Download presentation
Presentation is loading. Please wait.

1
INFECTION AND PRETERM BIRTH

2
Sequelae of Preterm Birth PerinatalMortality NeurologicHandicap (75%) (50%) (10%)
 (50%) (10%)")
3
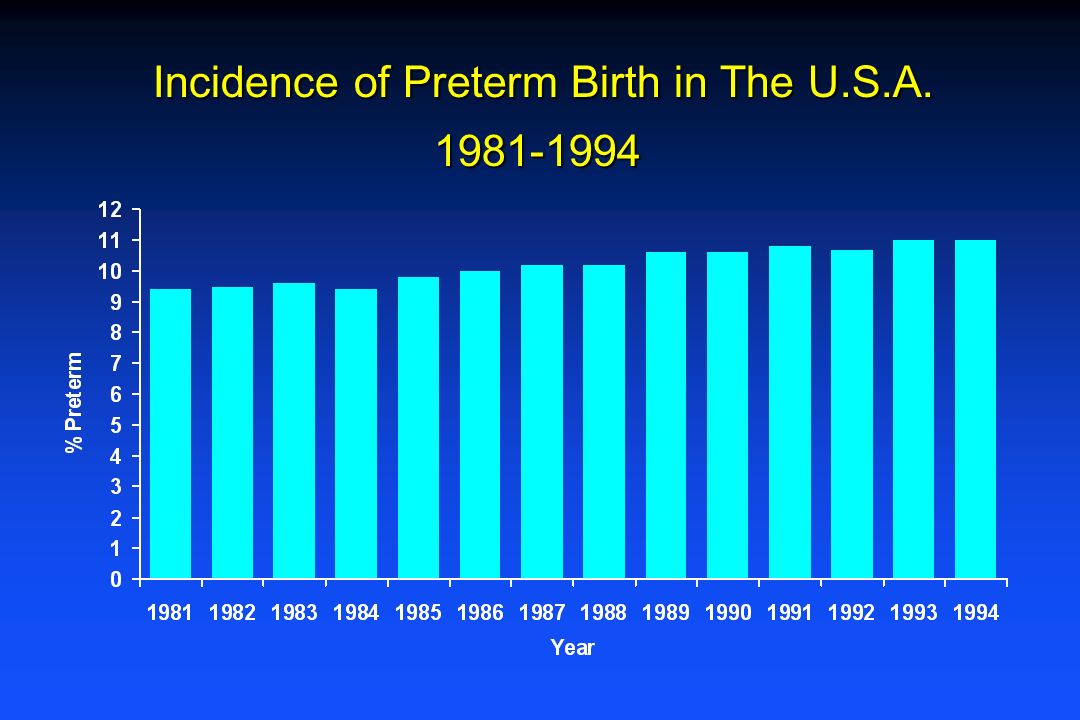
Incidence of Preterm Birth in The U.S.A. 1981-1994 Incidence of Preterm Birth in The U.S.A. 1981-1994
4
Time Trends in Low Birth Weight (<1,500 g) by Race/Ethnicity - United States, 1970-1990
 by Race/Ethnicity - United States,")
5
UAB Infants with Birthweights 1000 Grams Mean BWSurvival 1975900 gms17% 1980860 gms48% 1985820 gms56% 1990804 gms74%

