Download presentation
Presentation is loading. Please wait.

1
Rheumatology Back to Basics Dr. Doug Smith

2
Immune Mechanisms of Disease Type I:Anaphylactic IgE eg. asthma Type II: Cytotoxic eg. AIHA Type III: Immune Complex eg. SLE Type IV: Cell-mediated/Delayed Hypersensitivity: T-cells eg. Contact dermatitis

3
HLA: Disease Associations HLA B27 (MHC Class I) - Ankylosing Spondylitis - Reiter’s - Psoriatic arthritis - IBD arthropathy HLA DR4, DR1 (MHC Class II) - RA HLA DR3 (MHC Class II) - SLE, Sjogren’s, Type I DM…
 - Ankylosing Spondylitis - Reiter’s - Psoriatic arthritis - IBD arthropathy HLA DR4, DR1 (MHC Class II) - RA HLA DR3 (MHC Class II) - SLE, Sjogren’s, Type I DM…")
4
Rheumatoid Factor Anti-antibodies (Fc domain of IgG) Rheumatoid Arthritis: - sensitivity = 70% - poor prognosis - extra-articular features Non-specific: - other rheumatic diseases eg. Sjogren’s - chronic inflammatory diseases - chronic infections – SBE, Hep C - 10-20% over age 65

5
Antinuclear Antibodies SLE: sensitivity = 90% + Specificity low: - other autoimmune dis., - family members - drugs...

6
Other Autoantibodies Anti-DNA (native, double-stranded) - SLE- sensitivity 60-70% - specificity ~ 100% - correlate with disease activity Anti-SSA, SSB (Ro, La) - Sjogren’s, SLE - congenital complete heart block
 - SLE- sensitivity 60-70% - specificity ~ 100% - correlate with disease activity Anti-SSA, SSB (Ro, La) - Sjogren’s, SLE - congenital complete heart block")
7
Antiphospholipid Antibodies Anticardiolipin antibodies Lupus anticoagulant Associations: - thrombosis - recurrent pregnancy losses - thrombocytopenia SLE, other CTD’s, primary

8
Anti-Neutrophil Cytoplasmic Antibodies (ANCA) Patients with suspected vasculitis - pulmonary/renal syndromes cANCA: Wegener’s Granulomatosus: - 80% sensitive and specific pANCA: less specific
 Patients with suspected vasculitis - pulmonary/renal syndromes cANCA: Wegener’s Granulomatosus: - 80% sensitive and specific pANCA: less specific")
9
Osteoarthritis (OA) The most common type of arthritis > 5 million Canadians Disease of cartilage (cf. RA) Characterized by: - Cartilage degradation, loss - hypertrophic bone formation (osteophytes...
 Characterized by: - Cartilage degradation, loss - hypertrophic bone formation (osteophytes....")
10
Primary (idiopathic) OA Peripheral Joints: - hands- DIP, PIP (cf. RA) - 1st C-MC - feet - 1st MTP - large weight-bearing joints - hips, knees Spine- apophyseal joints - intervertebral discs
 - 1st C-MC - feet - 1st MTP - large weight-bearing joints - hips, knees Spine- apophyseal joints - intervertebral discs.")
11
OA: Heberden’s (DIP) Bouchard’s (PIP) Nodes
 Bouchard’s (PIP) Nodes")
12
Osteoarthritis: X-ray 1st C-MC Joint Joint space narrowing Subchondral sclerosis Osteophytes

