Download presentation
Presentation is loading. Please wait.

1
ACUTE AND POSTRAUMATIC STRESS DISORDERS, DISSOCIATIVE DISORDERS, AND SOMATOFORM DISORDERS CHAPTER SEVEN

2
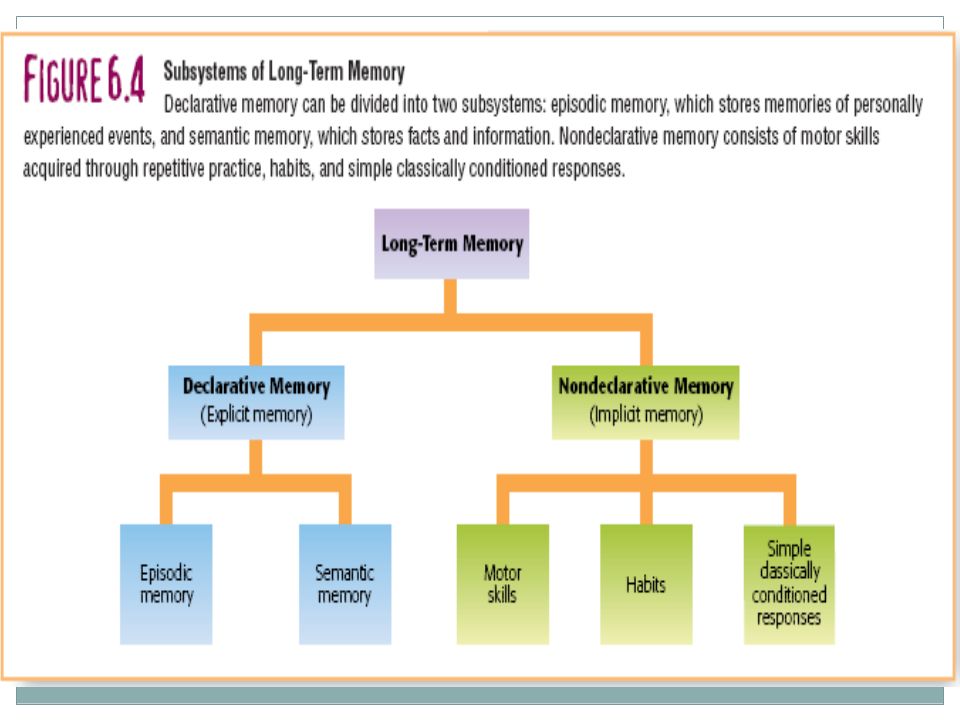
OVERVIEW Dissociation – the disruption of the normally integrated mental processes involved in memory, consciousness, identity, or perception.

3
ACUTE AND POSTRAUMATIC STRESS DISORDERS Traumatic stress An event that involves actual or threatened death or serious injury to self or others and creates intense feelings of fear, helplessness, or horror.

4
ACUTE AND POSTRAUMATIC STRESS DISORDERS Acute Stress Disorder (ASD) Occurs within four weeks after exposure to a traumatic stress and characterized by dissociative symptoms as well as: Reexperiencing, avoidance of reminders, and marked anxiety or arousal. Posttraumatic Stress Disorder (PTSD) Defined by symptoms of reexperiencing, avoidance, and arousal, but PTSD is either longer lasting (30+ days) or have a delayed onset.
 Defined by symptoms of reexperiencing, avoidance, and arousal, but PTSD is either longer lasting (30+ days) or have a delayed onset..")
5
ACUTE AND POSTRAUMATIC STRESS DISORDERS The defining symptoms of both acute and posttraumatic stress disorder include: (1) reexperiencing (2) avoidance (3) persistent arousal or anxiety Dissociative symptoms are common in the immediate aftermath of a trauma, but must be present for the diagnosis of ASD, but not PTSD.
 reexperiencing (2) avoidance (3) persistent arousal or anxiety Dissociative symptoms are common in the immediate aftermath of a trauma, but must be present for the diagnosis of ASD, but not PTSD.")
6
Reexperiencing Avoidance Repeated, distressing images or thoughts Intrusive flashbacks Horrifying dreams Attempts of avoid thoughts, feelings related to the event Avoid people, places, or activities that remind them of the event Numbing of responsiveness ACUTE AND POSTRAUMATIC STRESS DISORDERS

7
Arousal or anxiety Dissociative symptoms Predicts a worse prognosis Hypervigilance Restlessness, agitation, and irritability Exaggerated startle response Dazed and act “spaced out” Depersonalization Derealization Dissociative amnesia ACUTE AND POSTRAUMATIC STRESS DISORDERS

8
Comorbidity High for depression, other anxiety disorders, and substance abuse Anger – usually very prominent; Risk for suicide Frequency Prevalence of PTSD: 8% of people living in the United States (10% women, 5% of men) Rape and assault pose especially high risk for PTSD. Minorities are more likely experience PTSD. See Figure 7-1

9
ACUTE AND POSTRAUMATIC STRESS DISORDERS Biological Effects of Exposure to Trauma People with PTSD show alterations in the functioning, and perhaps structure, or the amygdala and hippocampus. The sympathetic nervous system is aroused and the fear response is sensitized in PTSD. Does trauma change the brain? Differences between people with and without PTSD are correlations.