6
Distribution of Neonatal Mortality BWT (gms) Distribution <100060% 1000-2500 20% >250020%* *Majority associated with congenital anomalies
 Distribution <100060% % >250020%* *Majority associated with congenital anomalies")
7
Approximate Prevalence of Cerebral Palsy per 1,000 Births by Birth Weight and Gestational Age LBW-PORT 0500100015002000250030003500400045005000 Birth Weight (g) / Gestational Age (wks) 0 10 20 30 40 50 Prevalence of Cerebral Palsy per 1,000 Live Births Term 230 240 250 23 27 3236
 / Gestational Age (wks) Prevalence of Cerebral Palsy per 1,000 Live Births Term")
8
Survival Rate for Extremely Small Infants (<800g) in Relation to Mid-Year of Birth 0 20 40 60 80 1975 19801985 1990 Mid-Year of Birth Survivors per Livebirth, % Lorenz, 1998
 in Relation to Mid-Year of Birth Mid-Year of Birth Survivors per Livebirth, % Lorenz, 1998")
9
Prevalence of Disability Among Extremely Small Survivors (<800g) in Relation to Mid-Year of Birth Mid-Year of Birth 0 10 20 30 40 50 60 70 1975 19801985 1990 Disabled Infants per Survivor, % Lorenz, 1998
 in Relation to Mid-Year of Birth Mid-Year of Birth Disabled Infants per Survivor, % Lorenz, 1998")
10
Percentage of Extremely Small (<800g) Livebirths Surviving with at Least One Disability in Relation to Mid-Year of Birth 1990 Mid-Year of Birth 0 5 10 15 20 197519801985 Disabled Infants per Livebirth, % Lorenz, 1998
 Livebirths Surviving with at Least One Disability in Relation to Mid-Year of Birth 1990 Mid-Year of Birth Disabled Infants per Livebirth, % Lorenz, 1998")
11
Cerebral Palsy in <1000gm infants Survivors with Any Disability**(n)3212802560 Survivors with CP* (n)166401280Survivors(n)2008,00016,000Survival(%)14080 <1000g births (n)20,00020,00020,000Year196019851997 *Assuming an 8% incidence in survivors consistently over time. **Assuming a 16% incidence in survivors consistently over time.

12
Etiology of Preterm Birth Etiology of Preterm Birth 50% 30% 20% Spontaneous Preterm Labor Preterm Birth for Maternal or Fetal Indications Premature Rupture of Membranes

13
REVIEW OF INTERVENTIONS TO PREVENT PRETERM BIRTH l Prenatal care l Risk screening l Nutrition counseling l Caloric supplementation l Protein supplementation l Iron supplementation l Most labor inhibiting agents l Drug, alcohol and tobacco cessation programs l Bed rest l Hydration l Home uterine activity monitoring Commonly used interventions which have not been shown to reduce preterm birth include:

14
INFECTION AND PRETERM BIRTH

15
SURGICAL PATHOLOGY REPORT Clinical History 34 year old white female with an intrauterine pregnancy at 25 and 3/7th weeks. Microscopic Description Sections of the free fetal membranes show severe, necrotizing chorioamnionitis. Both umbilical arteries as well as the umbilical vein exhibit funisitis.

16
Infection and Labor In 1927, Harris and Brown reported culturing women undergoing C- section with intact membranes. STATUSRESULTS (# POSITIVE) No labor0/21 Labor <5 hours0/5 Labor >5 hours6/7 (4/6 anaerobic) They concluded that organisms could reach the amniotic fluid with intact membranes and that fever was not a reliable sign of infection in labor.
 No labor0/21 Labor <5 hours0/5 Labor >5 hours6/7 (4/6 anaerobic) They concluded that organisms could reach the amniotic fluid with intact membranes and that fever was not a reliable sign of infection in labor..")
17
Infection in the female reproductive tract can cause premature rupture of the membranes and induce premature labor…. The membranes in all premature cases in this series show evidence of infection…. In most instances this reaction is severe. Infection in the female reproductive tract can cause premature rupture of the membranes and induce premature labor…. The membranes in all premature cases in this series show evidence of infection…. In most instances this reaction is severe. Knox, Am J Obstet Gynecol 1950

18
Infection and Prematurity Elder treated 279 non-bacteriuric women with a 6- week course of 1gm tetracycline daily or a placebo beginning at <32 weeks gestation. Tetracycline treated women had fewer preterm births. Elder, 1971

19
Infection and Preterm Labor In 1977 Bobitt and Ledger performed amniocenteses on 10 women in preterm labor with intact membranes. 7 had colony counts >1000 per ml with anaerobic organisms predominating. “It appears that bacteria can penetrate the fetal membranes and contaminate the amniotic fluid” “In patients in premature labor, the role of unrecognized amnionitis should be reevaluated.” Bobitt & Ledger, 1977 J Reprod Med

