Download presentation
Presentation is loading. Please wait.

1
Venous acess care Learning objectives –Learn about different cetral venous access devices (CVAD) –Catheter related complications of infectious and mechanical origin –Strategy to prevent problems and treatment of complications Summary Home parenteral nutrition (HPN) is a technical complex procedure that requries a central line. Although well trained in aseptic techniques patients will face infectious and other complications. This presentation deals with selecting the appropiate CCAD, prevention and management of complications. Refrences, links Slide from course McGee et al, N Engl J Med (PDF file) Slide from course Smith et al, JPEN (PDF file) Slide from course
 Slide from course Smith et al, JPEN (PDF file) Slide from course.")
2
Venous access care Considerations when choosing catheter Intravenous acess for HPN Insertion of catheters Catheter related complications –Infectious –Venous thrombosis –Catheter obstruction

3
Considerations when selecting a venous access device (VAD) The number of infusions to be given Type and length of therapy Available resources and expertise The age and diagnosis Specific vascular problems The VAD history Patients preference if long term treatment
 The number of infusions to be given Type and length of therapy Available resources and expertise The age and diagnosis Specific vascular problems The VAD history Patients preference if long term treatment")
4
Venous access devices Peripherally inserted central catheter (PICC) Central venous catheter (CVC) Hickman or Broviac, tunnelled catheter Port-a-cath
 Central venous catheter (CVC) Hickman or Broviac, tunnelled catheter Port-a-cath")
5
Peripherally inserted central catheter (PICC) Inserted in the cubital or upper arm region Intravenous nutrition and other infusion therapies No risk of trauma to neck structures, low risk of thrombosis For short term (3-4 weeks) use only Mostly for in patients Horattas MC et al. 2004; 10:2419-22

6
Tunnelled catheter A central catheter inserted in the subclavian or femoral vein with the tip in the vena cava or right atrium The distal part of the catheter is tunnelled in subcutaneous tissue Exit of tunnel with a position visible for the patient allowing self care

7
Broviac catheter for parenteral nutrition

8
Broviac or Hickman catheter Commonly used for HPN Different types with more lumens Blood draws should be avoided (infection) Covered by transparent dressing Patient may need help for dressing change Body image Shower and bathing possible
 Covered by transparent dressing Patient may need help for dressing change Body image Shower and bathing possible")
9
Broviac catheter

10
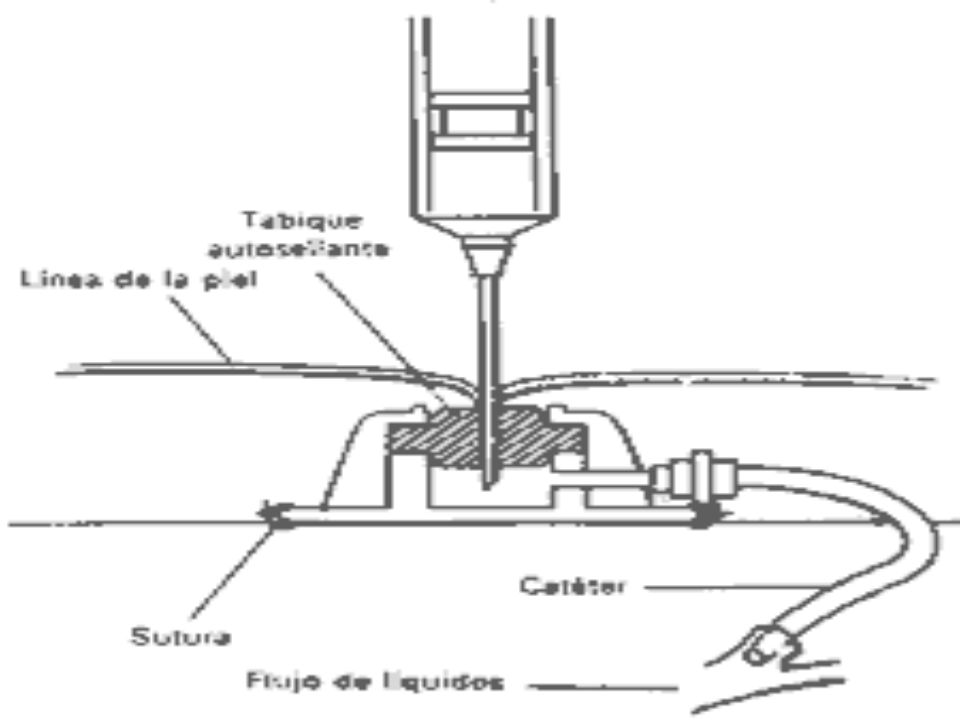
Port-a-Cath A stainless steel chamber with a membrane implanted in a subcutaneous pocket in the chest wall Accessed with a needle Not visible, body image If infected – remove – antibiotics will not clear the infection* *Kuizon, D et al. Arch Intern Med 2001; 161:406-10

