Download presentation
Presentation is loading. Please wait.

1
Dr Adrian Banning, The John Radcliffe, Oxford Drug eluting stents for in-stent restenosis

2
Case Presentation (1) 44-year old man August 2001 –presents with Unstable Angina, –severe LAD stenosis. Direct stent - 3.5x15 NIR Elite October 2001: –recurrent angina, –severe stenosis just proximal to the stent. – 3.5x8 Express, partially overlapping the first April 2002: –recurrent angina - diffuse in-stent restenosis. CABG with LIMA->LAD

3
Case Presentation August 2001 stent October 2001: stent April 2002: CABG with LIMA->LAD, June 2002 –Recurrent angina –Management? –Exercise test on treadmill?

5
Case Presentation (2) August 2002: –cath - failed LIMA graft- –enrolled in a multicenter registry (non-polymeric paclitaxel DES at concentration of 3.0 µg/mm2 DELIVER II ) –2 “Achieve” stents 3.5x18 and 3.5x23 mm in the mid LAD Entire previously stented segment was covered –Optimized with high-pressure 3.5 mm NC balloon, no IVUS
 August 2002: –cath - failed LIMA graft- –enrolled in a multicenter registry (non-polymeric paclitaxel DES at concentration of 3.0 µg/mm2 DELIVER II ) –2 Achieve stents 3.5x18 and 3.5x23 mm in the mid LAD Entire previously stented segment was covered –Optimized with high-pressure 3.5 mm NC balloon, no IVUS")
6
Case Presentation (2) August 2002: –cath - failed LIMA graft- –enrolled in a multicenter registry (non-polymeric paclitaxel DES at concentration of 3.0 µg/mm2 DELIVER II ) –2 “Achieve” stents 3.5x18 and 3.5x23 mm in the mid LAD Entire previously stented segment was covered September 2003 (13 months) recurrent angina –Further angiogram –5 th in 22 months
 August 2002: –cath - failed LIMA graft- –enrolled in a multicenter registry (non-polymeric paclitaxel DES at concentration of 3.0 µg/mm2 DELIVER II ) –2 Achieve stents 3.5x18 and 3.5x23 mm in the mid LAD Entire previously stented segment was covered September 2003 (13 months) recurrent angina –Further angiogram –5 th in 22 months")
7
September 2003 PRE-INTERVENTION

8
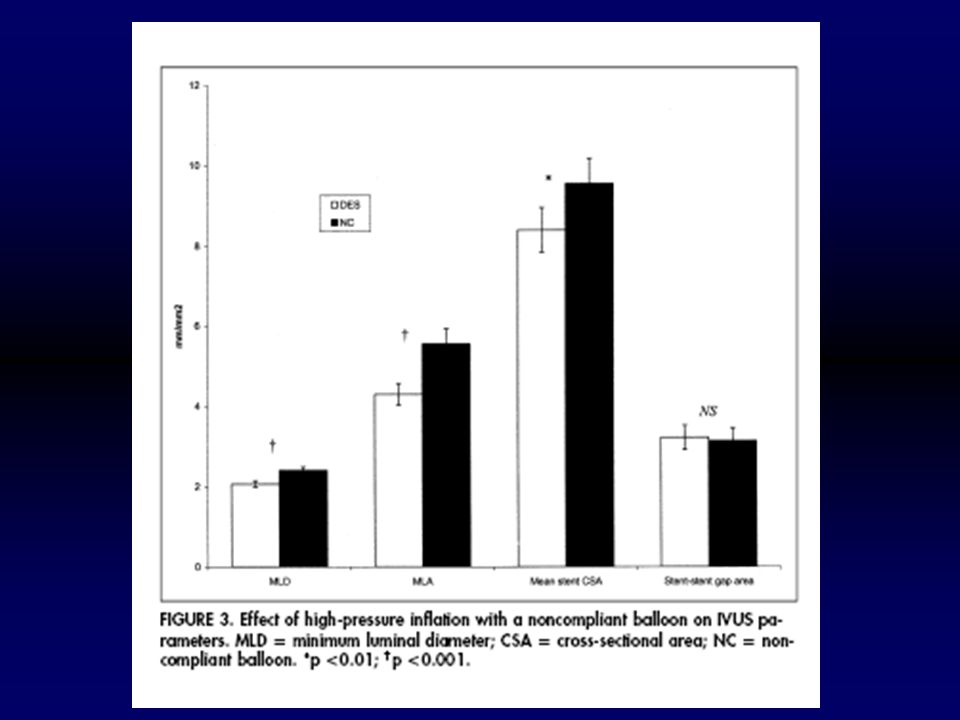
September 2003 Intervention number 4 –IVUS guidance Cypher 3.0x23 and 3.0x23 covering all the previously stented segment with overlap. 3.5 NC balloon multiple inflations (up to 24 atm) –IVUS used to check MLA>5 mm2
 –IVUS used to check MLA>5 mm2.")
9
September 2003 POST-INTERVENTION