20
Intrauterine Infection l Clinical chorioamnionitis l Sub-clinical chorioamnionitis –Organisms in amniotic fluid and membranes –Organisms only in membranes

21
Of women with positive chorioamnion cultures, only 50% also have positive amniotic fluid cultures.

22
INFECTION AND PREMATURITY Only 8% of women with histologic chorioamnionitis have clinical signs (fever and uterine tenderness) prior to delivery. Gusick 1985

23
Chorioamnionitis Histologic studies suggest a clear progression of granulocyte infiltration: Maternal Granulocytes Decidua Chorion Amnion Amniotic fluid Umbilical Cord Umbilical vessels Wharton’s Jelly Amniotic fluid Granulocytes in AF likely represent both a maternal and fetal response.

24
Funisitis l Prior to 1970, funisitis was thought to represent a sign of asphyxia l In 1970, Cassady showed that funisitis was associated with intrauterine infection - not asphyxia l The only proven intrauterine and fetal infection occurring in the absence of funisitis was Group B strep Overbach and Cassady, Pediatrics 1970

25
Chorioamnionitis l Funisitis is present in about half the cases of histologic chorioamnionitis and is almost never seen alone. l This suggests that the etiologic infection almost always starts in the chorioamnion.

26
Intrauterine Infection and Preterm Labor Relationship to Gestational Age

27
0 10 20 30 40 50 60 70 80 90 100 21-2425-2829-3233-3637-4041-44 Weeks Gestation Prevalence at Delivery of Histologic Chorioamnionitis at Different Stages of Gestation Russell, P. Am J Diag Gyn Obst. 1979;1:127 Percent

28
Incidence of Chorioamnionitis in Preterm Delivery Patients 6/9 11/19 17/33 27/120 295/1526 % with Chorioamnionitis Gestational Age (weeks) Mueller-Heubach 1990
 Mueller-Heubach 1990")
29
Histological Chorioamnionitis % Birthweight (g) Chellam, 1985
 Chellam, 1985")
30
Patients in Labor with Intact Membranes % Positive Amniotic Fluid Cultures Gestational Age (weeks) Watts, Ob/Gyn 79:351, 1992 20/105 (19%) + Cultures
 Watts, Ob/Gyn 79:351, /105 (19%) + Cultures")
31
0 20 40 60 80 100 Spontaneous Indicated Chorioamnion Colonization Indicated vs. Spontaneous Delivery <1000 1000-1499 1500-2499 2500 Birthweight (grams) % Positive Cultures
 % Positive Cultures.")
32
Etiology of Spontaneous PTB Infection Other Pathologies No Pathology Gestational Age

33
Etiology of Spontaneous Preterm Birth Single potent risk factor (Infection and placental abruption) Multiple weaker risk factors acting through usual hormonal pathways 20 weeks 36 weeks Mediating Factors cervical strength cervical strength uterine contractility uterine contractility host defenses host defenses
 Multiple weaker risk factors acting through usual hormonal pathways 20 weeks 36 weeks Mediating Factors cervical strength cervical strength uterine contractility uterine contractility host defenses host defenses")
34
Histologic Chorioamnionitis Evidence of chronicity 1. Ureaplasma diagnosed by amniocentesis (PCR or culture) at 15-20 wks delivery with HCA at 24-28 wks. 2. IL-6 in amniotic fluid at 15-20 wks delivery with HCA at <32 to 34 wks. 3. FFN (a marker for membrane disruption) in vagina or cervix at 13-24 wks - associated with HCA at 29-31 wks.
 at wks delivery with HCA at wks. 2. IL-6 in amniotic fluid at wks delivery with HCA at <32 to 34 wks. 3. FFN (a marker for membrane disruption) in vagina or cervix at wks - associated with HCA at wks..")
35
Recurrent Preterm Birth Women with recurrent spontaneous preterm births <32 weeks are more likely to have histologic chorioamnionitis than other women giving birth at similar gestational ages. Salafia, SMAM 2001

