Download presentation
Presentation is loading. Please wait.

1
Camille Okelberry Danielle Quinton Toni Brown
Pancreatitis Camille Okelberry Danielle Quinton Toni Brown

2
Physiology

3
Physiology of Pancreas
Endocrine function Insulin Glucagon Somatostatin

4
Physiology of the Pancreas
Made up of a series of microscopic ducts that drain into larger ducts These eventually drain into the main pancreatic duct which joins with the common bile duct and drains into the duodenum. There is also a smaller duct that drains directly into the duodenum from the pancreas

5
Source: SMART Imagebase
(
")
6
Physiology of the Pancreas

7
Physiology of the Pancreas
Pancreatic Juice About 1500ml/d Hypertonic Bicarbonate secreted by the duct cells via secretin Bicarb levels depend on the rate of flow from the pancreas If flow is slow, bicarb is exchanged for Chloride ions If flow is fast, bicarb does not have time to exchange

8
Physiology of the Pancreas
Pancreatic enzymes

9
Physiology of the Pancreas
Pancreatic enzymes Proteolytic Trypsin, chymotrypsin, carboxypeptidase Stored in acinar cells Secreted in the inactive form and activated in the small intestine Avoiding self-digestion Chymotrypsin activated by trypsin Hydrolyze peptide bonds If these are activated before reaching the duodenum PANCREATITIS

10
Physiology of the Pancreas
Pancreatic Enzymes Pancreatic amylase Secreted in active form CHO digestion begins w/ salivary amylase Can digests cooked and uncooked starch Lipolytic enzymes Digests fatty chyme Secreted in inactive form Pancreatic lipase

11
Physiology of the Pancreas
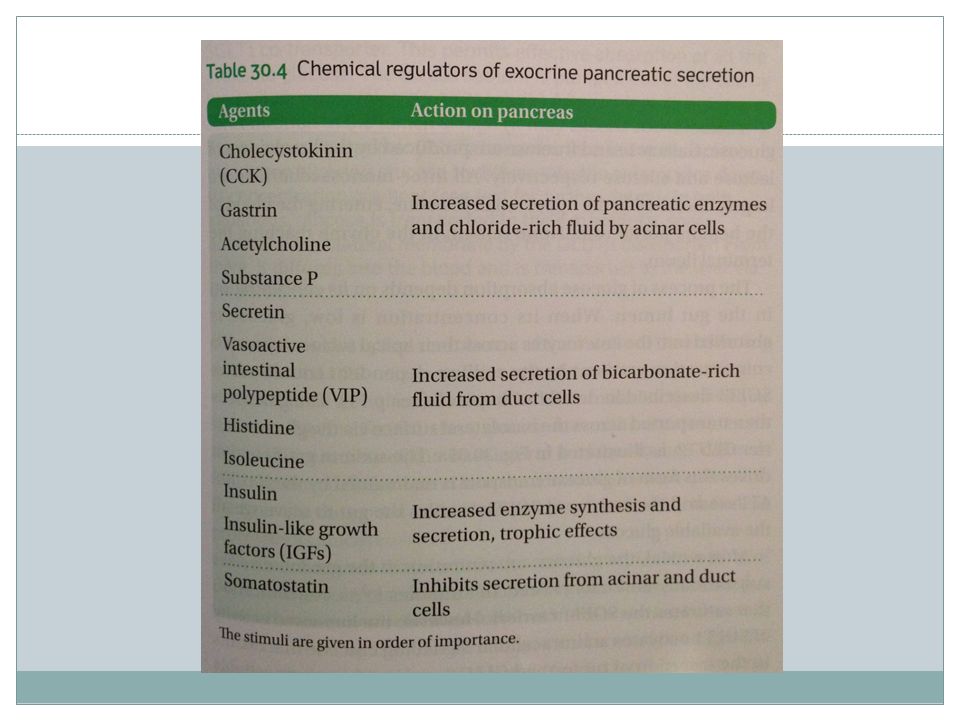
Regulation of Pancreatic secretion Vagus nerve Hormones Cephalic Phase Smooth muscle cells of the ducts and blood vessels innervated by parasympathetic vagal efferent fibers Gastric Phase Gastrin: secreted in response to distension of stomach Stomach distension also causes release of pancreatic enzymes Intestinal Phase Responsible for most of the secretion Response to hormones secreted by upper intestinal mucosa Secretin, CCK Secretin: response to low pH and stimulate the secretion of bicarbonate from the duct cells. Increases secretion of pancreatic enyzmes. CCK: when mucosal surface is bathed in monoglycerides, FA, peptides, and AA.

