Download presentation
Presentation is loading. Please wait.

1
Who should access pump therapy? UK perspective Dr Thomas Ulahannan International Diabetes Federation European Region General Assembly Together We Are Stronger Warsaw, Poland 3-5 November 2006

2
Who should access pump therapy? Clinical criteria Clinical criteria many potential indications Patient preference Patient preference option in intensive insulin therapy Health Economic criteria Health Economic criteria resource limitations/cost effectiveness

3
Location of Gloucestershire in UK

5
NHS Hospital Services in Gloucestershire Gloucestershire Hospitals NHS Foundation Trust serves a population or around 500,000 Gloucestershire Hospitals NHS Foundation Trust serves a population or around 500,000 CSII is based at Gloucestershire Royal Hospital CSII is based at Gloucestershire Royal Hospital 18, 000 diabetes patients in county 18, 000 diabetes patients in county 1,800 type 1 diabetes under hospital follow up 1,800 type 1 diabetes under hospital follow up 55 current pump users 55 current pump users

6
UK National Institute for Health and Clinical Excellence (NICE) independent organisation responsible for providing national guidance on the promotion of good health and the prevention and treatment of ill health independent organisation responsible for providing national guidance on the promotion of good health and the prevention and treatment of ill health Technology Guidance 57: Continuous subcutaneous insulin infusion for diabetes (February 2003) determines NHS eligibility for CSII Technology Guidance 57: Continuous subcutaneous insulin infusion for diabetes (February 2003) determines NHS eligibility for CSII
 independent organisation responsible for providing national guidance on the promotion of good health and the prevention and treatment of ill health independent organisation responsible for providing national guidance on the promotion of good health and the prevention and treatment of ill health Technology Guidance 57: Continuous subcutaneous insulin infusion for diabetes (February 2003) determines NHS eligibility for CSII Technology Guidance 57: Continuous subcutaneous insulin infusion for diabetes (February 2003) determines NHS eligibility for CSII")
7
Technology Guidance 57 recommended CSII as an option for people with type 1 diabetes provided that recommended CSII as an option for people with type 1 diabetes provided that Multi Dose Injection (basal-bolus) therapy (including, where appropriate, the use of insulin glargine) has failed, Multi Dose Injection (basal-bolus) therapy (including, where appropriate, the use of insulin glargine) has failed, and those receiving the treatment have the commitment and competence to use the therapy effectively and those receiving the treatment have the commitment and competence to use the therapy effectively
 therapy (including, where appropriate, the use of insulin glargine) has failed, Multi Dose Injection (basal-bolus) therapy (including, where appropriate, the use of insulin glargine) has failed, and those receiving the treatment have the commitment and competence to use the therapy effectively and those receiving the treatment have the commitment and competence to use the therapy effectively")
8
randomized controlled trials indicate in type 1 diabetic subjects, the glycemic control on CSII is comparable with or only slightly better than MDI Pumps are relatively costly and special expertise needed If patients are doing well on MDI, CSII is not indicated After optimized MDI a trial of CSII is appropriate if poor control persists because of 1) frequent unpredictable hypoglycemia or 2) a marked dawn blood glucose rise. Continuous Subcutaneous Insulin Infusion at 25 Years Evidence base for the expanding use of insulin pump therapy in type 1 diabetes John Pickup, Harry Keen, Diabetes Care 25:593-598, 2002

9
Patients with erratic blood glucose concentration will fall into the first category when attempts to improve control lead to frequent hypoglycemia CSII is an effective means of managing diabetes during pregnancy but these patients, as a group, are not better controlled than during multiple injections Continuous Subcutaneous Insulin Infusion at 25 Years Evidence base for the expanding use of insulin pump therapy in type 1 diabetes John Pickup, Harry Keen, Diabetes Care 25:593-598, 2002

10
What is MDI failure? Defined as inability to achieve stable HbA1c <7.5% (or 6.5% with complications) without recurrent hypoglycaemia Defined as inability to achieve stable HbA1c <7.5% (or 6.5% with complications) without recurrent hypoglycaemia Therefore restricts CSII to a subgroup of Type 1 diabetes only but permits use in children and pregnancy Therefore restricts CSII to a subgroup of Type 1 diabetes only but permits use in children and pregnancy
 without recurrent hypoglycaemia Defined as inability to achieve stable HbA1c <7.5% (or 6.5% with complications) without recurrent hypoglycaemia Therefore restricts CSII to a subgroup of Type 1 diabetes only but permits use in children and pregnancy Therefore restricts CSII to a subgroup of Type 1 diabetes only but permits use in children and pregnancy.")
11
Benefits of NICE guidance Provides NHS funding for the pump, consumables, upgrades and clinical staff time as long as criteria are met Provides NHS funding for the pump, consumables, upgrades and clinical staff time as long as criteria are met All hospital appointments, consultations and training are provided without cost to the patient All hospital appointments, consultations and training are provided without cost to the patient

