Download presentation
Presentation is loading. Please wait.

1
Diagnostic Imaging of the Gastrointestinal Tract

2
Plain Radiographs Contrast Studies Ultrasound

3
Plain Radiographs Demonstrate distribution of fluid and gas within the tract

4
Plain Radiographs In normal abdomen dependant on radiographic contrast

5
Plain Radiographs Ascites significantly impairs diagnostic utility

6
Loss of serosal detail due to hydroperitoneum

7
Plain Radiographs Cannot resolve soft tissue opacities as separate structures

8
Ultrasound Resolves soft tissue opacities

9
Tumour within wall of small intestine

10
Ultrasound can see the wall lesion within the fluid filled loop of bowel, plain radiographs cannot

11
Ultrasound Cannot image through gas

12
Plain Radiographs and Ultrasound are complementary

13
Contrast Radiography Allows visualization of the mucosal surface and indicates status of bowel lumen

14
Contrast Radiography Provides data regarding GI function

15
Esophagus

16
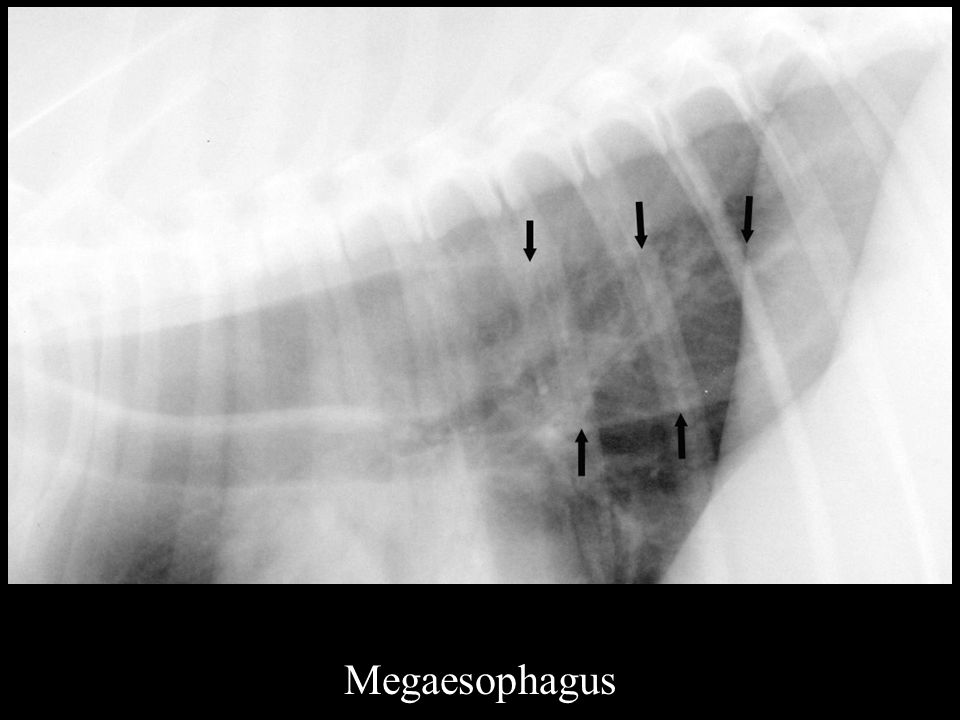
Megaesophagus Esophageal Foreign Body