36
Bacteria Associated with Prematurity UreaplasmaMycoplasmaGardnerellaMobiluncusPeptostreptococcusBacteroides Low Virulence

37
Choriodecidual bacterial colonization (endotoxins and exotoxins) Fetal tissue response Fetus Increased corticotropin-releasing hormone Increased adrenal cortisol production Myometrial contractions Chorioamnion weakening and rupture Preterm Delivery Increased prostaglandins Decreased chorionic prostaglandin dehydrogenase Chorioamnion and placenta Maternal response Decidua Increased cytokines and chemokines Neutrophil infiltration Increased metalloproteases Cervical ripening
 Fetal tissue response Fetus Increased corticotropin-releasing hormone Increased adrenal cortisol production Myometrial contractions Chorioamnion weakening and rupture Preterm Delivery Increased prostaglandins Decreased chorionic prostaglandin dehydrogenase Chorioamnion and placenta Maternal response Decidua Increased cytokines and chemokines Neutrophil infiltration Increased metalloproteases Cervical ripening")
39
Bacterial Vaginosis and Preterm Birth

40
Normal vaginal secretions Bacterial vaginosis

41
BV and Prematurity The odds ratio for preterm birth in association with BV in nearly every study ranges from 1.5 to 3.0

42
BV and Preterm Birth Women with BV type organisms such as gardnerella, bacteroides and mycoplasma in the vagina early in pregnancy were significantly more likely to have these organisms in the amniotic fluid at the time of delivery. VIP Study Krohn, 1996

43
BACTERIAL VAGINOSIS Korn et al., in non-pregnant women, showed that BV was associated with plasma cell endometritis as well as with endometrial colonization by a number of organisms which are present in excessive numbers in women with BV.

44
Association of BV with Plasma Cell Endometritis Metritis (%) Positive Negative Korn et al., Obstet Gynecol 1995;85:387-90 Bacterial Vaginosis
 Positive Negative Korn et al., Obstet Gynecol 1995;85: Bacterial Vaginosis")
45
VIP Study, Am J Obstet Gynecol, 1996 GENITAL INFECTIONS IN PREGNANT WOMEN BY RACE ChlamydiaGonorrheaTrichomonasGroup B MycoplasmaBacterial Strep vaginosis

46
Nearly 50% of the excess preterm births and mortality in black versus white infants is explained by the increase in vaginal and intrauterine infections in black women

47
Fetal Fibronectin l A basement membrane protein l Produced primarily by fetal tissue, the placenta and membranes. l It may help to adhere the placenta and membranes to the decidua.

48
FETAL FIBRONECTIN A marker for upper genital tract basement membrane disruption

49
INFECTION AND PRETERM BIRTH

50
FFN AND PRETERM BIRTH Delivery (weeks)OR <2860 <3042 <3223 <3511 <375 +Goldenberg AJOG 1995
OR <2860 <3042 <3223 <3511 <375 +Goldenberg AJOG 1995")
51
ASSOCIATION OF FFN AND INFECTION 1. FFN is twice as common in women with BV 2. FFN was 16-20 fold more common in women who developed clinical chorioamnionitis 3. All women with FFN has histologic chorioamnionitis 4. FFN was 6 fold more common in women whose infants developed sepsis

52
TIMINGTIMING EventGestational Age (Weeks ± SD) Screening for FFN23.9 ±.06 Clinical Chorioamnionitis30.6 ± 4.1
 Screening for FFN23.9 ±.06 Clinical Chorioamnionitis30.6 ± 4.1")
53
SPECULATIONSPECULATION l At 24 weeks, FFN in the vagina or cervix is a marker for an asymptomatic upper genital tract infection which later manifests itself as spontaneous preterm labor or PROM frequently in conjunction with a perinatal infection.