13
Rheumatoid Arthritis Prevalence 1:100 small joint, symmetric polyarthritis + AM stiffness chronic (>6weeks) Path = synovial inflammation extraarticular features
 Path = synovial inflammation extraarticular features")
15
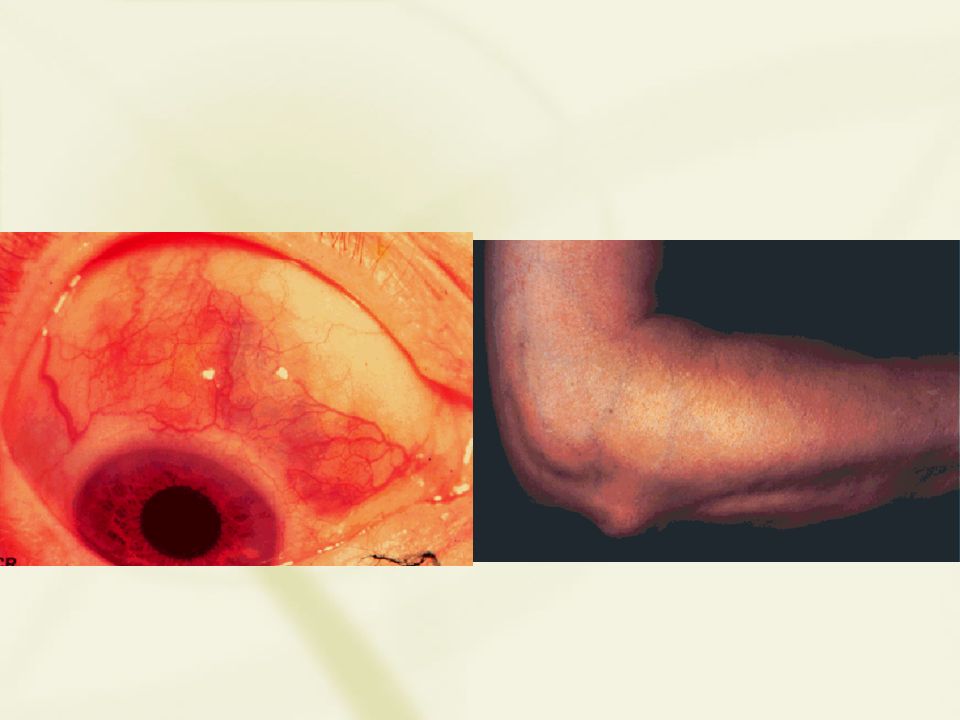
RA: Extra-articular features Skin - sc nodules, vasculitis... Eyes - sicca, scleritis, episcleritis Lungs - pleurisy/effusion, interstitial fibrosis, nodules Cardiac - pericarditis, nodules Hematologic - anemia, Felty’s Neurologic - peripheral neuropathy...

17
RA: Factors Associated with Poor Prognosis Rheumatoid factor positivity HLA-DR4 haplotype Degree of disease activity at onset … Early aggressive therapy

18
RA: Treatment Symptomatic - rest, education - splints, orthotics - ASA, NSAID’s, Coxibs (???) Disease Modifying Anti-Rheumatic Drugs (DMARDs)
 Disease Modifying Anti-Rheumatic Drugs (DMARDs)")
19
RA: Common DMARD’s Methotrexate Hydroxychloroquine Sulfasalazine New Biologics...

20
RA: New Therapies - Biologics anti-TNF soluble TNF receptor Interleukin 1 Receptor Antagonist (IL-1RA) Concerns:- cost - parenteral - risk of infections, TB
 Concerns:- cost - parenteral - risk of infections, TB")
21
Lupus Prevalence 1:2000 1:350 young black females 9:1 female: male broad spectrum: skin systemic

22
SLE: Classification Criteria 1. Malar Rash 2. Discoid Rash 3. Photosensitivity 4. Oral ulcers 5. Arthritis 6. Serositis 7. 7. Renal 8. 8. Neurologic 9. 9. Hematologic 10. 10. Immunologic 11. 11. ANA

23
SLE: Clinical Features at Presentation Arthralgia/arthritis55% Skin 20% Nephritis5% Fever 5% Other15%

24
Lupus: Arthritis (80-90%) Migratory Non-Erosive Deformities (10%)
 Migratory Non-Erosive Deformities (10%)")
25
Lupus : Skin (70%) Butterfly rash Discoid rash plaques Photosensitive
 Butterfly rash Discoid rash plaques Photosensitive")
26
Lupus: Treatment Sunprotection, sunscreens ASA, NSAIDs Antimalarial drugs Steroids Immunosuppressants