17
Megaesophagus Retention of air or food material within the esophagus

18
Megaesophagus

20
Contrast study required only if do NOT see distended esophagus on plain radiographs

21
Megaesophagus Retention of barium within the esophagus

22
Normal Barium Swallow

23
Megaesophagus

24
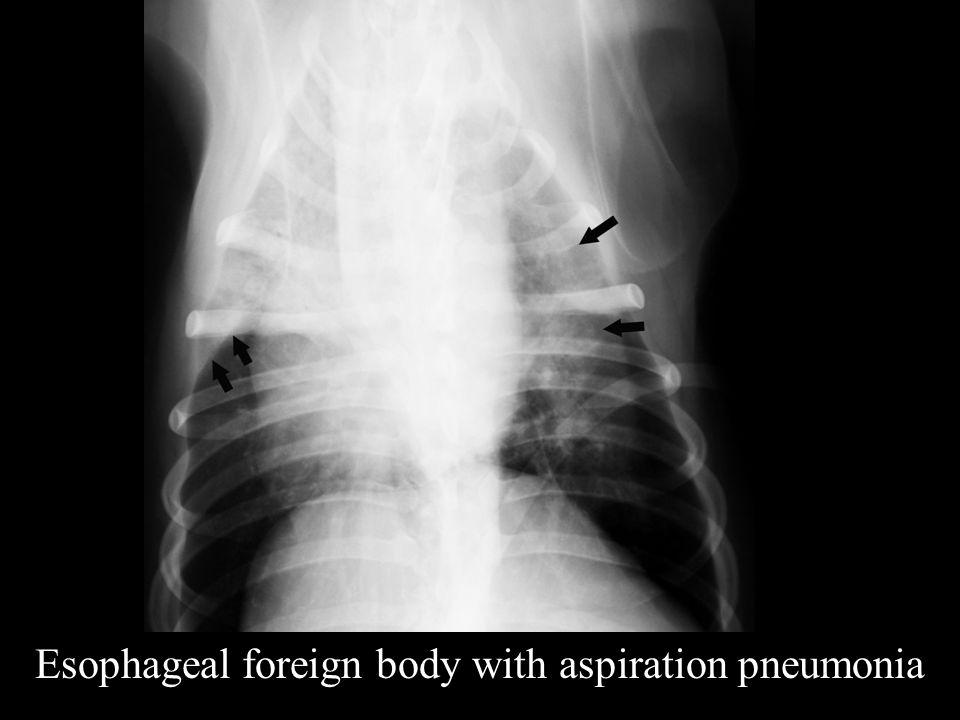
Esophageal Foreign Body

25
Usually easy to identify Good contrast with aerated lung

26
Esophageal Foreign body

27
Aspiration pneumonia is a common complication

28
Esophageal foreign body with aspiration pneumonia

30
Stomach

31
Gastric Dilation with Volvulus GDV

33
Right lateral projection

35
Gastric Ileus

36
Gastric Ileus Normal Stomach

37
Normal Stomach

38
Foreign Bodies

39
Radiopaque Foreign Body

40
Semi radiopaque foreign body

42
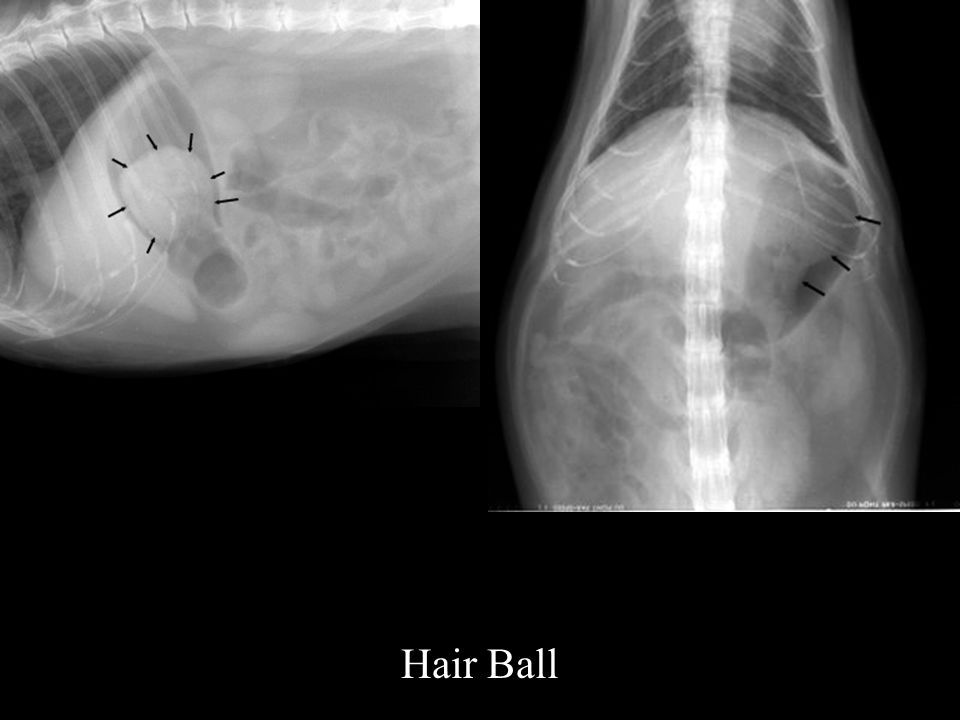
Hair Ball

44
Hairball v Food Material?

45
Hairball has smooth margins and may not contact stomach wall Do not disappear following fasting

46
Food material has irregular margins usually in contact with stomach wall Disappears following fasting

47
Fibres e.g. carpet, socks are difficult to identify on plain radiographs and ultrasound and frequently require contrast radiography