12
Potential benefits of CSII To the patient To the patient To the hospital To the hospital To primary care To primary care To the NHS To the NHS To wider society To wider society Glycaemic control Glycaemic control Reduced admissions Reduced admissions Less appointments Less appointments Lower costs Lower costs More productivity More productivity

13
Assessing benefits of CSII Previous studies have used economic models of projected long-term costs and outcomes of continuous subcutaneous insulin infusion (CSII) compared with multiple daily injections (MDI) in patients with Type 1 diabetes Previous studies have used economic models of projected long-term costs and outcomes of continuous subcutaneous insulin infusion (CSII) compared with multiple daily injections (MDI) in patients with Type 1 diabetes Scuffham P and Carr L. The cost-effectiveness of continuous subcutaneous insulin infusion compared with multiple daily injections for the management of diabetes. Diabet Med 2003; 20: 586 – 593. Scuffham P and Carr L. The cost-effectiveness of continuous subcutaneous insulin infusion compared with multiple daily injections for the management of diabetes. Diabet Med 2003; 20: 586 – 593.

14
Economic methods Typical measures Typical measures quality adjusted life expectancy (QALE) quality adjusted life expectancy (QALE) incremental cost-effectiveness ratio (ICER) and quality-adjusted life year (QALY) incremental cost-effectiveness ratio (ICER) and quality-adjusted life year (QALY) A common assumption is that improvements in glycaemic control associated with CSII lead to improved QALE by reduced incidence of diabetes- related complications A common assumption is that improvements in glycaemic control associated with CSII lead to improved QALE by reduced incidence of diabetes- related complications ICER of £25 648 €38 215 (£1=€1.49) per QALY gained is considered to represent good value for money by current standards in the UK. ICER of £25 648 €38 215 (£1=€1.49) per QALY gained is considered to represent good value for money by current standards in the UK.
 per QALY gained is considered to represent good value for money by current standards in the UK..")
15
Drawbacks of this approach local population and clinical conditions in which a pump service operates differ significantly from those assumed in the models local population and clinical conditions in which a pump service operates differ significantly from those assumed in the models cost savings from avoidance of complications of diabetes may take years to realize. cost savings from avoidance of complications of diabetes may take years to realize. front line clinicians and managers may not always be familiar with the economic modeling and measures such as QALE, ICER and QALY. front line clinicians and managers may not always be familiar with the economic modeling and measures such as QALE, ICER and QALY.

16
alternative to economic models directly monitoring of the effects of CSII introduction on directly monitoring of the effects of CSII introduction on relevant and important healthcare usage using the NHS national tariffs relevant and important healthcare usage using the NHS national tariffs in a single district general hospital in a single district general hospital and in local primary care providers. and in local primary care providers.