13
Acute Pancreatitis

14
Pancreatitis Acute Chronic Mild Severe

15
Acute Pancreatitis Sudden inflammation of the pancreas
Can sometimes result in a systemic inflammatory response that can damage other organs or systems Most people require a short hospital stay 1 in 10 may require longer treatment

16
Incidence and Prevalence
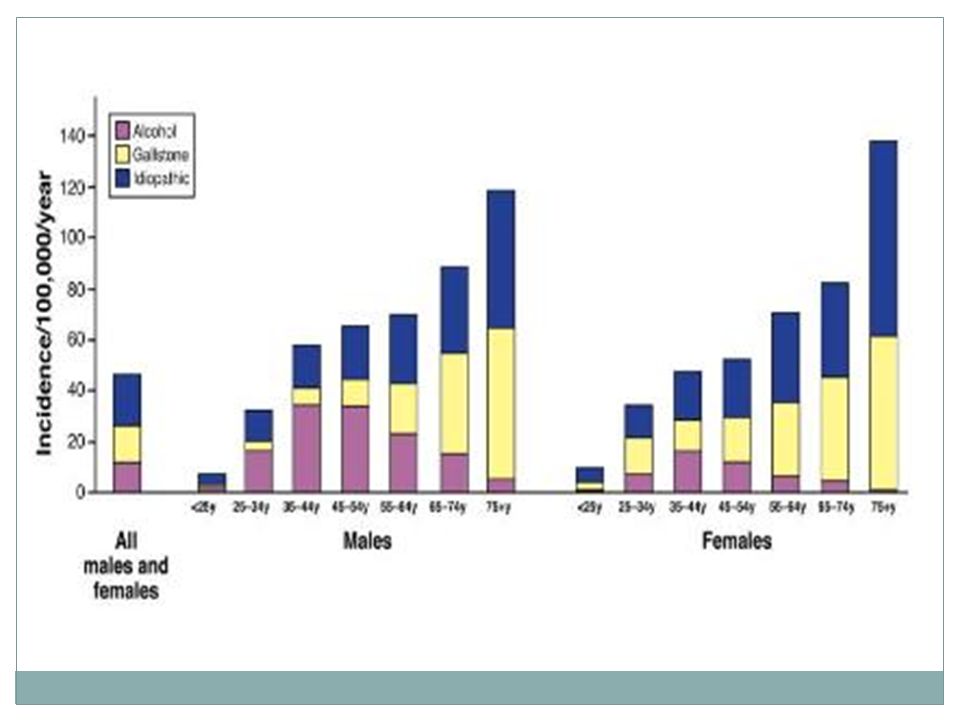
The incidence of acute pancreatitis that is gallstone related is 15/100,000 Non-gallstone related is 25/100,000 300,000 hospital admissions/year for treatment of acute pancreatitis African Americans are 2 to 3 times more likely to develop pancreatitis than Caucasians

17
Etiology Alcohol Gallstones Hypertriglyceridemia Hypercalcemia
Certain medications Genetics/gene mutations

19
Alcohol Oxidation of ethanol to acetaldehyde activates pancreatic stellate cells without any pre-activation which leads to oxidative stress and eventually fibrosis

20
Gallstones

21
Hypertriglyceridemia
Triglycerides are carried by chylomicrons in the blood If there is an excess amount of triglycerides, there will be an excess amount of chylomicrons When the chylomicrons are larger than 900 mg/dL they have the ability to block capillaries in the pancreas This can lead to ischemia, alteration of acinar cells and increased lipase release Increased lipolysis and free fatty acids in the blood can lead to inflammation, free radicals and necrosis