48
Double Contrast Gastrogram

49
Naso-gastric intubation

50
1-2 mls/kg undiluted barium 20ml/kg room air

51
Left lateral Right lateral Ventrodorsal Dorsoventral

52
Normal Double Contrast Gastrogram

53
Carpet Foreign Body

54
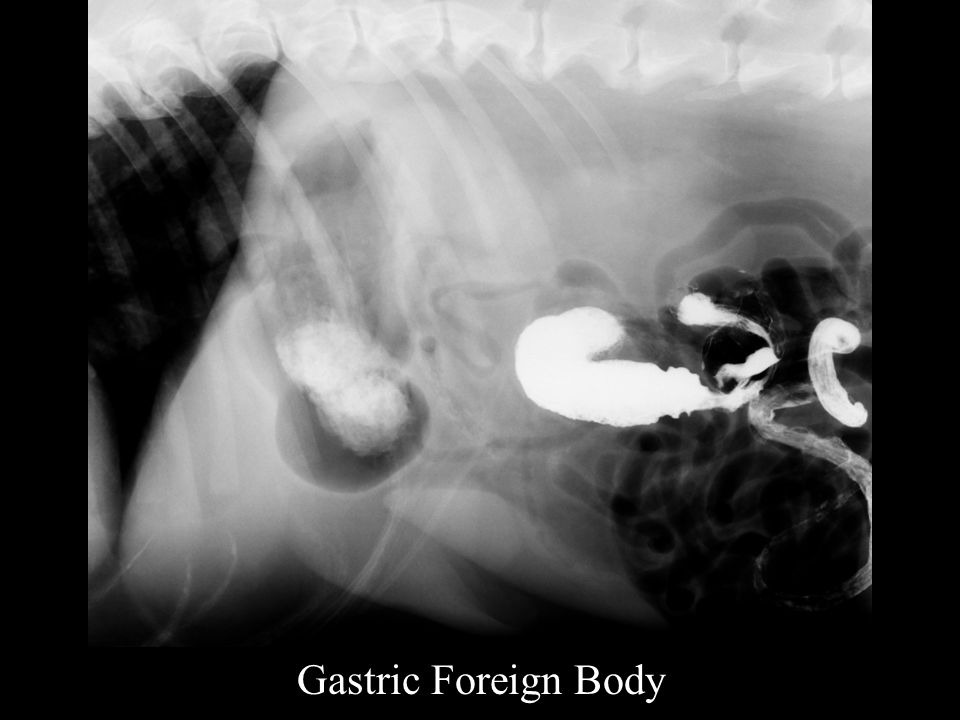
Gastric Foreign Body

57
Gastric Tumours

58
Uncommon

59
Filling defect on contrast study

60
May identify on ultrasound

61