13
Prevention of complications Recognize difficult catheter insertion –Previous failed attempts –Scaring, skeletal deformity Experience –Insertion of >50 catheters reduces complication risk significantly Ultrasound –For jugular access, lower rates of complications –For subclavian, no difference McGee D, Gould MK. N Engl J Med 2003; 348:1123-33

14
Insertion of catheter at the subclavian site: Lower risk of infection compared to internal jugular or femoral catherisation Lower risk of catheter related thrombosis compared to femoral or jugular insertion The rates of serious complications are similar for femoral and subclavian vein access Merrer J, De Jonghe B, Golliot F et al. JAMA. 2001; 286:700-7

15
Position of the distal tip Review of 141 cases of CVAD –Catheter tip location only factor predictive for malfunction (x-ray or fluoroscopy) –Significant increase in malfunction if tip more superior than 4 cm from junction of atrium and caval vein –Malfunction minimized in cases where tip in right atrium Petersen J, Delaney JH, Brakstad MT et al. Am J Surg. 1999;178:38-41

16
Catheter related complications Infectious –General measures –Impregnated catheters –Use of dressing –Patient support and education –ESPEN HAN survey on sepsis –Treatment

17
General measures Use of sterile barrier precautions reduces the rate of infections Disinfect catheter hubs – common site of contamination Remove catheters when no longer needed Routine changes of catheters do not reduce infectious complications McGee D, Gould MK. N Engl J Med 2003; 348:1123-33

18
Impregnated catheters The use of catheter impregnated with anti-microbial agents: Reduces the risk of catheter related bloodstream infections May lower cost of treatment Short term effect and probably not relevant to HPN population Raad I, Darouiche R, Dupuis J, et al Ann Intern Med. 1997; 127:267-74.

19
Central venous catheter dressings Different types of dressings available 25 studies, controlled/uncontrolled 15 studies included in meta-analysis –Comparison of gauze with dressings –Comparison of different dressings Conclusion –No difference in infectious complications rate between any dressing type –Small patient samples – lack of power Gillies D, O’Riordan E, et al, J Adv Nurs. 2003;44:623-32

20
Patient support and education Patient affiliation to ongoing HPN education interactive video-based for 18 months (randomised controlled), 39 patients –Significantly fewer hospitalisations for line infection at 6 and 18 months –Better quality of life score –Lower rate of depression –Patients better at defined problem solving Smith CE, Curtas S et al, JPEN 2003; 27:137-145
, 39 patients –Significantly fewer hospitalisations for line infection at 6 and 18 months –Better quality of life score –Lower rate of depression –Patients better at defined problem solving Smith CE, Curtas S et al, JPEN 2003; 27:")
21
ESPEN-HAN survey sepsis 2002 12 centres, 447 patients, a total of 110869 catheter days About 25 % had problems, about 50 % of infectious origin and removal of catheter in half the cases Risk factors port-a-cath and daily use of catheter Bozzetti F, Mariani L, Bertinet DB et al. Clin Nutr. 2002; 21:475-85.

22
Catheter associated infection Colonisation –The presence of organisms in the catheter by culture Blood stream infection –Culture of the same organism in the catheter and blood stream and no other source of infection Exit site infection –Erythema and tenderness or purulence within 2 cm of the exit site

23
Suspected catheter related infection Blood cultures drawn from catheter and a peripheral site Culture from the hub Inspect catheter site for signs of infection – if erythema or pus consider removal Antibiotic treatment

24
Catheter related infection Antibiotic treatment according to microbiology *Catheter lock ? –Antibiotics to disinfect –Alcohol to dissolve organic debris –Urokinase to lyse fresh thrombus Save catheter when possible Remove immediately in case of septic shock * Case reports and small studies in support

25
Catheter related complications Thrombosis Mechanical

26
Catheter related venous thrombosis In 33 % of ICU patients by Doppler Risk higher with insertion at femoral > jugular > subclavian site If diagnosed in the HPN patient population –Removal of catheter, anticoagulant treatment –Thrombolytic medication ? –Loss of venous access –Probably under diagnosed –Clinical studies warranted

27
Catheter occlusion Common problem Random and unpredictable event Can be associated with: –Catheter life span –Type of catheter –Handling –Blood flushing back –Composition of parenteral nutrition

28
Catheter occlusion Management –Use of thrombolytic agents –Flush with saline –Flush with alcohol –Flush with acid –Mechanical rinsing with brush References, available, mostly case reports

29
Summary slide Chose access for CVAD carefully General use aseptic techniques are of paramount importance Support patients educationally to minimise line related complications In case of complications use protocols to treat patients Support clinical studies in this field

Similar presentations













 Management of Central Venous Access Devices 4. PERIPHERALLY.>")

 involves injecting a medication directly into the blood via venous access devices IV products must be sterile.>")




