Download presentation
Presentation is loading. Please wait.

1
CUSP 4 MVP – VAP Improving Care for Mechanically Ventilated Patients
4 E’s for Early Mobility Pat Posa RN, BSN, MSA, FAAN System Performance Improvement Leader St. Joseph Mercy Hospital Ann Arbor MI CUSP 4 MVP – VAP Improving Care for Mechanically Ventilated Patients

2
Early Mobility Implementation – Importance of Nurse-led Mobilization
Goal for Early ICU Mobility Nursing led Physician driven Therapist supported and guided Activity prescription or activity/ADL prescription Armstrong Institute for Patient Safety and Quality

3
Importance of Nurse-led Mobilization
Most ICU nurses know why Early Mobility in the ICU is critically important Need to do root cause analysis of barriers and address each through education, training, policies, equipment, communication Barriers found upon Beaumont survey: Safety is a high concern Risk of injury to patient and self Accurately dosing mobility, choosing equipment, and communicating

4
Translating Evidence into Practice
(Johns Hopkins model)
")
5
Problems Associated with Critical Illness
When deconditioning and muscle weakness occur the course becomes complicated, the stay in the ICU is prolonged, and mortality increases Risk developing ICU-associated weakness due to polyneuropathy, myopathy, or a combination of both The cumulative effect of the complications are functional limitations that might or might not resolve.

6
Potential body/structure effects of critical illness
Nordon-Craft A, Moss M, Quan D, Schenkman M: Intensive care unit-acquired weakness: Implication for physical therapist management. Phys Ther. 2012; 92:

7
Long-Term Effects of Neuromuscular Disease
Probably one of the most landmark and well described studies illustrating the effects of neuromuscular weakness was completed by Margaret Herridge and published in the New England Journal of Medicine in Here they followed 109 ARDS survivors at three, six, and twelve months post-hospital discharge. Surprisingly, these patients had minimal lung pathology changes with normal lung volume and spirometric measurements by six months. Not one of the 109 survivors required the use of supplemental oxygen at 12 months despite the primary lung involvement at time of hospitalization. However, you can see here that a large percentage of patients continued to experience various functional deficits. At 12 months, forty-nine percent of patients were still unable to return to work most commonly due to persistent fatigue and weakness. You can also see that they commonly had much lower SF-36 scale scores in regards to physical functioning and physical role. It is important to note here that these were not patients nearing end of life as the median age of the population was 45 years. This is an age in which most are in the midst of income earning years. Herridge, MS et al. NEJM 348: 8, 2003

8
“The complications experienced by ICU
survivors include: Deterioration of strength, physical abilities, and psychological abilities. The persistence of symptoms such as reduced ability to perform activities of daily living, reduced capacity for ambulation, depression, posttraumatic stress syndrome, and anxiety contributes to an adverse effect on the individual’s quality of life and long-term survival. ‘Post–intensive care syndrome’ (PICS) is the preferred designation for this constellation of complications that endure well past the stay in the ICU.” Bemis-Dougherty AR, Smith JM. What follows survival of critical illness? Physical therapists’ management of patients with post–intensive care syndrome. Phys Ther. 2013;93:179–185.
 is the preferred designation for this constellation of complications that endure well past the stay in the ICU. Bemis-Dougherty AR, Smith JM. What follows survival of critical illness Physical therapists’ management of patients with post–intensive care syndrome. Phys Ther. 2013;93:179–185.")
9
Early Mobilization Protocol in Mechanically Ventilated Patients
Schweickert et al, Lancet 2009;373:

10
Schweickert et al, Lancet 2009;373:1874-82

11
Better outcomes Schweickert et al, Lancet 2009;373:

12
Summary Early PT and OT, paired with Wake Up and Breathe SAT/SBT protocol is… Safe and well-tolerated. Resulted in… 24% improvement (1.7-fold better) return to independent functional status at discharge (NNT=4) 50% reduction in the duration of delirium Schweickert et al, Lancet 2009;373:
 return to independent functional status at discharge (NNT=4) 50% reduction in the duration of delirium. Schweickert et al, Lancet 2009;373:")
13
Translating Evidence into Practice
(Johns Hopkins model) Walk your current process—ID the defects at each step
 Walk your current process—ID the defects at each step.")
14
What Are Your Barriers? Needham and Korpolu, Top Stroke Rehabil 2010;17(4):271–281
:271–281")
15
4E’s Early Mobility Frontline Staff Early Mobility Engage Adaptive Ask, how will Early Mobility make the world a better place? -Help staff understand preventable harm -Share stories about patients affected -Develop a business care -Include execute champion/physician leadership -Define evidence related to preventing VAEs (short and long term cognitive affects, and physical/psychological disabilities) -Share success stories, videos, or explore the IRN website during CUSP 4 MVP-VAP mtgs -Plan a site visit with experienced units/facilities -Create business case related to the impact of early mobility, including increased time off the ventilator, decreased hospital LOS and decreased ICU LOS -Share business case with executive champion/ physician leadership Educate Technical What do we need to mobilize critically ill patients? -Convert evidence into behaviors -Evaluate awareness and agreement -Discuss Post-Intensive Care Syndrome (PICS) -Review the literature -develop mobility criteria and progressive mobility protocol/guideline -Define your education plan (utilizing workshops, hands-on trainings, conferences, slides, presentations and interactive discussions via multiple modalities to cater to different learning styles) -Identify support through outreach to the leadership team Execute How will we implement early mobility at our hospital give local culture and resources? -Listen to resisters -Standardize care and create independent checks -Make it easy to do the right thing -Learn from mistakes -What is the process for mobilizing a patient? -Is there a policy on the unit? -Who should be involved? -Do we have all the equipment? -Discuss as part of interdisciplinary rounds/daily goals -Learn from defects Evaluate How will we know that our efforts to mobilize our patients made a difference? -Define measures -Regularly assess measures -Provide feedback to staff and celebrate success -Collect Early Mobility Daily Rounding measures and review at CUSP 4 MVP-VAP meetings -Use CECity to trend performance
 -Share success stories, videos, or explore the IRN website during CUSP 4 MVP-VAP mtgs. -Plan a site visit with experienced units/facilities. -Create business case related to the impact of early mobility, including increased time off the ventilator, decreased hospital LOS and decreased ICU LOS. -Share business case with executive champion/ physician leadership. Educate. Technical. What do we need to mobilize critically ill patients -Convert evidence into behaviors. -Evaluate awareness and agreement. -Discuss Post-Intensive Care Syndrome (PICS) -Review the literature. -develop mobility criteria and progressive mobility protocol/guideline. -Define your education plan (utilizing workshops, hands-on trainings, conferences, slides, presentations and interactive discussions via multiple modalities to cater to different learning styles) -Identify support through outreach to the leadership team. Execute. How will we implement early mobility at our hospital give local culture and resources -Listen to resisters. -Standardize care and create independent checks. -Make it easy to do the right thing. -Learn from mistakes. -What is the process for mobilizing a patient -Is there a policy on the unit -Who should be involved -Do we have all the equipment -Discuss as part of interdisciplinary rounds/daily goals. -Learn from defects. Evaluate. How will we know that our efforts to mobilize our patients made a difference -Define measures. -Regularly assess measures. -Provide feedback to staff and celebrate success. -Collect Early Mobility Daily Rounding measures and review at CUSP 4 MVP-VAP meetings. -Use CECity to trend performance.")
16
Educate / Engage at all Opportunities
CUSP meetings / Executive meetings Have therapy (PT/OT/Speech) as a member Group (Staff) meetings q6 weeks Board meetings (huddles) (pictures only please) Newsletter Bulletin Boards/Bathroom 1:1 (opportunity to talk with staff while collecting data)
 as a member. Group (Staff) meetings q6 weeks. Board meetings (huddles) (pictures only please) Newsletter. Bulletin Boards/Bathroom. 1:1 (opportunity to talk with staff while collecting data)")
17
Engage All Staff Sitters/Observers
Clinical Technicians/ Nursing Assistants Ambulate Turn ROM Document Ancillary Personnel Communication tools

18
Engage - Family Resources

19
Educate Turn evidence into behaviors
Define/Approve Mobilization readiness criteria Develop early/progressive mobility protocol/guideline Question: Our unit has protocol for early exercise and progressive mobility for ALL patients Question: Immobile patients on our unit receive passive range of motion regularly, if tolerated.

20
Medical Readiness Assessment
Armstrong Institute for Patient Safety and Quality

21
Readiness Assessment: Other Considerations
Recent Publication: Expert Consensus and Recommendations on safety criteria for active mobilization Critical Care (2014) 18:658 Patient factors Sedation level Breathing support for EM intervention Femoral Lines ECMO (Extracorporeal Membrane Oxygenation) Presence of lines, drains, catheters Other factors The right equipment Sufficient staffing / multidisciplinary focus
 18:658. Patient factors. Sedation level. Breathing support for EM intervention. Femoral Lines. ECMO (Extracorporeal Membrane Oxygenation) Presence of lines, drains, catheters. Other factors. The right equipment. Sufficient staffing / multidisciplinary focus.")
22
St. Joseph Mercy Hospital
Adapted from AACN

23
Early Mobility Protocols

24
Early Mobility Protocols

25
Execute make it easy to do the right thing
What is the process for mobilizing a patient? Is there a policy on the unit? Who should be involved? Do we have all the equipment? Discuss as part of interdisciplinary rounds/daily goals Added Mobility level to report sheet and nursing handoff Question: Mobility is addressed during daily rounds.