22
Hypercalcemia Increased calcium over a prolonged period of time results in destruction of defense mechanisms This leads to the premature activation of trypsinogen and acinar cell necrosis (pancreatitis)
")
23
Gene mutations One of the mutations occurs in the cystic fibrosis transmembrane conductance regulator (CFTR) The mutation of this regulator results in the retention of zymogens in the duct These zymogens become active and begin digesting the pancreas, leading to acute pancreatitis

24
Medications Opiates Tetracycline Steroids Furosemide Acetaminophen
Erythromycin Rifampin Estrogen preparations Drug-induced pancreatitis: an update. Trivedi CD1, Pitchumoni CS.

25
Pathophysiology Sudden intense abdominal attacks
If mild, the patient can withhold feeding for a couple of days until pain subsides To prevent further attacks, treat the underlying cause (gallstones, alcohol, hypertriglyceridemia, etc.) If pain comes back after a few days, it may be severe pancreatitis and require longer hospitalization
 If pain comes back after a few days, it may be severe pancreatitis and require longer hospitalization.")
26
Signs and Symptoms Sudden Attacks
Intense epigastric pain radiating to the back N/V Fever Symptoms may be aggravated after eating

27
Diagnosis Blood amylase and lipase levels CT/MRI test Ultrasound
Ranson’s Criteria Amylase and lipase levels are 3 times the normal amount in acute pancreatitis

28
Diagnosis – Amylase and Lipase
Evaluating amylase and lipase levels is one of the most widely used diagnostic tests to determine pancreatitis Amylase and lipase levels will be 3 times higher in a patient with pancreatitis compared to normal - Lipase levels rise later and stay elevated for 5 to 7 days therefore are more useful in the late diagnosis of acute pancreatitis Pagana

29
Diagnosis - CT Scan

30
Ranson’s Criteria The criteria that classifies the severity of pancreatitis includes: Age >55 White blood cell >16,000 m3 Blood glucose levels >200 mg Lactic dehydrogenase >350 units/L Aspartate transaminase >250 units/L

31
Ranson’s Criteria During the first 48 hours:
Hematocrit decrease of >10 mg/dL Blood urea nitrogen increase of >5 mg/dL Arterial PO2 <60 mm Hg Base deficit >4 mEq/L Fluid sequestration >6000 mL Serum calcium level <8 mg/mL

32
Treatment Medication Surgery (for severe acute pancreatitis)
")
33
Treatment - Medical therapies
H2 receptor antagonist Proton pump inhibitors Somatostatin Opiods (morphine) H2 receptor antagonists stop the release of acid from parietal cells in the stomach One study showed there was no difference between cimetidine (H2 receptor antagonist) and a placebo considering duration of pain. Somatostatin inhibits secretion of insulin, glucagon, gastrin
 H2 receptor antagonists stop the release of acid from parietal cells in the stomach. One study showed there was no difference between cimetidine (H2 receptor antagonist) and a placebo considering duration of pain. Somatostatin inhibits secretion of insulin, glucagon, gastrin.")
34
H2 receptor antagonists and Proton Pump Inhibitors

35
Treatment - Surgery Remove the gallbladder
Remove inflamed parts of the pancreas Remove necrotic tissue and pseudocysts ERCP

36
Treatment - ERCP Endoscopic Retrograde Cholangiopancreatography
Special technique designed to treat complications of pancreatitis including gallstones, narrowing of the pancreatic or bile duct, leaks and pseudocysts An endoscope is inserted into the intestine where the problem is identified and fixed 4:08 to 6:40

37
MNT Mild Acute Pancreatitis
“Pancreatic rest” NPO – oral feeding is withheld Fluids given intravenously In less severe attacks, a clear liquid diet low in fat may be given for a few days until patient can tolerate more easily digested foods. Six, smaller meals/day Animal and human studies show that exocrine function is decreased after pancreatitis. – it shouldn’t matter whether they are fed through NG or NJ. NJ is more expensive and requires a specialist to insert. A study compared NPO versus NGT. NGT was well tolerated in patients with mild to moderate AP. Compared to NPO, it reduces the intensity and duration of abdominal pain, need for opiates, and risk of oral food intolerance but not overall hospital stay. Early nasogastric tube feeding versus nil per os in mild to moderate acute pancreatitis: A randomized controlled trial Maxim S. Petrova, , , Kerry McIlroyb, Lorraine Graysona, Anthony R.J. Phillipsa, John A. Windsora