54
Is pregnancy an antibiotic- deficient state?

55
Antibiotics in Labor and Preterm Birth

56
Antibiotics in Women with Preterm Labor and Intact Membranes Delayed Improved Infant StudyAntibiotic NDeliveryOutcome MacGregor, 1986Erythromycin17Yes No Morales, 1988Erythromycin, Ampicillin150Yes No Winkler, 1988Erythromycin 19Yes - Newton, 1989Erythromycin / Ampicillin95 No No MacGregor, 1991Clindamycin103Yes No McCaul, 1992Ampicillin40 No No Romero, 1993Ampicillin / Amoxicillin / Erythromycin275 No No Cox, 1995Ampicillin / Amoxicillin78 No No Gordon, 1995Ceftizoximine117 No No

57
Antibiotics in Women with Preterm Labor and Intact Membranes l Meta-analysis of existing RCTs l These results do not support the routine use of antibiotics in women in preterm labor Egarter et al, 1996

58
Antibiotics and Preterm Birth Labor with Intact Membranes Study GroupPlacebo Group Outcomen=43n=38 BWT (x) (g)23182093 Days to delivery (median) 15 2.5* Delivery <7 days (%)37%63%* NEC (%)0%13%* *p<.05 † greater prolongation occurred in <30 week pregnancies Metronidazole and Ampicillin for 6 days at ~30 weeks in a RCT Norman et al (South Africa), Br J Obstet Gynaecol, 1994
 (g) Days to delivery (median) * Delivery <7 days (%)37%63%* NEC (%)0%13%* *p<.05 † greater prolongation occurred in <30 week pregnancies Metronidazole and Ampicillin for 6 days at ~30 weeks in a RCT Norman et al (South Africa), Br J Obstet Gynaecol, 1994")
59
Antibiotics and Preterm Birth Labor with Intact Membranes AntibioticsPlacebo Outcome(n=59) (n=51)P value Days to delivery (x)4827.01 GA at delivery (wks) (x)3734.01 Birth <37 weeks (%)42%65%.01 BWT (g) (x)2662 2370.08 NICU Admission (%)40%63%.03 Neonatal sepsis (%)10%22%.18 Ampicillin and Metronidazole for 8 days at ~30 weeks in a RCT Svare et al (Denmark), Br J Ob Gyn 1997
 (n=51)P value Days to delivery (x) GA at delivery (wks) (x) Birth <37 weeks (%)42%65%.01 BWT (g) (x) NICU Admission (%)40%63%.03 Neonatal sepsis (%)10%22%.18 Ampicillin and Metronidazole for 8 days at ~30 weeks in a RCT Svare et al (Denmark), Br J Ob Gyn 1997")
60
Antibiotics in Women with Preterm Labor and Intact Membranes l The most promising studies used metronidazole. l the organisms found in upper tract infection associated with early preterm labor are likely to be more responsive to this antibiotic. l Additional RCTs to test the efficacy of metronidazole to reduce early preterm birth in laboring women are indicated.

61
Antibiotics Prior to Labor and Preterm Birth

62
A Randomized Trial of Cefamet-Pivoxil in High Risk Pregnant Women in Nairobi Number EGA at Rx Birthweight LBW (<2500g) PP Endometritis Antibiotics160 ~ 30 wks 292718.7%17.3%Placebo160 277232.8%31.6% Gichangi, Am J ObGyn, 1997 P.04.01.03
 PP Endometritis Antibiotics160 ~ 30 wks %17.3%Placebo %31.6% Gichangi, Am J ObGyn, 1997 P")
63
Rakai Study of Mass STD Treatment During Pregnancy Outcome Neonatal Death Preterm delivery T. vag B.V. Maternal NG/CT Infant NG/CT R.R.0.800.730.280.380.420.38 95% C.I. 0.69-0.940.54-0.990.17-0.460.21-0.680.25-0.700.21-0.68 *There was no difference in maternal HIV acquisition or in MCT of HIV or in stillbirths, spontaneous Ab or maternal death.