17
Patients and Methods Patients commencing CSII over a five year period between June 2000 and June 2005 inclusive were seen in a single district general hospital by one pump team Patients commencing CSII over a five year period between June 2000 and June 2005 inclusive were seen in a single district general hospital by one pump team Patients were selected for CSII according to NICE criteria (13) after these were available. Prior to NICE guidance, Type 2 diabetics were not excluded from consideration. Patients were selected for CSII according to NICE criteria (13) after these were available. Prior to NICE guidance, Type 2 diabetics were not excluded from consideration. All patients received intensive general diabetes education and carbohydrate counting training, initially on a one to one basis, and latterly using the REACCT (Re-Education And Carbohydrate Counting Training) programme (developed from DAFNE) All patients received intensive general diabetes education and carbohydrate counting training, initially on a one to one basis, and latterly using the REACCT (Re-Education And Carbohydrate Counting Training) programme (developed from DAFNE) DAFNE Study Group. Training in flexible, intensive insulin management to enable dietary freedom in people with type 1 diabetes: dose adjustment for normal eating (DAFNE) randomised control trial. BMJ 2002; 325 (7367): 746-751. DAFNE Study Group. Training in flexible, intensive insulin management to enable dietary freedom in people with type 1 diabetes: dose adjustment for normal eating (DAFNE) randomised control trial. BMJ 2002; 325 (7367): 746-751. Ross WI, Davies FC, Ulahannan TJ Re-Education And Carbohydrate Counting Training: REACCT Diabetic Medicine 2006; 23 (supp 2):96 Ross WI, Davies FC, Ulahannan TJ Re-Education And Carbohydrate Counting Training: REACCT Diabetic Medicine 2006; 23 (supp 2):96
 after these were available. Prior to NICE guidance, Type 2 diabetics were not excluded from consideration. All patients received intensive general diabetes education and carbohydrate counting training, initially on a one to one basis, and latterly using the REACCT (Re-Education And Carbohydrate Counting Training) programme (developed from DAFNE) All patients received intensive general diabetes education and carbohydrate counting training, initially on a one to one basis, and latterly using the REACCT (Re-Education And Carbohydrate Counting Training) programme (developed from DAFNE) DAFNE Study Group. Training in flexible, intensive insulin management to enable dietary freedom in people with type 1 diabetes: dose adjustment for normal eating (DAFNE) randomised control trial. BMJ 2002; 325 (7367): DAFNE Study Group. Training in flexible, intensive insulin management to enable dietary freedom in people with type 1 diabetes: dose adjustment for normal eating (DAFNE) randomised control trial. BMJ 2002; 325 (7367): Ross WI, Davies FC, Ulahannan TJ Re-Education And Carbohydrate Counting Training: REACCT Diabetic Medicine 2006; 23 (supp 2):96 Ross WI, Davies FC, Ulahannan TJ Re-Education And Carbohydrate Counting Training: REACCT Diabetic Medicine 2006; 23 (supp 2):96.")
18
Patient Management Suitability for a trial on pump therapy was decided jointly by the pump team if stable glucose control was not achieved despite intensive education and use of basal- bolus insulin regimes including insulin analogues where applicable. Suitability for a trial on pump therapy was decided jointly by the pump team if stable glucose control was not achieved despite intensive education and use of basal- bolus insulin regimes including insulin analogues where applicable. Patients not willing to comply with recommendations were not considered further for pump therapy. Patients not willing to comply with recommendations were not considered further for pump therapy. After 3 months patients were reassessed and if it was agreed by the pump team that the therapy was of benefit to the patients, they remained under the care of the same specialist team for pump therapy. After 3 months patients were reassessed and if it was agreed by the pump team that the therapy was of benefit to the patients, they remained under the care of the same specialist team for pump therapy. Healthcare resource utilization before and after CSII initiation were compared. Healthcare resource utilization before and after CSII initiation were compared.

19
Data Collection Data was collected for a maximum time of 60 months (5 years) before and after 60 months after CSII initiation Data was collected for a maximum time of 60 months (5 years) before and after 60 months after CSII initiation Routine hospital data was obtained on outpatient appointments in diabetes clinics appointments in other departments Routine hospital data was obtained on outpatient appointments in diabetes clinics appointments in other departments Hospital admission and discharge data was also reviewed Hospital admission and discharge data was also reviewed http://www.dh.gov.uk/assetRoot/04/13/44/04/04134404.xls http://www.dh.gov.uk/assetRoot/04/13/44/04/04134404.xls http://www.dh.gov.uk/assetRoot/04/13/44/04/04134404.xls
 before and after 60 months after CSII initiation Data was collected for a maximum time of 60 months (5 years) before and after 60 months after CSII initiation Routine hospital data was obtained on outpatient appointments in diabetes clinics appointments in other departments Routine hospital data was obtained on outpatient appointments in diabetes clinics appointments in other departments Hospital admission and discharge data was also reviewed Hospital admission and discharge data was also reviewed")
20
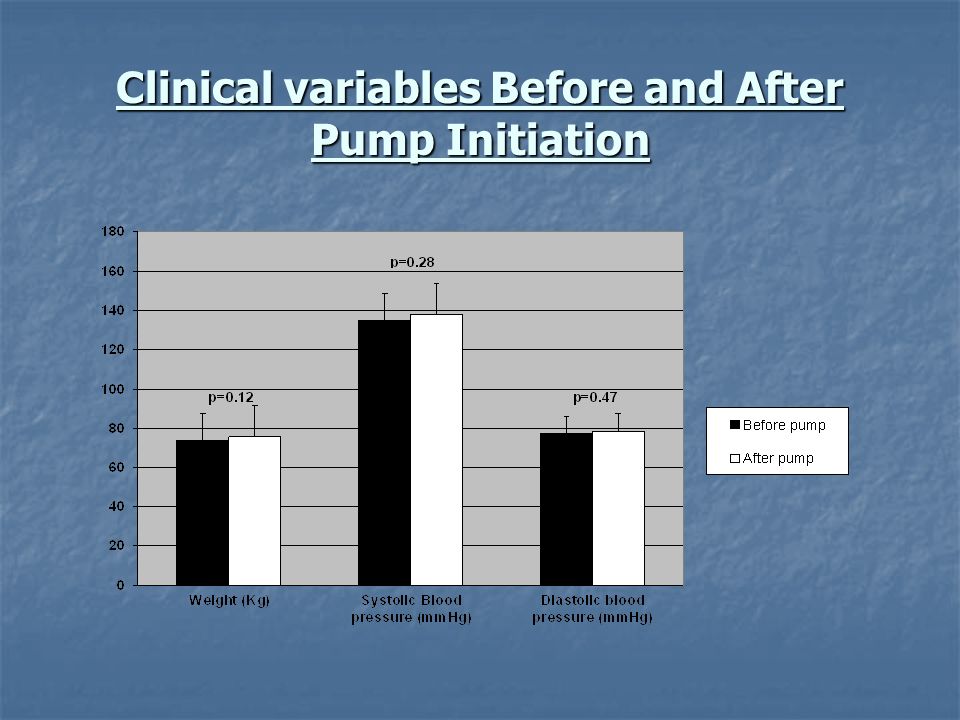
Clinical variables Before and After Pump Initiation