38
MNT Severe Acute Pancreatitis
Severe acute pancreatitis results in a hypermetabolic, catabolic state with demands similar to sepsis Nutrition therapy should include adequate protein If oral nutrition can’t be initiated in 5 to 7 days, start tube feeding Enteral nutrition is preferred method because it stimulates GIT and reduces risk of bacterial translocation Enteral nutrition given within 48 hours reduces MODS, mortality and pancreatic complications Standard formula is used first and if not tolerated, switched to elemental NG tube feeding has been found to be efficacious in AP.

39
NG vs. NJ – Which is better?
NG tube will stimulate pancreatic secretion while bypassing the duodenum with an NJ tube can limit pancreatic secretion

40
Prognosis The higher the prognosis score, the poorer the outcome
Patients with mild acute pancreatitis have a low mortality rate while those with severe acute pancreatitis are more likely to have complications and therefore have a higher death rate Mortality for mild acute pancreatitis is <1% while the death rate for severe acute pancreatitis can be 10% to 30 % depending on sterile versus infected necrosis

41
Alcohol

42
Prevalence

43
Prevalence Prevalence of Drinking: (In 2012)
87.6 percent of people ages 18 or older reported that they drank alcohol at some point in their lifetime 71 percent reported that they drank in the past year 56.3 percent reported that they drank in the past month Prevalence of Binge Drinking and Heavy Drinking: (In 2012) 24.6 percent of people ages 18 or older reported that they engaged in binge drinking in the past month 7.1 percent reported that they engaged in heavy drinking in the past month
 24.6 percent of people ages 18 or older reported that they engaged in binge drinking in the past month. 7.1 percent reported that they engaged in heavy drinking in the past month.")
44
Drug Time Period 8th Graders 10th Graders 12th Graders
Monitoring the Future Study: Trends in Prevalence of Alcohol for 8th Graders, 10th Graders, and 12th Graders; 2014 (in percent)* Drug Time Period 8th Graders 10th Graders 12th Graders Alcohol Lifetime 26.80 [49.30] [66.00] Past Year 20.80 [44.00] 60.20 Past Month 9.00 [23.50] 37.40 National Survey on Drug Use and Health: Trends in Prevalence of Alcohol for Ages 12 or Older, Ages 12 to 17, Ages 18 to 25, and Ages 26 or Older; 2013 (in percent)* Drug Time Period Ages 12 or Older Ages 12 to 17 Ages 18 to 25 Ages 26 or Older Alcohol Lifetime [81.50] 30.80 83.80 87.30 Past Year 66.30 [24.60] 76.80 69.60 Past Month 52.20 [11.60] 59.60 55.90
* Drug. Time Period. 8th Graders. 10th Graders. 12th Graders. Alcohol. Lifetime [49.30] [66.00] Past Year [44.00] Past Month [23.50] National Survey on Drug Use and Health: Trends in Prevalence of Alcohol for Ages 12 or Older, Ages 12 to 17, Ages 18 to 25, and Ages 26 or Older; 2013 (in percent)* Drug. Time Period. Ages 12 or Older. Ages 12 to 17. Ages 18 to 25. Ages 26 or Older. Alcohol. Lifetime. [81.50] Past Year [24.60] Past Month [11.60]")
45
Prevalence: Young Adult/Teenagers
Prevalence of Drinking: 2 out of 5 15-year-olds report that they have had at least 1 drink in their lives In 2012, about 9.3 million people ages 12–20 (24.3 percent of this age group) reported drinking alcohol in the past month (24.7 percent of males and 24 percent of females) Prevalence of Binge Drinking: Approximately 5.9 million people (about 15 percent) ages 12–20 were binge drinkers (16.5 percent of males and 14 percent of females) Prevalence of Heavy Drinking: Approximately 1.7 million people (about 4.3 percent) ages 12–20 were heavy drinkers (5.2 percent of males and 3.4 percent of females).
 reported drinking alcohol in the past month (24.7 percent of males and 24 percent of females) Prevalence of Binge Drinking: Approximately 5.9 million people (about 15 percent) ages 12–20 were binge drinkers (16.5 percent of males and 14 percent of females) Prevalence of Heavy Drinking: Approximately 1.7 million people (about 4.3 percent) ages 12–20 were heavy drinkers (5.2 percent of males and 3.4 percent of females).")
46
What is a drink? A standard drink equals 0.6 ounces of pure ethanol
12 ounces of beer 8 ounces of malt liquor 5 ounces of wine or 1.5 ounces (a "shot") of 80-proof distilled spirits or liquor (e.g., gin, rum, vodka, or whiskey)
 of 80-proof distilled spirits or liquor (e.g., gin, rum, vodka, or whiskey)")
47
Drinking Terms Moderate Drinking: Up to 1 drink per day for women and up to 2 drinks per day for men Binge Drinking: Drinking 5 or more alcoholic drinks on the same occasion on at least 1 day in the past 30 days Heavy Drinking: Drinking 5 or more drinks on the same occasion on each of 5 or more days in the past 30 days Alcoholism: Alcoholism or alcohol dependence is a diagnosable disease characterized by a strong craving for alcohol, and/or continued use despite harm or personal injury Alcohol Abuse: Alcohol abuse, which can lead to alcoholism, is a pattern of drinking that results in harm to one's health, interpersonal relationships, or ability to work