But easily missed if stomach is gas filled

62
Gastric Tumour

63
Pyloric Dysfunction

64
Obstruction of pyloric outflow

65
Congenital

66
Obstruction of pyloric outflow Congenital Acquired Neoplasia

67
Obstruction of pyloric outflow Congenital Acquired Neoplasia Fibrosis

68
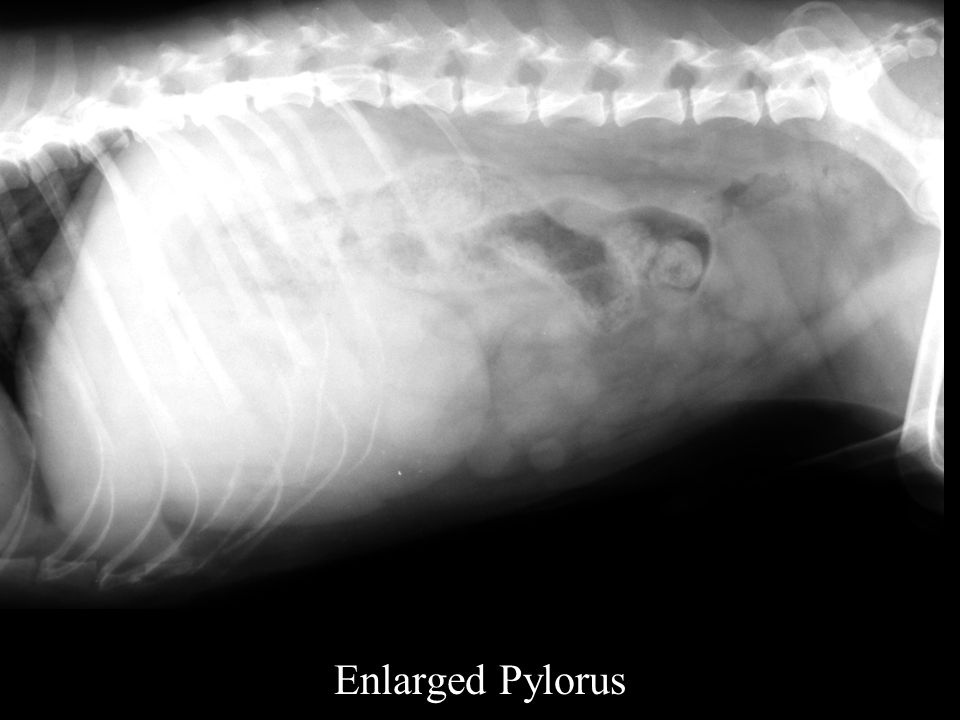
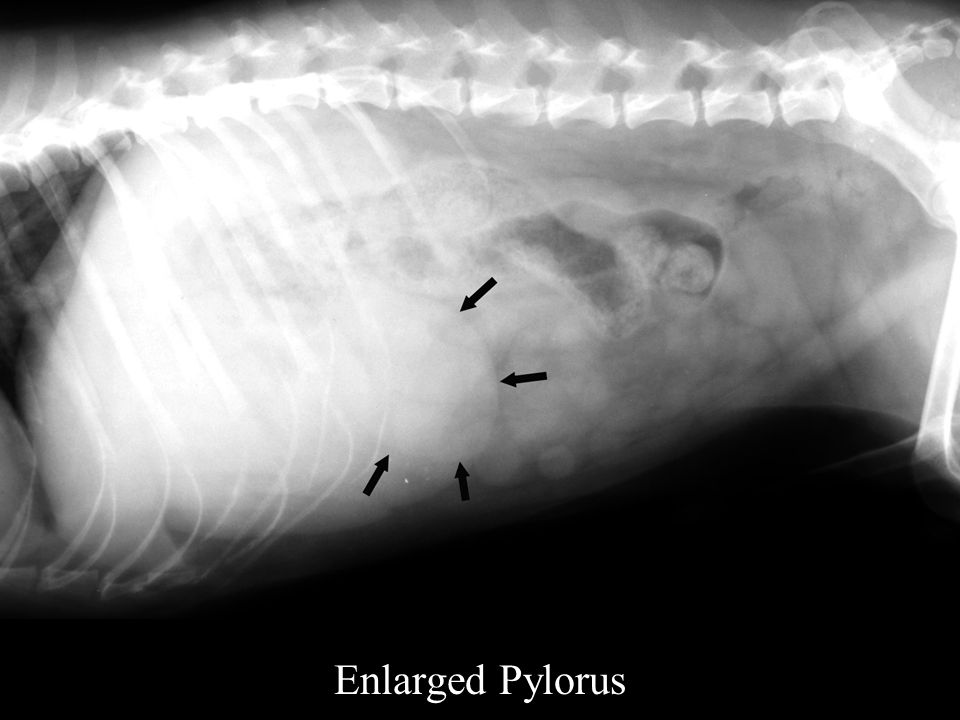
Plain Radiographs Enlarged Pylorus

