryos transferred, the mean number of grade 1 embryos transferred, the clinical PR/ET, implantation rate, were comparable among the three groups..")
17
Laparoscopic resection or sonography-guided vaginal aspiration of endometriomas prior to ICSI- ET does not worsen treatment outcomes Tavmergen E, et al. Clin Exp Obstet Gynecol. 2007; resection group (Group I) 36 cycles ; aspiration (Group II) - 26 cycles control group (Group III) - 53 cycles - tubal factor Gonadotropin consumption was higher, peak estradiol level lower, the number of oocytes less in the laparascopic resection group (Group I) with respect to the control group. laparascopic endometrioma resection, transvaginal ultrasound-guided endometrioma cyst aspiration do not worsen the treatment outcome.
 36 cycles ; aspiration (Group II) - 26 cycles control group (Group III) - 53 cycles - tubal factor Gonadotropin consumption was higher, peak estradiol level lower, the number of oocytes less in the laparascopic resection group (Group I) with respect to the control group. laparascopic endometrioma resection, transvaginal ultrasound-guided endometrioma cyst aspiration do not worsen the treatment outcome..")
18
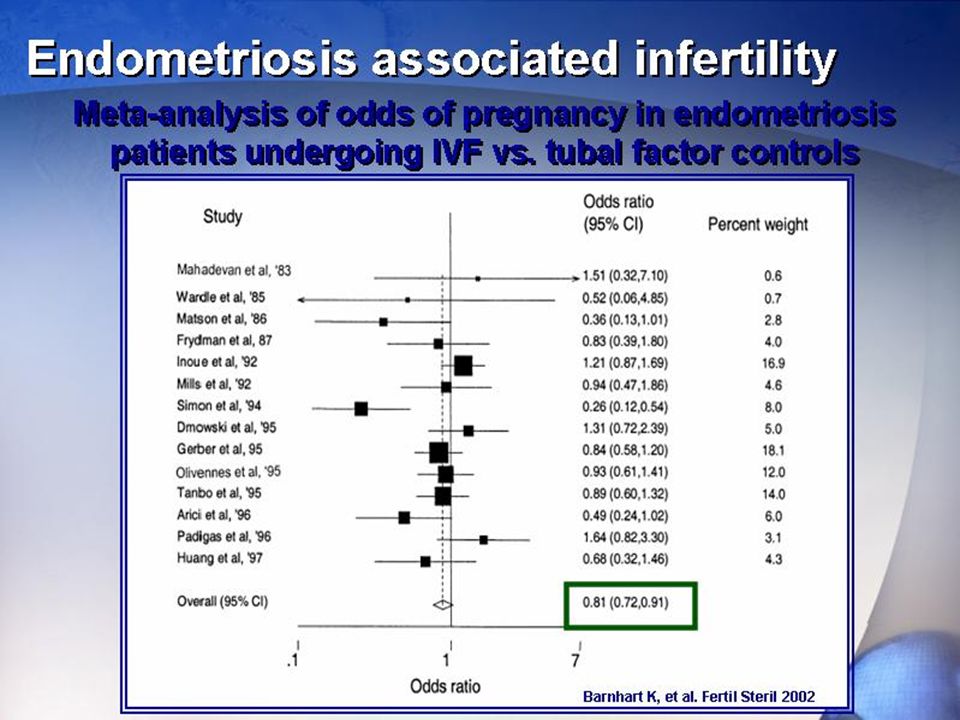
Impact of ovarian endometrioma on assisted reproduction outcomes. Gupta S. Reprod Biomed Online. 2006 Metaanalysis The odds for clinical pregnancy were not affected significantly in patients with ovarian endometrioma compared with controls, with an overall odds ratio of 1.07 from three studies [95% CI: (0.63-1.81), P = 0.79].
, P = 0.79]..")
19
The effect of surgical treatment for endometrioma on in vitro fertilization outcomes: a systematic review and meta-analysis. Tsoumpou I,.UK Fertil Steril 2008 A systematic review and meta-analysis three electronic databases - 1985 - 2007 20 eligible studies. Meta-analysis - five studies that compared surgery vs. no treatment of endometrioma. There was no significant difference in clinical pregnancy rate between the treated and the untreated groups. no significant difference -to controlled ovarian hyperstimulation with gonadotrophins

20
Should endometriomas be treated before IVF-ICSI cycles? Somigliana E, et al. Human Reprod Update 2006 The idea that surgery increases IVF pregnancy rates is not supported by the available evidence. However, the chance of conception is not the only issue that has to be considered.