48
Metabolism CO2 and H2O Highly toxic and known carcinogen
The process of breaking alcohol down generates toxins even more harmful than alcohol itself. These byproducts damage liver cells, promote inflammation, and weaken the body’s natural defenses. Eventually, these problems can disrupt the body’s metabolism and impair the function of other organs. CO2 and H2O

49
Effects on the Body Increases risk of cancers of the mouth, esophagus, throat, liver, breast Interferes with the brain’s communication pathways, can change mood and behavior Cardiomyopathy (stretching and drooping of heart muscle), arrhythmias (irregular heart beat), stroke, high blood pressure Causes the pancreas to produce toxic substances that can eventually lead to pancreatitis Steatosis (fatty liver), alcoholic hepatitis, fibrosis, cirrhosis
, arrhythmias (irregular heart beat), stroke, high blood pressure Causes the pancreas to produce toxic substances that can eventually lead to pancreatitis. Steatosis (fatty liver), alcoholic hepatitis, fibrosis, cirrhosis.")
50
Alcohol-related Mortality
Nearly 88,000 people (approximately 62,000 men and 26,000 women) die from alcohol related causes annually, making it the third leading preventable cause of death in the United States In 2012, alcohol-impaired-driving fatalities accounted for 10,322 deaths (31 percent of overall driving fatalities) In 2012, 3.3 million deaths, or 5.9 percent of all global deaths (7.6 percent for men and 4 percent for women), were attributable to alcohol consumption Alcohol contributes to over 200 diseases and injury-related health conditions, most notably alcohol dependence, liver cirrhosis, cancers, and injuries Alcohol misuse is the fifth leading risk factor for premature death and disability; among people between the ages of 15 and 49, it is the first worldwide
 die from alcohol related causes annually, making it the third leading preventable cause of death in the United States In 2012, alcohol-impaired-driving fatalities accounted for 10,322 deaths (31 percent of overall driving fatalities) In 2012, 3.3 million deaths, or 5.9 percent of all global deaths (7.6 percent for men and 4 percent for women), were attributable to alcohol consumption Alcohol contributes to over 200 diseases and injury-related health conditions, most notably alcohol dependence, liver cirrhosis, cancers, and injuries Alcohol misuse is the fifth leading risk factor for premature death and disability; among people between the ages of 15 and 49, it is the first worldwide.")
51
Health Benefits Decreased risk for heart disease and mortality due to heart disease Decreased risk of ischemic stroke (in which the arteries to the brain become narrowed or blocked, resulting in reduced blood flow), and Decreased risk of diabetes “In most Western countries where chronic diseases such as coronary heart disease (CHD), cancer, stroke, and diabetes are the primary causes of death, results from large epidemiological studies consistently show that alcohol reduces mortality, especially among middle-aged and older men and women—an association which is likely due to the protective effects of moderate alcohol consumption on CHD, diabetes, and ischemic stroke.” “It is estimated that 26,000 deaths were averted in 2005 because of reductions in heart disease, stroke, and diabetes from the benefits attributed to moderate alcohol consumption.” Alcohol may not benefit everyone who drinks moderately Pg 26
, and. Decreased risk of diabetes In most Western countries where chronic diseases such as coronary heart disease (CHD), cancer, stroke, and diabetes are the primary causes of death, results from large epidemiological studies consistently show that alcohol reduces mortality, especially among middle-aged and older men and women—an association which is likely due to the protective effects of moderate alcohol consumption on CHD, diabetes, and ischemic stroke. It is estimated that 26,000 deaths were averted in 2005 because of reductions in heart disease, stroke, and diabetes from the benefits attributed to moderate alcohol consumption. Alcohol may not benefit everyone who drinks moderately. ua=1 Pg 26.")
52
Chronic Pancreatitis