71
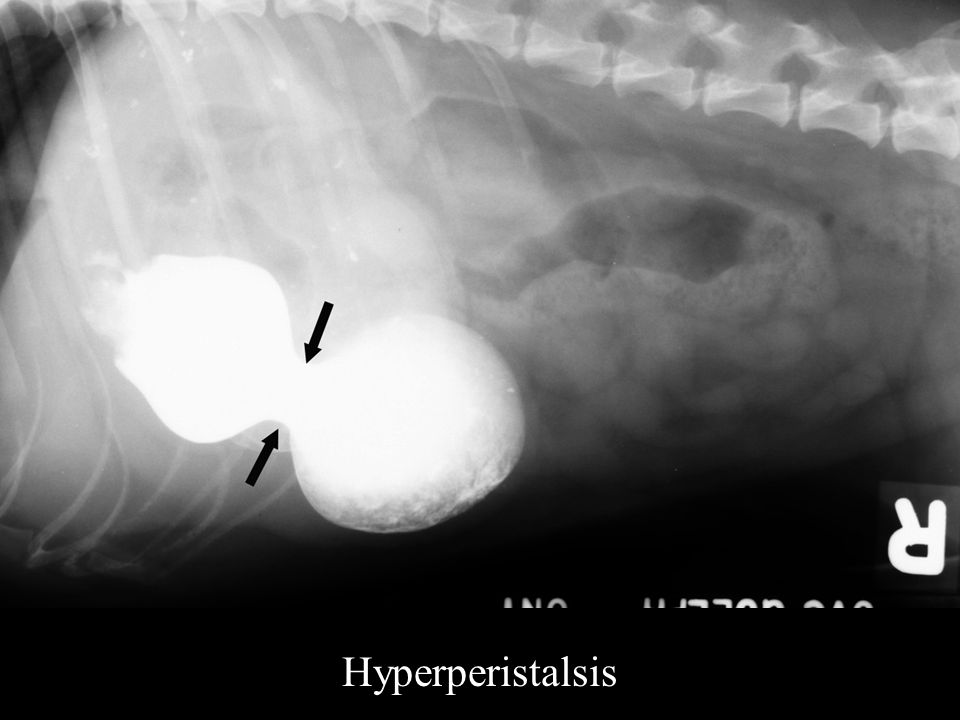
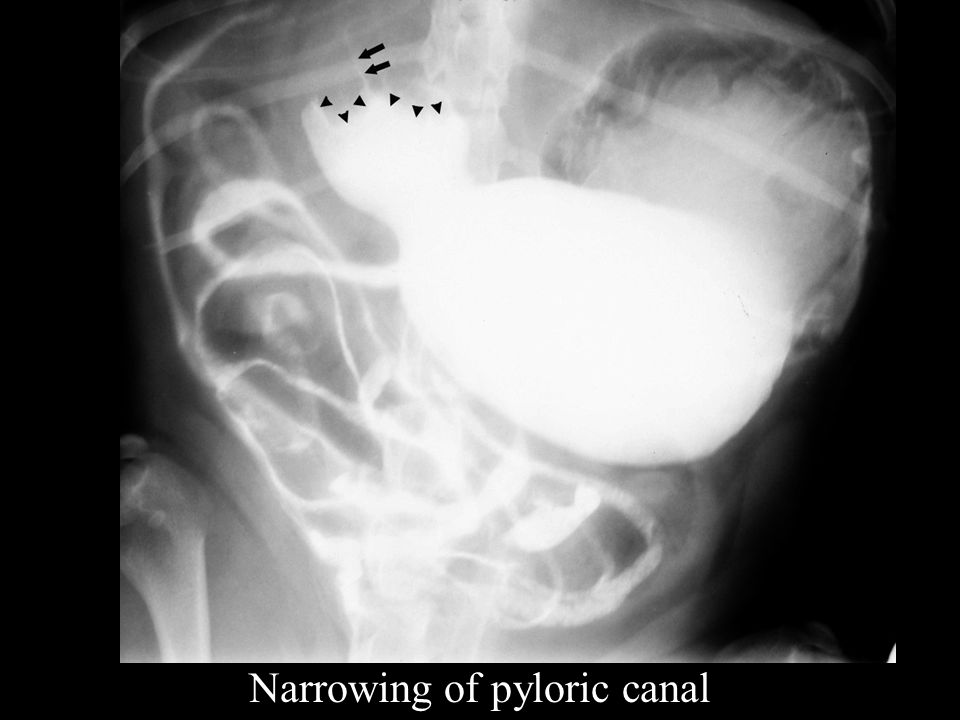
Contrast Study Hyperperistalsis