64
BV AND PRETERM BIRTH WHAT ARE WE TREATING?

65
BV and Prematurity Randomized trial of metronidazole in 80 women with BV and a previous PTB Rx = 18%Placebo = 39% p = <.05 Morales 1994

66
BV and Prematurity Randomized trial of metronidazole and erythromycin in women with BV and at high risk for PTB Rx = 23%Placebo = 37% p = <.001 Hauth 1994

67
BV During pregnancy at 14-26 weeks, intravaginal 2% Clindamycin cream cured BV (86%), but had no effect on the rate of preterm delivery - 15% vs. 13.5% for placebo. OR 1.1 (0.7-1.7). Indonesia Joesoef SER 1995
. Indonesia Joesoef SER")
68
BV Treatment and Spontaneous Preterm Birth MetronidazolePlaceboOR BV Positive11/242 (4.5%)15/238 (6.3%)0.71 (0.3-1.7) BV Positive and Prior PTB1/17 (5.9%)6/17 (35.3%)0.11 (0.0-1.2) BV Positive and Negative and Prior PTB2/22 (9.1%)10/24 (42%)0.14 (0.0-0.8) McDonald, 1997 Br J Obstet Gynaecol
15/238 (6.3%)0.71 ( ) BV Positive and Prior PTB1/17 (5.9%)6/17 (35.3%)0.11 ( ) BV Positive and Negative and Prior PTB2/22 (9.1%)10/24 (42%)0.14 ( ) McDonald, 1997 Br J Obstet Gynaecol")
69
BV and Preterm Birth Treating asymptomatic predominantly low-risk women with BV with two doses of 2 gm of metronidazole 48 hours apart, on two occasions did not reduce preterm birth

70
A randomized trial of antibiotics in 700 women positive for fFN showed no benefit in reducing spontaneous preterm birth.

71
Metronidazole to Prevent Preterm Birth Among Asymptomatic Pregnant Women with Trichomonas Vaginalis NICHD MFMU Network

72
Preterm Birth - Antibiotic Treatment l Old literature: oral tetracycline during pregnancy reduced SPB l Treatment of BV in high risk women with oral metro. and erythro. has reduced SPB l Topical treatment of BV has not reduced SPB l In women in SPL, penicillin-type antibiotics have not generally reduced SPB l Treatment of women in SPL with metro. and amp. has reduced SPB

73
PREMATURITY “The treatment of premature labor is identical with that already described for term labor and does not require further mention.” Williams 1908

74
Markers for Infection Markers for Infection Amniotic FluidAmniotic Fluid Plasma/SerumPlasma/Serum Vaginal FluidVaginal Fluid Cervical FluidCervical Fluid UrineUrine Saliva Saliva

75
Markers of Intrauterine Infection in Asymptomatic Women in Routine Prenatal Care Amniotic Fluid High interleukin-6 Cervix or Vagina Bacterial vaginosis High interleukin-6 High ferritin High fetal fibronectin High -FP High HCG High Prolactin High CICP Serum High GCSF High ferritin

76
Markers of Intrauterine Infection in Pregnant Women Women Presenting in Labor Amniotic Fluid Bacteria Low glucose High wt-cell count High GCSF High IL-1 High IL-6 Cervix or Vagina Bacterial vaginosis High GCSF High TNF- High IL-1 High IL-6 High IL-8 High fetal fibronectin Serum High GCSF High IL-6 High TNF- High C-reactive protein

77
Research Questions l When do bacteria invade the uterus? l What is the infection status of the uterus prior to conception? l What Mechanical and molecular mechanisms are associated with uterine invasion? l What are the protective mechanisms?

78
Why is the rate of genital tract infection so high in black women? Lack of access to treatment? Douching or other behaviors? Immunological differences? Greater risk of exposure? What strategies work to reduce these differences?

79
And what role does genetics play? None? Differences in immune response? Differences in chorioamnion membrane strength or ability to repair (keloids)? Differences in uterine muscle contractility?
. Differences in uterine muscle contractility .")
80
Research Questions l Which markers best predict current intrauterine infection? l Which interventions (i.e., antibiotics, anti-inflammatory agents) will reduce preterm birth and neonatal damage associated with intrauterine infection?
 will reduce preterm birth and neonatal damage associated with intrauterine infection .")
Similar presentations


>")








 and very expensive study of antioxidant.>")