53
Chronic inflammation of the pancreas that leads to permanent damage (necrosis)
")
54
Usually develops in patients between the ages of 30 and 40
people in every 100,000 will develop pancreatitis in industrialized countries Usually develops in patients between the ages of 30 and 40 More prevalent among men than women Numbers in parenthesis indicate approximate yearly incident rates per 100,000 persons. Arrow indicates relationship between benign and malignant disease. Recurrent AP develops predominately in patients with non-gallstone related pancreatitis, although it can develop in patients with gallstone-related pancreatitis when cholecystectomy has been delayed or refused.

55
Incidence of CP

56
Physiology Inhibits secretions of hormones like GH, TSH, CCK, insulin
Released in response to ingestion; regulates food intake

57
Causes Heavy alcohol use Elevated triglycerides Autoimmune disorders
Genetic conditions (cystic fibrosis, hereditary pancreatitis) Blocked pancreatic duct or common bile duct Inherited pancreatitis (2 or more immediate family members with a history of pancreatitis)
 Blocked pancreatic duct or common bile duct. Inherited pancreatitis (2 or more immediate family members with a history of pancreatitis)")
58
Signs and Symptoms Nausea Vomiting Back pain Weight loss (late stages)
Diarrhea Oily or fatty stools (late stages)
")
59
Individuals with chronic pancreatitis frequently lose weight, even when their appetite and eating habits are normal

60
Diagnosis Blood tests are NOT helpful, but sometimes test for IgG4 to assess for autoimmune pancreatitis useful Transabdominal ultrasound Endoscopic ultrasound Magnetic resonance cholangiopancreatopgraphy (MRCP) Computerized Tomography (CT)
 Computerized Tomography (CT)")
61
Transabdominal Ultrasound
Sound waves are sent toward the pancreas via a handheld device that a technician glides over the abdomen The sound waves bounce off the pancreas, gallbladder, liver, and other organs, and their echoes generate electrical impulses that create an image (a sonogram) on a video monitor If gallstones are causing inflammation, the sound waves will bounce off of them, showing their location
 on a video monitor. If gallstones are causing inflammation, the sound waves will bounce off of them, showing their location.")
62
Endoscopic Ultrasound
Spray a solution to numb the patient’s throat Doctor inserts an endoscope down the throat, through the stomach, and into the small intestine They turn on an ultrasound attachment to the endoscope, which produces sound waves to create visual images of the pancreas and bile ducts

63
Magnetic Resonance Cholangiopancreatography (MRCP)
Patient is lightly sedated and lies in a cylinder-like tube Technician injects dye into the patient’s veins, which helps show the pancreas, gallbladder, and pancreatic and bile ducts