21
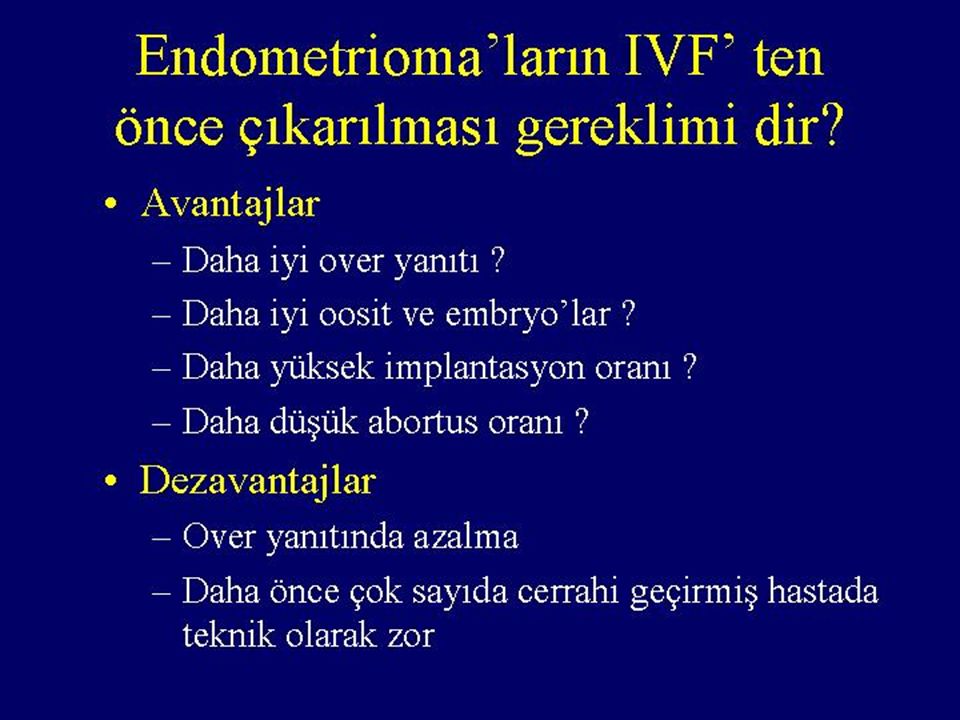
Copyright restrictions may apply. Somigliana, E. et al. Hum Reprod Update 2006 12:57-64; doi:10.1093/humupd/dmi035 Pros and cons of surgical treatment of endometriomas before IVF-ICSI cycles

22
Copyright restrictions may apply. Vercellini, P. et al. Hum. Reprod. 2008 0:den379v1-15; doi:10.1093/humrep/den379 Pregnancy rates observed after laparoscopic excision of endometriomas

23
Management of endometriomas in women requiring IVF: to touch or not to touch. Garcia-Velasco JA. Human Reprod 2008 proceeding directly to IVF to reduce time to pregnancy, to avoid potential surgical complications and to limit patient costs. Surgery should be envisaged only in presence of *large cysts, *pain symptoms which are refractory to medical treatments, *malignancy cannot reliably be ruled out

24
International guidelines on surgical treatment of endometriosis-associated infertility in asymptomatic women. Recommendation Recommended if endometrioma Online ISSN 1460-2350 - Print ISSN 0268-1161 Copyright ©Copyright © 2008 European Society of Human Reproduction and EmbryologyEuropean Society of Human Reproduction and Embryology Oxford Journals Oxford University Press Site Map Site Map Privacy Policy Privacy Policy Frequently Asked Questions Frequently Asked Questions Other Oxford University Press sites: ESHRE 2005ASRM 2006RCOG 2006 Minimal-mild endometriosis (stage I–II disease) Limited benefit: surgery recommendedSmall benefit: surgery recommendedDemonstrated benefit: surgery recommended Moderate–severe endometriosis (stage III-IV disease) Possible but unproven benefit: surgery recommended Possible benefit: surgery recommended Possible benefit: recommendation uncertain Post-operative adjuvant treatment No benefit: not recommended Surgery before IVF4 cmDoubtful benefit: no recommendation 4 cm Recurrent endometriosisNo recommendationSecond-line surgery not recommended No recommendation Return to article
 Limited benefit: surgery recommendedSmall benefit: surgery recommendedDemonstrated benefit: surgery recommended Moderate–severe endometriosis (stage III-IV disease) Possible but unproven benefit: surgery recommended Possible benefit: surgery recommended Possible benefit: recommendation uncertain Post-operative adjuvant treatment No benefit: not recommended Surgery before IVF4 cmDoubtful benefit: no recommendation 4 cm Recurrent endometriosisNo recommendationSecond-line surgery not recommended No recommendation Return to article.")
25
1- IVF öncesi cerrahi zorunlu değil 2-Semptom varsa opere edilebilir 3-Hastanın kaderini belirlemede ilk operasyon çok önemli Sonuç

Similar presentations


 Jahrom university of medical.>")

 Is It Safe? Mustafa Uğur Zekai Tahir Burak Women’s Health Education and Research Hospital, Ankara, Turkey.>")














 followed by ICSI in men with obstructive azoospermia University of Aberdeen Assisted reproductive unit D.Giannaris,>")