22
Appointments to see diabetes consultants, diabetes nurses and other specialties and admissions to hospital for diabetes or other causes according to hospital PAS data before and after CSII therapy Appointments (per month) Before Pump After Pump p value Consultant Diabetologist 0.20(0.10-0.80)0.11(0-0.30)<0.0001 Diabetes Specialist Nurse 0.40 (0- 1.5) 0.44(0-1.0)0.66 Diabetic Admission 0(0-0.10)0(0-0)0.028 Other Clinic 0.146(0-2.7)0.162(0-1.0)0.82 Other Admission 0.04(0-0.2)0(0-0.3)0.006
 Before Pump After Pump p value Consultant Diabetologist 0.20( )0.11(0-0.30)< Diabetes Specialist Nurse 0.40 (0- 1.5) 0.44(0-1.0)0.66 Diabetic Admission 0(0-0.10)0(0-0)0.028 Other Clinic 0.146(0-2.7)0.162(0-1.0)0.82 Other Admission 0.04(0-0.2)0(0-0.3)0.006")
23
Estimated Savings on primary care costs/resource utilisation audit

24
Estimated Savings on Hospital Resource Utilization Secondary care costs Mean number of appointments/ad missions saved (per pt/year) Estimated Savings per 100 patients/year Diabetes Consultant Appointments ( £ 88) 1.44 £ 12,672 ( € 18 881) Diabetes Admissions: If hypoglycaemic emergency ( £ 757) If midpoint of scale ( £ 1932.50) 0.132 £ 9,992 ( € 14 888) £ 25,509 ( € 38 008) Primary Care Costs (assuming tarrif £ 88) 6.52 £ 57,400 ( € 85 526)
 Estimated Savings per 100 patients/year Diabetes Consultant Appointments ( £ 88) 1.44 £ 12,672 ( € ) Diabetes Admissions: If hypoglycaemic emergency ( £ 757) If midpoint of scale ( £ ) £ 9,992 ( € ) £ 25,509 ( € ) Primary Care Costs (assuming tarrif £ 88) 6.52 £ 57,400 ( € )")
25
Practical Lessons CSII has resource benefits as well as costs CSII has resource benefits as well as costs Benefits occur in primary and secondary care Benefits occur in primary and secondary care Demonstrating these benefits strengthens the case for continued funding of the pump programme Demonstrating these benefits strengthens the case for continued funding of the pump programme We cannot say whether the same outcomes would apply with wider usage of CSII We cannot say whether the same outcomes would apply with wider usage of CSII This is not a randomised trial only observational data This is not a randomised trial only observational data

26
Conclusions: Who should access pump therapy? When there is clinical benefit When there is clinical benefit Definition of benefit Definition of benefit When the resources allow When the resources allow Definition of cost effectiveness Definition of cost effectiveness Effects of Insulin Pump Therapy on Local Healthcare Resource Utilisation of Insulin Pump Therapy T Ulahannan, N Myint, KF Lonnen submitted Effects of Insulin Pump Therapy on Local Healthcare Resource Utilisation of Insulin Pump Therapy T Ulahannan, N Myint, KF Lonnen submitted

27
Acknowledgements Kathryn Lonnen Kathryn Lonnen Nyo Nyo Myint Nyo Nyo Myint Wilma Ross Wilma Ross Fiona Davies Fiona Davies Sian Webb Sian Webb Jhansi Kamalkrishnan Jhansi Kamalkrishnan Irene Stewart Irene Stewart

Similar presentations





 Structured education programme for patients with insulin requiring.>")


 Consultant in Community Geriatric Medicine & Health Foundation/Institute.>")


>")