27
Scleroderma Disorder of: - small blood vessels = SPASM, ischemia + - overproduction of connective tissue (collagen) = FIBROSIS
 = FIBROSIS")
28
Scleroderma: Types Systemic - Diffuse - Limited (CREST) Localized- morphea - linear scleroderma
 Localized- morphea - linear scleroderma")
29
Scleroderma: Antibodies ANA: common Systemic - Diffuse: anti-topoisomerase(Scl-70) - Limited (CREST): anti-centromere Localized: none
 - Limited (CREST): anti-centromere Localized: none")
30
Scleroderma: Systemic Vascular: Raynaud’s telangiectasias Skin: swelling, thickening, tightening Esophagus: reflux, strictures… Lungs: - Pulmonary fibrosis - Pulmonary hypertension Kidneys: - hypertension, renal failure - esp. Diffuse

31
Raynaud’s phenomenon Triggers: cold, stress 3 phases: white blue red 8-10% of normals 90% - scleroderma

32
Scleroderma: kidneys Patients with diffuse disease Usually in first few years of disease Hypertension, renal failure Treatable/reversible! - ACE inhibitors

33
Limited Scleroderma (CREST) Calcinosis Telangiectasias
 Calcinosis Telangiectasias")
34
Acute Inflammatory Monoarthritis Infections Spondyloarthropathies Crystals

35
Synovial Fluid Testing Cell count, differential WBC: 200-2000 = non-inflammatory 2000-100,000 = inflammatory >75,000 = septic Gram stain, C&S Crystals

36
Spondyloarthropathies 1. Ankylosing Spondylitis 2. Reiter’s/reactiv e arthritis 3. Psoriatic arthritis 4. Inflammatory Bowel Disease Axial and/or peripheral joints HLA-B27 Path = enthesopathy Inflammatory back pain Extra-articular: - uveitis etc. RF negative

39
Reiter’s Syndrome

40
HLA-B27: Disease Associations Ankylosing Spondylitis>90% Reiter’s syndrome/ reactive 80% Inflammatory bowel disease 50% Psoriatic Arthritis - with spondylitis 50% - with peripheral arthritis 15% Caucasians 8% Inuit25%

41
Gout Acute monoarthritis - lasts days - recurrent attacks Uncontrolled hyperuricemia tophi polyarthritis

42
Gout: uric acid crystals Needle-shaped Strong negative bireringence Phagocytosed by PMN’s

43
Gout: Treatment Asymptomatic hyperuricemia none Acute attack- NSAID’s - colchicine - steroid’s Indications to lower uric acid - allopurinol - renal stones - frequent attacks - tophi

44
Pseudogout - CPPD Acute monoarthritis Knees, wrists Chondrocalcinosis Pyrophosphate crystals: - rhomboid - weak positive birefringence

45
Vasculitis: Classification Small Vessel Hypersensitivity Medium Vessel: - necrotizing = Polyarteritis nodosa - granulomatous = Wegener’s Large Vessel: - Giant Cell (Temporal) arteritis - Takayasu’s (Aortic Arch Syndrome)
 arteritis - Takayasu’s (Aortic Arch Syndrome)")
46
Giant Cell Arteritis (GCA) Age >50 years - mean = 70 years Symptoms related to arteries: - headache, scalp tenderness - visual loss - jaw claudication
 Age >50 years - mean = 70 years Symptoms related to arteries: - headache, scalp tenderness - visual loss - jaw claudication")
47
Giant Cell (Temporal) Arteritis
 Arteritis")
48
Diagnosis: - CBC - anemia of chronic disease - ESR - markedly elevated, often >100 - Biopsy temporal artery Treatment: URGENT! (prevent visual loss) - steroids - prednisone 60mg daily...
 - steroids - prednisone 60mg daily....")
49
Toxicity: ASA and NSAIDs GI renal CNS platelet effects contraindicated ASA hypersensitivity avoid if possible - pregnancy and lactation

50
Cox-2 “specific” Inhibitors (coxibs) improved GI safety no effect on platelets efficacious in RA, OA, pain X ?? Increased risk MI, stroke X renal effects like other NSAID’s caution!- elderly - hypertension - cardiac disease - renal disease

Similar presentations






>")
 25 th Nov 2013.>")
,FRCPLondon,FRCP Edin, FACP Rheum CONSULTANT RHEUMATOLOGIST Aut Even Hospital, Kilkenny Whitfield Clinic Waterford,The St.>")