10
April 2004 (8 months post) FOLLOW UP
 FOLLOW UP")
11
April 2004 (8 months post) FOLLOW UP
 FOLLOW UP")
12
What is “in stent restenosis” Densely packed neointima mainly VSMC and matrix Like a keloid scar Not atheroma

15
The pre-DES era

16
Treatment modality does not matter

17
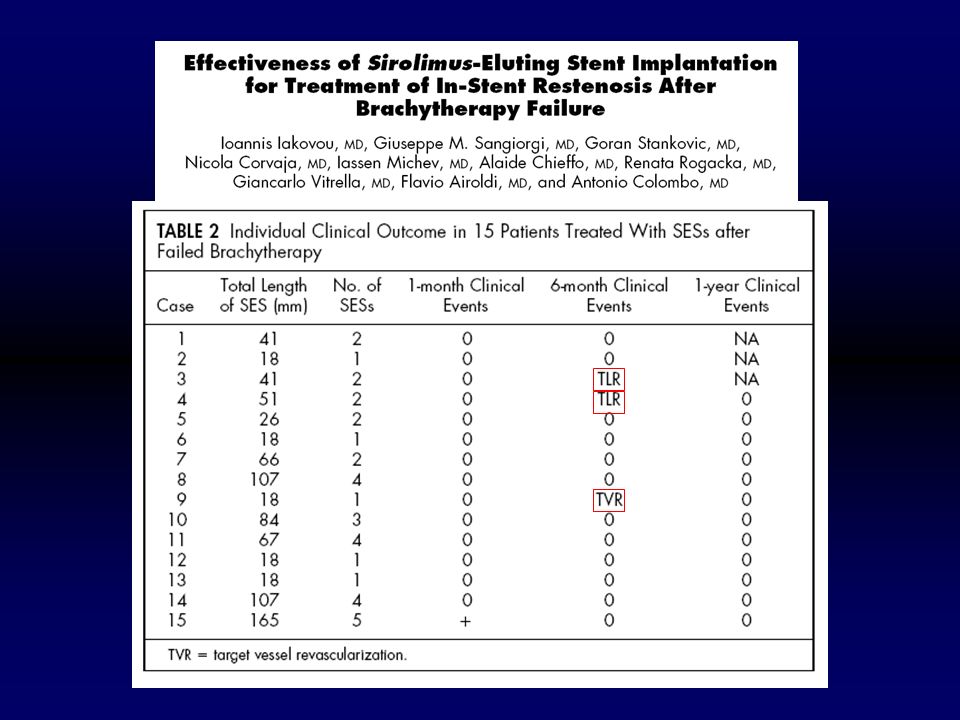
Vascular brachytherapy good short term results

19
DES era: a bad start

20
Data from registries

21
Cypher stent: Brazilian and Dutch experience

22
Long term follow-up

23
QCA data: late catch up?

24
IVUS data: reassuring

28
SECURE registry

29
Recurrent ISRNo Rec. ISRp MLA <5mm2 9/115/190.003 MLA <4mm2 7/114/190.02 MLA <3mm2 4/111/190.03 Stent underexpansion is still important !!!

31
Sequential IVUS analysis of lumen and stent dimensions

35
Practical tips for treating ISR Prevent ISR using DES or properly expanded BMS! –much less diffuse ISR When treating ISR –Use preinflation/cutting balloon –Cover the whole stented segment with generous margins –IVUS guidance (mandatory for DES failure) –Optimally expand both stents with NC balloons
 –Optimally expand both stents with NC balloons.")
36
Conclusions DES can treat ISR as well (and probably better than) any other modality –including brachy and surgery!! Definitive trials will be published shortly Radiotherapy has a limited role in the future

37
TOO much radiation is bad for you

38
Even a little radiation can be bad for you! And who is that young man?

39
Don’t know but……

40
More pictures on SexyDrRobCrook.com.uk

41
Thank you The end

43
Ongoing studies

46
Final result does

Similar presentations














 Trial Presented at The American College of Cardiology Scientific Session.>")




 study with the Sirolimus coated BX™ VElocity balloon expandable stent (CYPHER™)>")