26
St. Joseph Mercy Hospital
Adapted from AACN

27
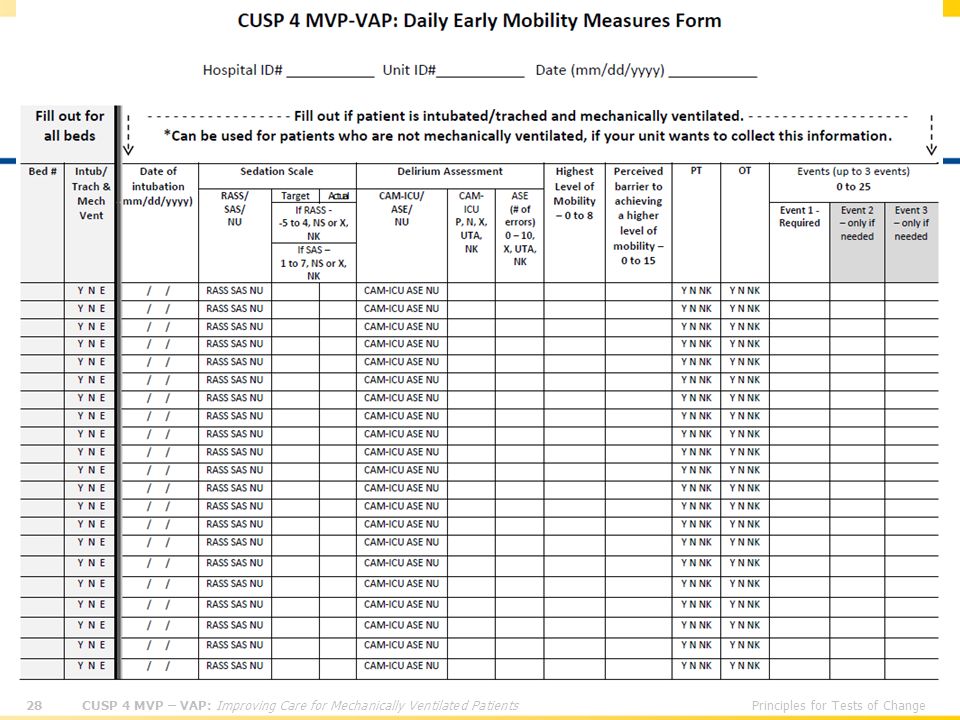
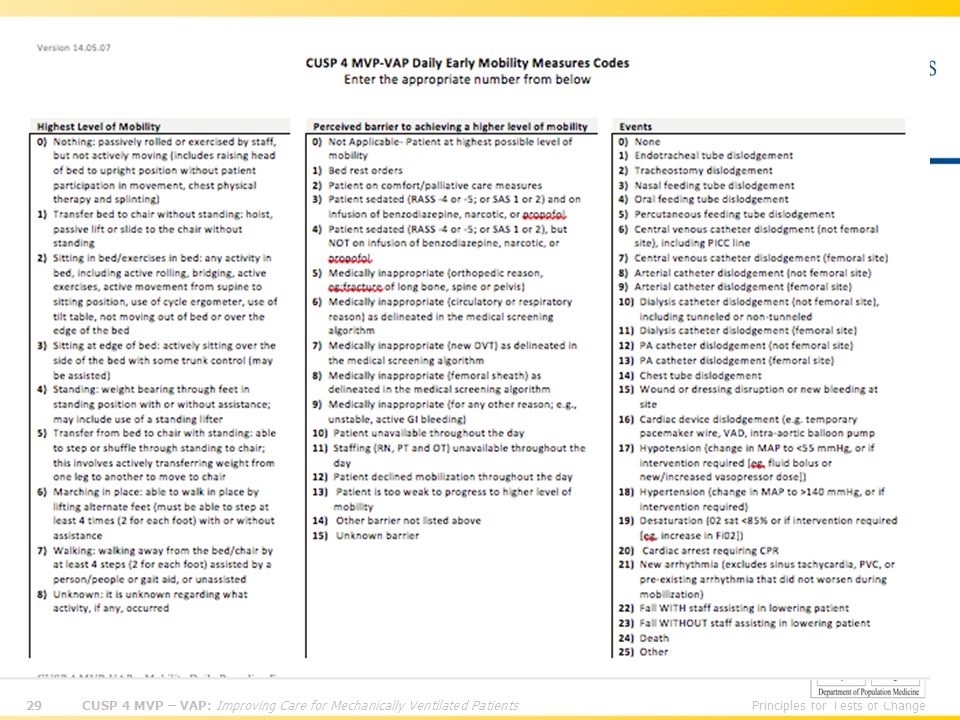
Evaluate Collect Early Mobility Daily Rounding measures and review at CUSP 4 MVP-VAP meetings We identified that we had no documentation standard related to mobility. We corrected that, which made our data collection easier. Use CECity to trend performance

Similar presentations







>")