73
The hourglass appearance must be present on several radiographs

74
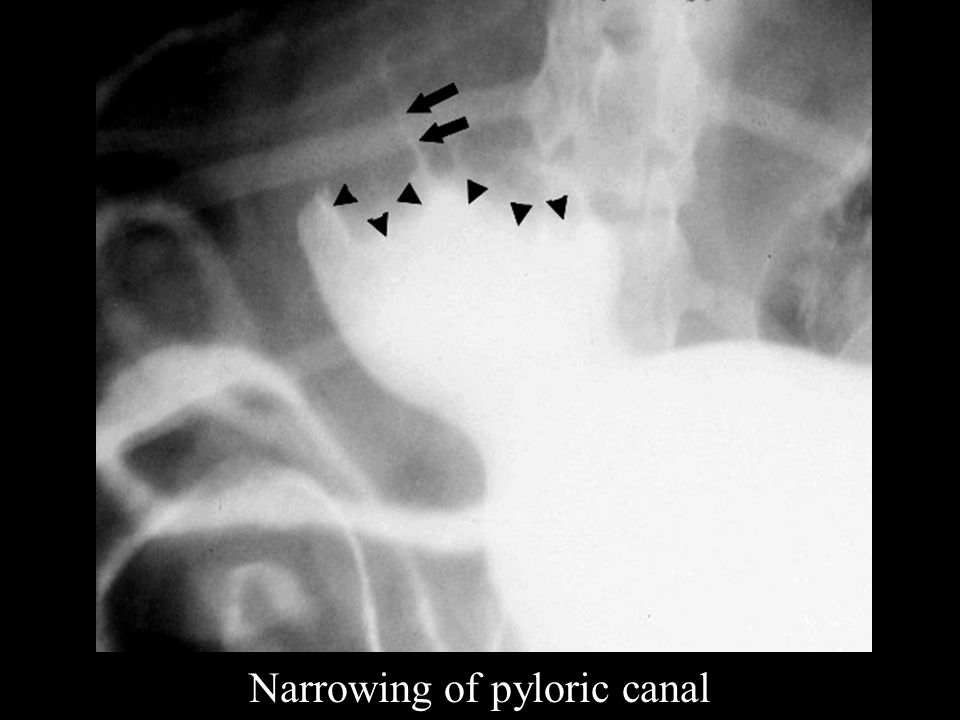
Narrowing of pyloric canal

75
String or bird’s beak appearance

76
Narrowing of pyloric canal

79
Small Intestine

80
Obstruction is commonest abnormality identified

81
Foreign Body Intussuception Tumour

82
Foreign body most common

83
Complete obstruction v Partial obstruction

84
Normal width of small intestine 2-3 X width of a rib Width of a vertebral body

85
Obstruction results in fluid or gas distension or a combination of both

86
Foreign body may be Radiopaque Semi-radiopaque Radiolucent

87
Radiopaque small intestinal foreign body

88
Semi radiopaque small intestinal foreign body

92
Radiolucent small intestinal foreign body

93
Occasionally early enteritis, especially parvo virus infection will present with intestinal distension

94
Parvo virus enteritis

95
Cases with clear plain radiographic evidence of obstruction require surgery

96
They do not require an upper gastrointestinal series

97
The decision to perform an upper gastrointestinal study or a laparotomy is influenced by experience in interpreting the plain radiographs