10
ACUTE AND POSTRAUMATIC STRESS DISORDERS Psychological Factors in ASD and PTSD Two-factor theory Classical conditioning creates fear when the terror of trauma is paired with the cues associated with it. Operant conditioning maintains avoidance by reducing fear (negative reinforcement). Avoidance prevents the extinction of anxiety through exposure. The risk for PTSD depends on cognitive factors: preparedness, purpose and blame. Antidepressants such as SSRI’s are helpful Typical anxiety meds not effective
. Avoidance prevents the extinction of anxiety through exposure. The risk for PTSD depends on cognitive factors: preparedness, purpose and blame. Antidepressants such as SSRI’s are helpful Typical anxiety meds not effective.")
11
CBT for PTSD EMDR (Eye Movement Desensitization and Reprocessing) The most effective treatment for PTSD is reexposure to trauma. Prolonged exposure Imagery rehearsal therapy Cognitive restructuring Francine Sharpiro Includes rapid back- and-forth eye movements Prolonged exposure appears to be the “active ingredient” ACUTE AND POSTRAUMATIC STRESS DISORDERS

12
DISSOCIATIVE DISORDERS The symptoms of dissociative disorders are characterized by persistent, maladaptive disruption in the integration of memory, consciousness, or identity. Controversial and disbelieved by many.

14
Amnesia Retrograde Amnesia Anterograde Amnesia Is the amnesia biologically-based or psychogenic ? Organic amnesia usually involves personal and general information; also may involve anterograde amnesia. Psychogenic amnesia usually involves only personal information; also may involve retrograde amnesia.

15
Classifying Dissociative Disorders

17
Dissociative Fugue

18
Classifying Dissociative Disorders Dissociative Identity Disorder a.k.a. multiple personality disorder

19
Dissociative Identity Disorder “Host” personality – retains person’s name and identity and functions in the outside world. “Persecutory” personalities may be aggressive and hostile. “Protector” personalities may try to protect the host personality “Lost time” – loss of memory for events during which another personality was present.

20
Why should you doubt claims that dissociative identity disorder is common? 1. Most cases diagnosed by a handful of ardent advocates. 2. Frequency (DID in particular) increased rapidly after release of the very popular book and movie Sybil. 3. The number of personalities claimed to exist has grown rapidly, from a handful to 100 or more. 4. Rarely diagnosed outside of the USA and Canada; (only one case of DID has been reported in Great Britain in the last 25 years.)
 increased rapidly after release of the very popular book and movie Sybil. 3. The number of personalities claimed to exist has grown rapidly, from a handful to 100 or more. 4. Rarely diagnosed outside of the USA and Canada; (only one case of DID has been reported in Great Britain in the last 25 years.).")
21
DISSOCIATIVE DISORDERS Causes of Dissociative Disorders Psychological Factors in Dissociative Disorders Little controversy that dissociative amnesia and fugues can be precipitated by trauma. Trauma is “suspected” in DID, but much of the data is retrospective. The vast majority of trauma victims do not develop a dissociative disorder.

22
DISSOCIATIVE DISORDERS Causes of Dissociative Disorders Biological Factors Little to no evidence of biological and genetic factors. Social Factors Iatrogenesis – the manufacture of a disorder by its treatments. “cases” were created by the expectations of therapists?

23
Psychodynamic Perspectives Freud’s model Topographic model conscious preconscious unconscious

25
SOMATOFORM DISORDERS Symptoms of Somatoform Disorders Complaints about physical symptoms in the absence of medical evidence. The problem is very real in the mind, though not the body. Usual numerous, constantly evolving complaints such as chronic pain, upset stomach, dizziness. Worry about a deadly disease despite negative medical evidence.

26
SOMATOFORM DISORDERS Diagnosis of Somatoform Disorders Conversion Disorder Symptoms mimic neurological disorders Make no anatomic sense Implies that psychological conflicts are being converted into physical symptoms Somatization Disorder History of multiple somatic complaints in the absence of organic impairments. Eight symptoms, onset prior to age 30

27
SOMATOFORM DISORDERS Diagnosis of Somatoform Disorders Hypochondriasis Fear or belief that one is suffering from a physical illness. Much more serious than normal or fleeting worries and can lead to substantial impairment in life functioning. Pain Disorder Preoccupation with pain At risk for developing dependence on pain medication

28
Body dysmorphic disorder Malingering and factitious disorder Preoccupation with some imagined defect in appearance Repeated visits to the plastic surgeon Exceeds normal worry about imperfections Pretending to have a physical illness in order to achieve some external gain ($$$) Factitious disorder is motivated by a desire to assume a sick role SOMATOFORM DISORDERS
 Factitious disorder is motivated by a desire to assume a sick role SOMATOFORM DISORDERS")
29
Frequency of Somatoform Disorders Gender, SES and Culture More common among women (10 times) More common among lower SES Four times more common among African Americans and higher in Puerto Rico and Latin America Comorbidity Depression, anxiety, and antisocial personality disorder
 More common among lower SES Four times more common among African Americans and higher in Puerto Rico and Latin America Comorbidity Depression, anxiety, and antisocial personality disorder")
30
SOMATOFORM DISORDERS Causes of Somatoform Disorders Biological Factors Diagnosis by exclusion Perils of this approach – cases where some medical etiology can emerged later Psychological Factors Primary and secondary gain Cognitive tendencies: amplification, alexithymia (inability to express emotions in words)
")
31
FIGURE 7-6 Psychological Factors in Somatoform Disorders

32
SOMATOFORM DISORDERS Treatment of Somatoform Disorders Operant approaches to chronic pain Reward successful coping and adaptation Cognitive behavioral therapy Cognitive restructuring Antidepressants Patients are likely to refuse a referral to a mental health professional.

Similar presentations











 Delusions Hallucinations Disorganized.>")







 is a condition of persistent mental and emotional stress occurring as a result of injury or.>")