64
Computerized Tomography (CT)
Noninvasive radiograph (x-ray) that produces 3-dimensional images of parts of the body The patient lies on a table that slides into a donut-shaped machine The test can show gallstones and the extent of damage to the pancreas
 that produces 3-dimensional images of parts of the body. The patient lies on a table that slides into a donut-shaped machine. The test can show gallstones and the extent of damage to the pancreas.")
65
Pancreatic Stimulation Test
Injection of secretin to stimulate pancreas Used for cases where difficult to diagnose Expensive Invasive

66
Medical Treatment No cure for chronic pancreatitis
Treat symptoms, decrease pain Avoid triggers Pancreatic enzyme replacement (PERT) Antioxidants
 Antioxidants.")
67
Medical Treatment: Medications
WHO’s 3-step ladder: Begin with nonopioids (acetaminophen, ibuprofen, or both) If nonopioids do not relieve pain, mild opioids (like codeine) are given If mild opioids do not relieve pain, strong opioids (like morphine) are given
 If nonopioids do not relieve pain, mild opioids (like codeine) are given. If mild opioids do not relieve pain, strong opioids (like morphine) are given.")
68
Medical Treatment: Surgery
Lateral pancreaticojejunostomy (modified Puestow procedure): can lead to pain relief in up to 80% of patients Whipple Procedure Total pancreatectomy with islet auto-transplantation (TP-IAT): when pain remains incapacitating
: can lead to pain relief in up to 80% of patients. Whipple Procedure. Total pancreatectomy with islet auto-transplantation (TP-IAT): when pain remains incapacitating.")
69
MNT Avoid alcohol Quit smoking Avoid high-fat foods
Vitamins and minerals as needed

70
MNT cont. MAIN GOALS: 1) Provide optimal nutrition support and 2) decrease pain my minimizing stimulation of the exocrine pancreas Small frequent meals Low-fat Vegetable based oils Treat vitamin B12, A, D, E, K deficiencies Maintain acid-base balance (using antacids, H2-receptor antagonists, or proton pump inhibitors Insulin and nutrition therapy B12 def: pancreatic protease is necessary to cleave B12 from its carrier protein Acid-base:pancreatic bicarbonate secretions is frequently defective Manage blood glucose, but focus on control of symptoms rather than normoglycemia

71
Alternative Therapy Yoga Massage therapy Therapeutic Touch
Physical Exercise Meditation Laughter Acupuncture Pomegranate seeds?

72
Pancreatic Cancer

73
Pancreatic Cancer Fourth leading cause of death from cancer in the U.S. 5 year survival rate is 4% American Cancer Society estimates that in 2014 there will be 46,420 new cases and 39,590 deaths from pancreatic cancer. 3% of all cancer in the U.S. Accounts for 7% of cancer deaths

74
Pancreatic Cancer Risk Factors Age Smoking Chronic pancreatitis
Most significant Twice as likely to get CA Chronic pancreatitis Lots of associations between diseases and pancreatic CA, but cause-and-effect relationship has not been established

75
Pancreatic Cancer S/S Pain Jaundice Wt loss Dull epigastric pain
Back pain DVT CA in body or tail of pancreas

76
Pancreatic Cancer Tumor on head of pancreas- obstructs bile flow, jaundice Tumor on body of pancreas- impinges celiac ganglion pain Tumor on tail of pancreas- metastasizes before symptoms appear

77
Diagnosis Pt hx Physical exam
Elevated serum bilirubin and alkaline phosphate Suggest pancreatic cancer, but not diagnostic Ultrasound CT scans Percutaneous fine-needle aspiration cytology Misses the smaller, more curable tumors

78
Treatment Surgical resection of tumor Radiation, chemotherapy
Most cancers have metastasized before it is diagnosed Radiation, chemotherapy Whipple Procedure

79
Whipple Procedure Pancreaticoduodenectomy (PD)
Removal of head of pancreas, distal bile duct, gallbladder, duodenum, small part of jejunum, distal stomach and pylorus Complications: Delayed gastric emptying Dumping Weight loss Diabetes Mellitus Nutrient deficiencies Malabsorption