98
Clear evidence of rupture of the gastrointestinal tract is a contraindication to an upper gastrointestinal series

99
Long standing cases of obstruction will also have hydroperitoneum

100
Pneumoperitoneum secondary to intestinal rupture

102
Fibres e.g. carpet or socks have a characteristic appearance on contrast studies

103
Look for a linear or reticular fibre pattern

104
Sock foreign body

106
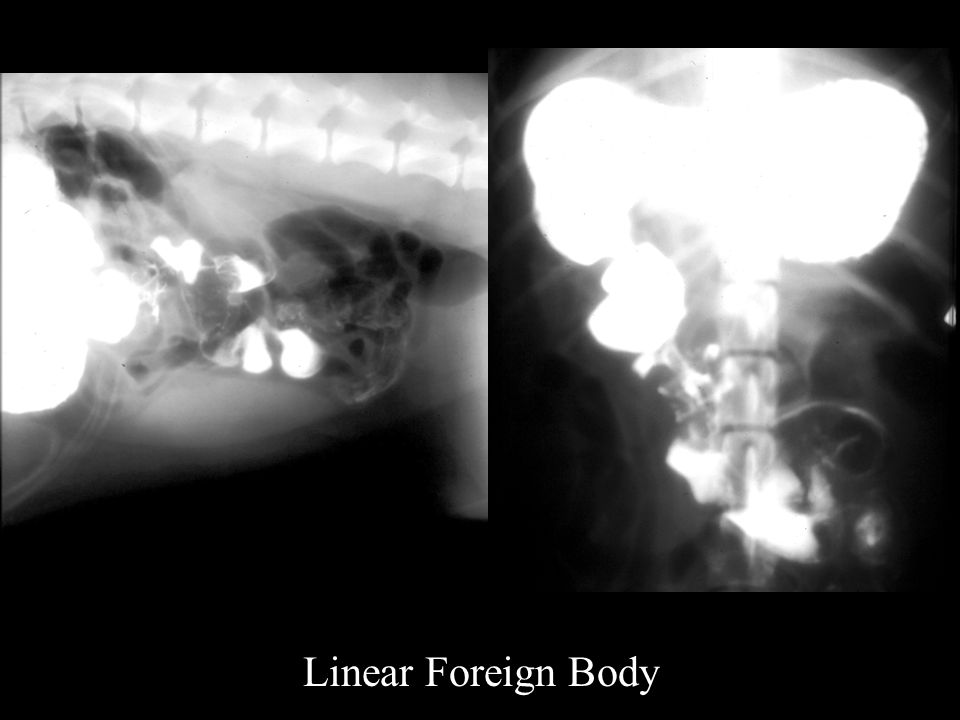
Linear Foreign Body

107
Contrast column has acute angles with contrast accumulation at the angles

108
Linear Foreign Body

111
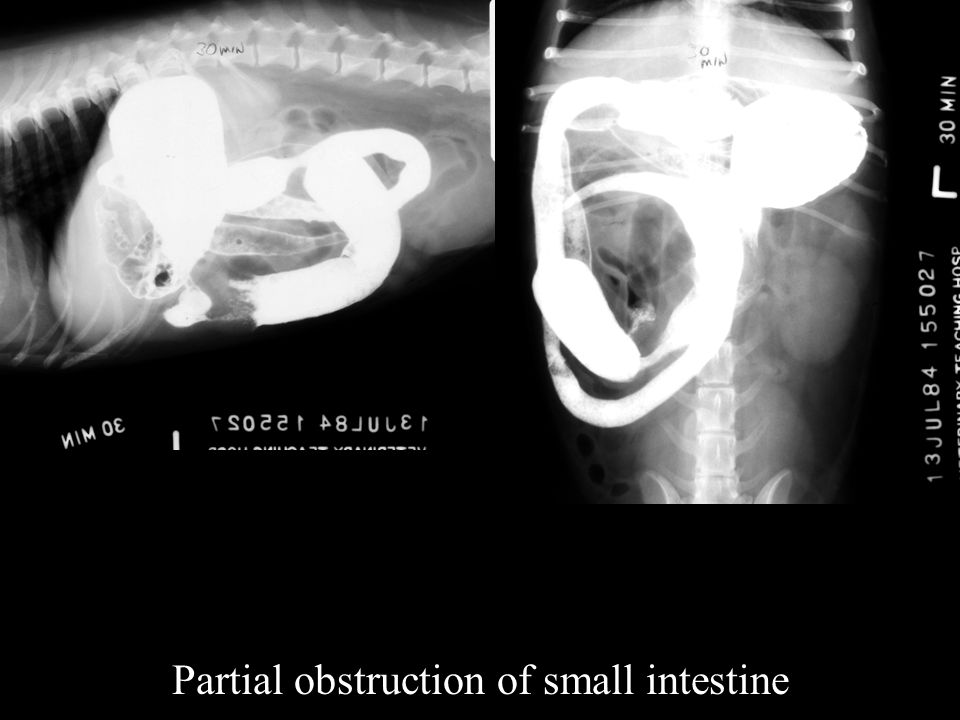
Partial obstruction of the small intestine

112
More challenging on plain radiographs

113
Partial obstruction of small intestine

116
Small Intestinal Tumours

117
Ultrasound most useful imaging modality

118
Normal small intestine 5 layers

119
Mucosal surface – white Mucosa – black Submucosa – white Muscularis – black Serosa – white

120
Normal small intestine

122
Normal single wall thickness <5mm

123
Intestinal Tumour Focal lesion

124
Intestinal tumour

125
Diffuse Thickening of Small Intestine

126
Gastro Intestinal Lymphoma Inflammatory Bowel Disease

127
Gastro Intestinal Lymphoma

128
Tumours of colon Uncommon

129
Normal colon

130
Tumour of the colon

131
Intussuception Rarely diagnosed definitively on plain radiographs

132
Intussuception Presents as non specific obstruction of small intestine

133
Ultrasound Target appearance Or Too many layers

134
Intussuception Requires a contrast study or ultrasound evaluation for confirmation

135
Intussuception

136
Contrast Radiographs Coiled spring appearance

137
Intussuception

138
Mega Colon

Similar presentations