80
Liver Gallbladder Removed Jejunum Head of pancreas removed

81
Source: SMART Imagebase
(
")
83
Whipple Procedure Post-operation symptoms
N/V, bloating, early satiety, abdominal pain Dumping Weight loss d/t pancreatic insufficiency Diabetes d/t decreased insulin production Nutrient deficiencies d/t malabsorption Ca, Zn, Cu, Se Vits A, E, D, K Bacterial overgrowth in small intestine Lactose intolerance

84
Whipple Procedure Treatment of symptoms (similar to any gastric surgery) Small frequent meals Drink most of your fluids between meals Eat slowly Avoid simple sugars Increase protein intake Limit fat to <30% Avoid sugar alcohols

85
Case Study

86
Case Study- Assessment
Background JM is a 29-year-old white male PhD student in English School full-time Lives w/ roommates Jewish Hx Dx of depression s/p appendectomy age 12 No tobacco use Family hx: Mother: breast CA; Father: HTN Alcohol use: 6 pack beer, 4-5 shots bourbon daily; weekends: wine and other mixed drinks

87
Case Study- Assessment
Admit hx Friend brings him to ER b/c he has acute abdominal pain, N/V States he didn’t realize how much alcohol he had been consuming since he went off his antidepressant meds Chief complaint: “My stomach pain is so bad- I just can’t stand it. I can’t seem to quit vomiting and cannot keep anything down.” Pt is pale and obese, in obvious distress

88
Case Study- Assessment
Vital Signs Temp: 101.7ºF Pulse: 108 bpm Resp rate: 27 BP: 132/96 Ht: 5’11” Wt: 245 HEENT: WNL, except dry mucus membranes in nose and throat Hyperactive bowel sounds, tender abdomen

89
Case Study- Assessment
Medications: Imipenen Pepcid Meperidine Ondansetron Colace - laxative MOM - laxative Ativan

90
Case Study- Assessment
Nutrition NPO Fluid: mL Hx: Pt state he has gained 50lbs in the last 5 years. Eats out for most dinners. Coffee w/ toast or bagel for breakfast. Sub sandwich or pizza for lunch

91
Case Study- Assessment
MD progress note Day after admit, reports hypoactive bowel sounds HEENT: WNL Dx: Acute Pancreatitis

92
Case Study- Assessment

93
Case Study- Assessment

94
Case Study- Assessment

95
Case Study- Diagnosis PES statement
Excessive alcohol intake r/t stress and depression AEB reported alcohol intake.

96
Case Study- Monitor/Evaluation
Labs Weight Vitals Symptoms Acute- probably won’t be in the hospital longer than a week. Will probably resolve itself. Manage symptoms.

97
Sample diet PM Snack Breakfast AM Snack Dinner HS Snack Lunch
Celery w/ PB Oatmeal w/ mixed berries Raisins Milk (LF) Wheat thins AM Snack Dinner Toast with jam Pasta String cheese (LF) Spinach Salad w/ LF dressing Carrots HS Snack Lunch Apple Grilled cheese Pudding Chicken noodle soup Elemental J-tube Low fat MCT Avoid odorous foods
 Wheat thins. AM Snack. Dinner. Toast with jam. Pasta. String cheese (LF) Spinach Salad w/ LF dressing. Carrots. HS Snack. Lunch. Apple. Grilled cheese. Pudding. Chicken noodle soup. Elemental J-tube. Low fat. MCT. Avoid odorous foods.")
98
References

99
References Pagana KD, Pagana TJ. Mosby’s Manual of Diagnostic and Laboratory Tests. 5th edition. St. Louis, MO: Mosby, Inc; 2010. Krauss About Acute Pancreatitis. Available at Accessed March 4, 2015.

100
References Yadav D, Lowenfels AB. The epidemiology of pancreatitis and pancreatic cancer. Gastroenterology. 2013;144(6):
:")
Similar presentations



 EXOCRINE PANCREASE Lecture Dr. Gamal Hamra Wednesday 01/12/1430 (18/11/2009)>")

>")




 muscle proteins liver glycogen fat lipids glucose.>")









